
1. Introduction
Compared to surgical procedures, radiation, or chemotherapy, drug therapy offers a relatively safer and less burdensome approach to treating tumors. Moreover, there is an ongoing and dedicated effort to discover and develop new drugs [1,2,3]. In the past, the effectiveness of drugs was predicted through in vitro cytological analysis and various animal disease models. However, these models failed to accurately simulate the complex mechanisms involved in tumor pathology and the heterogeneity of tumors among patients, resulting in inaccurate predictions of drug efficacy [4]. To address this issue, cell line models, including two-dimensional (2D) cultures of cancer cell lines and cancer cell line-derived xenografts (CDX), have been established for drug discovery and screening. However, compared to cancer cells in the in vivo tumor tissue, cells cultured in 2D display flattened morphologies that limit their ability to capture aspects of tumor heterogeneity and important signaling networks [5,6]. Additionally, long-term culture of cancer cell lines in vitro is known to introduce genetic mutations and epigenetic modifications, which can alter cellular responses to drugs [7]. Therefore, there is an urgent need for new approaches to drug development and screening that take into account tumor heterogeneity. Personalized drug therapy has emerged as a promising approach that considers the genetic information and disease heterogeneity of individual patients. It aims to predict the effects and side effects of drugs, thereby improving treatment efficacy [8]. However, most methods for predicting therapeutic response in cancer primarily rely on molecular analysis of the tumor, which may lack sufficient accuracy. Considering these factors, incorporating in vitro animal models to assess treatment response could significantly enhance the effectiveness of personalized drug therapy. Patient-derived preclinical cancer models, including PDX, CTC-derived models, and tumor organoids-on-chip, have emerged as valuable tools for personalized drug therapy by closely resembling the physiological and clinical characteristics of patients’ native tumors [4]. Each of these models has a distinct preference for different types of patient tumors, such as solid tumors, metastatic tumors, or advanced-stage tumors. Furthermore, each model has its own advantages and limitations in terms of drug discovery, delivery, and screening. However, most reviews have focused solely on discussing the application and development trends of specific models without providing a comprehensive comparison of preclinical tumor models. In this review, we aim to summarize the establishment and progress of PDX, CTC-derived models, and tumor organoids-on-chips. We will highlight their unique applications in drug discovery, sensitive testing, and screening, providing valuable suggestions and guidance for selecting appropriate models for specific tumor types and clinical trials.
2. PDX models from solid tumors for drug delivery and metabolism
Traditional cell-line derived xenograft (CDX) models have contributed to our understanding of cancer development and drug mechanisms, but they have limitations such as lack of tumor heterogeneity and inappropriate microenvironment. In contrast, PDX models are generated by implanting biopsy or surgical tumor specimens from patients into immunodeficient mice, offering a more personalized approach to drug therapy [9]. Once established, PDX models can be directly examined in situ at the original graft site or serially transplanted by harvesting and re-transplanting a portion of the initial graft into subsequent host mice [5]. These models provide a more accurate representation of the tumor biology and heterogeneity of individual human cancers compared to CDX models. In addition, when treated with drugs, PDX models demonstrate clinical outcomes consistent with those observed in the corresponding patient donors. Thus, PDX models derived from solid tumors offer significant advantages in studying drug delivery and metabolism, providing a more clinically relevant platform for personalized drug therapy research.
1. The development of PDX models
The generation of patient-derived xenograft (PDX) models dates back to the pioneering work of Ragaard and Povlsen, who successfully transplanted human colonic tumor tissue into nude mice at the Municipal Hospital, University of Copenhagen in 1969 [6]. Subsequently, in 2006, Hidalgo and his colleagues made significant advancements in the field by utilizing NOD-SCID mice (non-obese diabetes-severe combined immunodeficiency), which greatly improved the success rate of PDX models [10]. This breakthrough led to the widespread acceptance and extensive utilization of PDX models by research groups, academic institutions, and pharmaceutical companies in the early 21st century. The contributions made by Hidalgo and his colleagues in enhancing the success rate of PDX models through the use of NOD-SCID mice have had a profound impact on the field of cancer research. Their pioneering work has opened up new avenues for studying the biology of human tumors and evaluating potential therapeutic approaches in a more clinically relevant setting. As a result, PDX models have become an invaluable tool for researchers and drug development teams in their quest for improved cancer treatments.
2. The construction and application of the PDX model
The generation of patient-derived xenograft (PDX) models involves the transplantation of patient tumor tissue into immunodeficient mice. This can be done through orthotopic transplantation, where the patient tumor samples are transplanted into the corresponding tissue or organ in mice. Alternatively, heterotopic transplantation involves transplanting the tumor samples into a different tissue or organ in mice, typically under the skin [9]. Both orthotopic and heterotopic transplantation methods are commonly employed in cancer treatment studies. However, it is important to note that mice differ significantly from humans in terms of their genetic and immune systems. Therefore, studying the unique immune responses in humans using mice models alone can lead to unsatisfactory predictions of personalized drug treatments. To address these species-specific differences, researchers have developed “humanized” mice or “human immune system” (HIS) mice, which involves transplanting human cells or tissues into immunodeficient mice. This allows for in vivo preclinical studies that more closely mimic the human immune response [9]. Table 1 provides an overview of the commonly used methods for constructing humanized mice.
Table 1. Establishment of humanized immune system mouse models. |
| Humanized models | Mouse strain | Establishment method | Ref |
|---|---|---|---|
| Hu-PBL-SCID mice model | SCID mice | Perihperal blood lymphocyte (PBL) cells were injected intraperitoneally or intravenously into non-irradiated or sublethal irradiated mice | [83,84] |
| Hu-HSC(Hu-SRC-SCID) mice model | NOD-SCID mice, NSG mice | 1. Human CD34+ hematopoietic stem cells (HSC) were injected into neonatal or adult immunodeficient recipient mice by intravenous injection or bone marrow cavity injection | [84,85,86] |
| 2. Human hematopoietic stem cells were intrahepatic injected into neonatal NSG or NOG-SCID mice irradiated with sublethal amounts to obtain good human cell transplantation and generate T cells, B cells, macrophages, NK cells and DC cells | |||
| Human BLT (bone marrow, liver, thymus) model | NOD-SCID mice, NSG mice | NOD/SCID mice irradiated with sublethal doses were transplanted with human embryonic thymus and embryonic liver tissue under the renal capsule, and CD34+HSCs were isolated from homologous embryonic liver by tail vein injection to construct a new humanized mouse model | [84,87,88] |
The utilization of humanized mice in conjunction with PDX models offers a more comprehensive approach to studying cancer treatments and understanding human-specific immune responses. Incorporating these technologies into preclinical research can improve the prediction and evaluation of personalized drug therapies for cancer patients. Fig. 1 illustrates the extensive applications of PDX models in cancer research. These applications encompass a wide range of investigations, including the exploration of fundamental biological mechanisms, identification of biomarkers indicative of treatment response and resistance, and the conduct of translational research. PDX models play a crucial role in drug discovery by allowing for preclinical evaluation of therapeutic agents and facilitating the exploration of novel drug combinations. Furthermore, PDX models have significant value in combination clinical trials, where the model is treated with the same treatment protocol as the original patient tumor. This approach enables a direct assessment of the PDX model's response, thereby providing additional insights into the accuracy and predictive capabilities of the model. Overall, the versatility of PDX models in cancer research makes them invaluable tools for gaining deeper insights into the underlying biology of cancer, evaluating treatment efficacy, and identifying potential therapeutic strategies for personalized medicine.
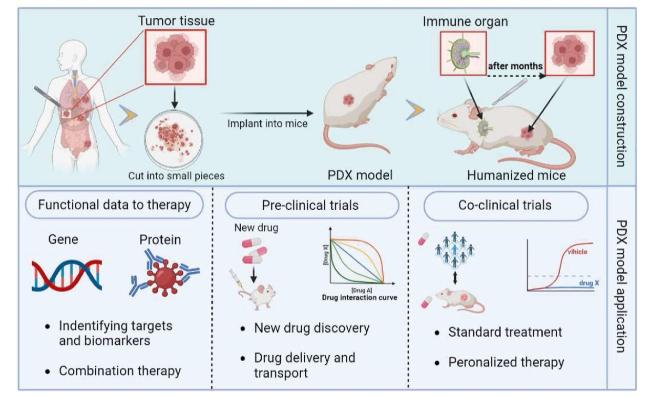
Fig. 1. Diagram showing the construction and application of the PDX models. |
3. Assesing drug delivery and metabolism by PDX models constructed from solid tumors
Preclinical tumor models play a pivotal role in various aspects of new drug discovery, efficacy testing, drug delivery, and drug metabolism studies. These models provide valuable insights and predictions regarding the effectiveness of anticancer drugs to a certain extent. In comparison to other preclinical tumor models, patient-derived xenograft (PDX) models and humanized mouse PDX models offer distinct advantages. They allow for the investigation of drug delivery and metabolism dynamics over time, providing a more comprehensive understanding of how drugs interact with tumors in vivo. This information is crucial for optimizing drug dosing regimens and assessing their efficacy in clinical settings. By utilizing PDX models, researchers can simulate the complexities and heterogeneity of human tumors, enabling more accurate assessments of drug response and potential treatment outcomes. Humanized mouse PDX models, on the other hand, provide an additional layer of relevance by incorporating a human immune system, allowing for the evaluation of immunotherapies and the study of immune-tumor interactions. Overall, the use of PDX models and humanized mouse PDX models offers significant advancements in the exploration of drug delivery, metabolism, and the clinical assessment of drug dosing and efficacy. These models bridge the gap between preclinical studies and clinical applications, ultimately facilitating the development of more effective and personalized cancer treatments.
2.1. Application of PDX model in drug delivery
Translating promising in vitro drug efficacy into successful in vivo treatment can be challenging. The diluted drug doses, circulation and metabolism within the body, and the presence of barriers can limit the achievement of effective therapeutic concentrations at the target site. Delivering drugs effectively to the therapeutic target while minimizing disruption of normal physiological functions is an ongoing concern for researchers. PDX models have emerged as a valuable tool in exploring effective drug delivery systems, allowing researchers to evaluate various drug delivery strategies and systems. This includes nanoparticle-based drug delivery systems, liposomes, micelles, polymer-based systems, targeted drug delivery systems, and other innovative approaches. By studying the behavior and efficacy of these drug delivery systems in PDX models, researchers can gain insights into their potential for successful translation to human clinical trials.
In the past decade, nano drug delivery systems have been highly valued for their potential to overcome drug resistance, improve solubility, reduce adverse effects of chemotherapeutic drugs and control release of therapeutic agents [11]. The application of PDX model in nano-drug delivery system is mainly to simulate in vivo biodistribution, targeting specific sites and simulating barrier system. Chen's team designed a dual-responsive copolymeric nanoparticles to encapsulate bortezomib (BTZ), a protease inhibitor, to solve the problems of drug resistance, poor stability, and high toxicity when administered alone [12]. In this study, a gallbladder cancer PDX mouse model was used to evaluate the biodistribution, targeting ability and controlled drug release ability of the developed nanodrug delivery system, which is a classic application of PDX in nanodrug delivery system. The patient-derived PDX model not only inherits some specific characteristics of the patient's tumor, but also has the unique barrier function in vivo, which can be used to simulate some tumors in special locations. Glioblastoma multiforme (GBM) is a highly aggressive intracranial tumor, and chemotherapy drugs is severely limited by poor drugs penetration due to the blood-brain barrier (BBB). To solve this problem, Lu's team designed a biomimetic nanoparticle system that can cross the BBB and target GBM cells for therapeutic effects. In this study, surgically resected tumor tissues from GBM patients were subcutaneously and orthotopically transplanted into mice to evaluate the ability of their constructed biomimetic nanoparticle system to penetrate the BBB and target tumors [13]. This is one of the applications where the PDX model simulates the in vivo barrier system to confirm that nanoparticles can successfully deliver drugs to the therapeutic site.
Apart from nano-drug delivery systems, PDX model has also been applied to a variety of other drug delivery systems, including liposomes, hydrogels, antibody-drug coupling systems, and engineered exosome systems. PDX models enable the assessment of drug accumulation, penetration, and distribution within the tumor microenvironment. They also offer the ability to evaluate the impact of drug delivery systems on tumor growth, metastasis, and therapeutic response. This information can guide the development of strategies to improve drug delivery to the target site and enhance treatment outcomes. In summary, PDX models serve as a valuable platform for investigating and optimizing drug delivery systems. By utilizing these models, researchers can gain a deeper understanding of how drugs interact with tumors in vivo and develop more effective strategies to deliver drugs to the therapeutic target, ultimately improving the efficacy and success of cancer treatments.
2.2. Assessing drug metabolism by PDX models
PDX models are also widely used in the study of drug metabolism in personalized medicine therapy. Pharmacokinetics refers to the movement and modification of medication inside the body. Once the medication get administered, it first has to be absorbed into circulation, then distributed to various tissues throughout the body, metabolized or broken down; and finally, eliminated or excreted in the urine or feces [14]. Therefore, under most conditions, the PDX model is used to explore how metabolic reactions transform active drugs into less active or inactive metabolites. One study used the PDX model of pancreatic cancer to quantitatively characterize the effect of dexamethasone blood concentration on tumor growth inhibition [15]. The pharmacokinetic/pharmacodynamic model was established in the PDX mice model, and the mathematical relationship between dexamethasone blood concentration and tumor growth dynamics was established, demonstrating the feasibility of dexamethasone in the treatment of pancreatic cancer [15]. It is common to establish pharmacokinetic-pharmacodynamics models in PDX models to explore the anti-tumor effects of drugs. The conventional method is to set up different concentrations of drugs and different duration of administration, and observe and test the optimal antitumor activity of drugs through PDX model, so as to further develop the appropriate dose of drugs for human.
The PDX model transplanted tumors from patients into immunodeficient mice, which retained the heterogeneous characteristics of tumors and greatly improved the efficiency of personalized drug therapy. PDX models are not only indispensable for drug delivery systems and pharmacokinesis-pharmacodynamic studies, but also play an important role in drug development, screening, testing, and evaluation.
3. CTC models derived from advanced-stage patients for personalized drug testing
1. Strategies for enrichment and detection of CTCs
The circulating tumor cell (CTC) is single tumor cell or tumor mass that shed from a patient's tumor lesion and enter the circulation system [16,17]. Clinically, CTC, as a form of liquid biopsy, possess safe and noninvasive advantages over traditional tissue biopsy and can be used to monitor the cancer progression and treatment response in real time [18]. However, the tiny minority of CTC in the blood, with 1-10 cells per 10 ml of blood that far less than billions of blood cells and a short half-life about 1-2.4 h, limit the application of CTC extremely [19,20]. Various techniques have been developed in recent years to effectively isolate, identify, and amplify CTC, as shown in Fig. 2.
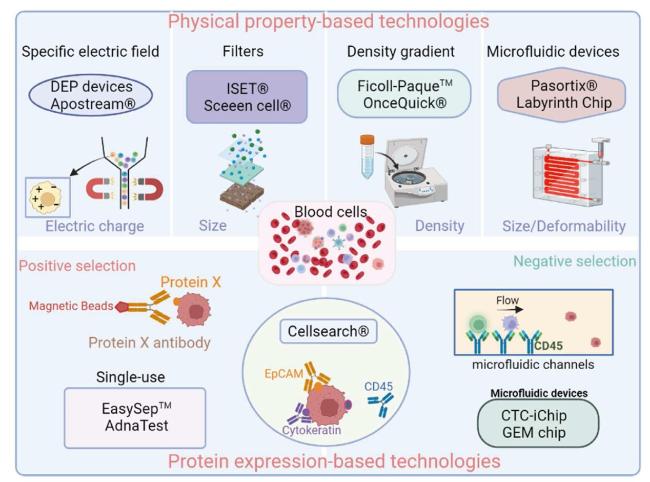
Fig. 2. Circulating tumor cell (CTC) enrichment techniques. |
Most of the enrichment methods of CTC are based on biological properties such as cell-surface markers and physical characteristics such as electric charge, size, density, deformability [21,22]. And those methods are usually combined with detection techniques including immunofluorescence, immunohistochemistry to identify CTC [23,24]. Among most commonly used biologically-based technology is the CellSearch system (Menarini-Silicon Biosystem, Bologna, Italy), it is the exclusive technology approved by the US Food and Drug Administration (FDA) to assist prognosis for patients with metastatic breast, prostate, and colorectal cancer [19,25,26,27]. CTC is obtained by EpCAM (epithelial cell adhesion molecule)-coated immunomagnetic beads in CellSearch system. Then, detection of CTC by fluorescent using anti-cytokeratinsms (CK 8, CK 18, CK 19), anti-CD45 (leukocyte marker) [28]. Physical property-based methods including filtration systems have been developed to capture CTC based on their large size compared to leukocytes, notably the ISET® (Isolation by Size of Tumor Cells) (RareCells Diagnostics, Paris, France) [29] and the ScreenCell® (Paris, France) [30] methods, which are able to detect CTC using microporous polycarbonate filters. In addition, a variety of technologies based on physical or biological properties, or both, have been discovered and developed. In fact, there are no techniques which can fully respond to the phenotypic heterogeneity of CTC, and each method has its own advantages and limitations. However, the existing CTC-enrichment technology can be used to establish CTC-driven patient models, so as to achieve rapid drug discovery and efficacy testing in advanced patients [31].
2. Ex Vivo and xenografts models derived from CTCs
The metastatic spread and resistance to treatment are the leading causes of death in patients with advanced cancer [32]. CTCs are considered to be the “seeds” of tumor metastasis by dissociating from primary tumors into the circulatory system, flowing with the blood and colonizing distal tissues and organs [33]. Therefore, to explore the mechanism of tumor metastasis and cell functional characteristics through CTC is very important for drug discovery and evaluation in the treatment of advanced patients [34,35]. CTC-driven cell models and animal models have been constructed and used in the research of cancer mechanism and personalized treatment of patients.
CTC-derived Ex Vivo model was constructed by the isolation of CTC from patients' blood and amplification culture in vitro [36]. For reproducible studies, especially to characterize behavior, expansion into stable cell lines is a preferable choices [37,38]. In the past decade, many attempts have been made to propagate CTC from clinical patient blood through ex vivo culture, but most showing a short-term culture time, lasting from 3 days to 14 days [37]. Only a few long-term cultures shown in Table 2, what have reported successfully established CTC lines with demonstrated immortality.
Table 2. CTC cell lines in recent 5 years. |
| Cell Line | Type of Cancer | Culture Period or Passage | Specific Characteristics | Ref. |
|---|---|---|---|---|
| CTC-MCC-41 CTC- MCC-41.4 CTC-MCC-41.5 (A-G) | Colon cancer | Several cell lines from the same patient at different times (9 cell lines) | ALDH1 CD44 panCD66 EpCAM | [89] |
| CTC-TJH-01 | Non-small cell lung cancer | 24 months | CXCL5 CD44 ALDH1 | [90] |
| CTC-ITB-01 | Breast cancer | >4 years | E-Cadherin EpCAM K19 CD24 Twist 1 | [48] |
| UWG01CTC, UWG02CTC | Gastroesophageal cancer | >12 months | EpCAM(+) CK(+) CD44 E-Cadherin | [91] |
| EMC-Pca-41 | Prostate cancer | >1 year, 10 passages | TMPRSS2-ERG fusion loss of PTEN | [92] |
| Mel-167 PEM-22 Mel-182 PEM-78 | Melanoma | N/A | BRAF-mutant NG-2 MLANA | [93] |
CTC-derived xenografts models are generated by implanting isolated CTC into immunodeficient mice [39]. In 2013, Baccelli and colleagues first detected bone, lung, and liver metastases in 6 recipient mice by injecting CTC isolated from patients with luminal breast cancer into immunodeficient mice [40]. Later, Pereira and colleagues constructed the first triple-negative CDX model of circulating tumor cells in breast cancer. Briefly, they obtained 969 CTCs and 74 CTCs clusters of triple negative breast cancer CTCs by cellSearch isolation and injected the enriched CTCs subcutaneously into nude mice, and finally obvious tumors were observed after 5 months culture [41].
Recently, various CTC-Derived Xenografts Models (as Table 3) have been successfully constructed. These data describe functional CTCs and related markers that could help develop more effective tools for tumor diagnosis and treatment.
Table 3. CTC-Derived Xenografts Models. |
| Type of Cancer | Model | Main findings | Ref. |
|---|---|---|---|
| Breast cancer | Dilution in Matrigel subcutaneous injection to node mice | Wnt pathway upregulation may be a potential therapeutic target in TNBC | [41] |
| Melanoma | Dilution in Matrigel subcutaneous injection into NOD.Scid IL2γ (NSG) mice | recapitulation of patient response to dabrafetinib in the CDX | [94] |
| SCLC | Dilution in matrigel/subcutaneous into NOD/SCID gamma (NSG) mice | ·1. Recapitulation of CTC genomic profile by CDX tumors | [79] |
| ·2. CDX mimicked donor's response to chemotherapy | |||
| Short-term non-adherent vivo cell cultures | Recapitulate genomic landscape and in vivo drug response | [95] | |
| NSCLC | Dilution in matrigel/subcutaneous into female CB-17/lcrHsd-PrkdcscidLystbg-J (SCID-bg) mice | Importance of mesenchymal CTCs with tumorigenic capacity | [96] |
3. Personalized drug therapy for advanced-stage patients by CTCs
3.1. CTC-derived Ex Vivo models for rapid drug testing of advanced-stage patients
The molecular characterization of individual CTC revealed the important information about the genotype and phenotype of tumor cells and demonstrated a remarkable heterogeneity of CTC. Currently, investigations have been made to seek the molecular characterization of CTC, as a manner to increase their diagnostic specificity. The expansion of viable CTC ex vivo contributes to molecular analysis and drugs testing for advanced-stage patients in a shorter time. Recently, Lin and colleagues extracted CTC from blood samples of head and neck cancer (HNC) patients through eSelect, a lab-developed biomimetic cell culture system, and then expanded ex vivo to form organoids that could be tested with anti-cancer therapeutic groups. The drug sensitivity profiles derived from cisplatin treatment of organoids were subsequently found to correlate with clinical treatment response to cisplatin in patients. This is the first study to report the establishment of tumor organoid culturing from CTC of patients with HNC. It is also the first study to evaluate drug sensitivity using CTC-derived organoids and to correlate the results with actual clinical responses in patients with HNC [42].
Ex vivo cultures also present the possibility of pre-clinical testing to determine drug susceptibility. Kapeleris and colleagues used the spiral microfluidic chip and a RosetteSep™ enriching CTCs from blood of non-small cell lung cancer (NSCLC) patients. CTC cultures were carried out using the Clevers media under hypoxic conditions and characterized by exome sequencing. The whole exome sequencing (WES) confirmed the presence of somatic mutations in the CTC cultures with mutational signatures consistent with NSCLC [43]. Rivera-Báez et al. first reported the obtain of CTC cells from locally advanced pancreatic cancer patients and the application of the CTC cell line as a therapeutic response surrogate to detect the changes in cell proliferation, cell cycle and DNA damage accumulation during drug treatment [36]. These suggest that the CTC cell line has the same mutational characteristics as the patient's tumor cells, which can be used for drug sensitivity testing, so as to quickly help patients determine effective treatment options and further promote personalized tumor therapy.
3.2. CTC-derived xenografts for the evaluation of drug susceptibility
In vivo models have a great potential application in basic and preclinical cancer research, such as the discovery of biomarkers, the understanding of drug resistance mechanisms and the development of new therapies. CDX molecular characterization provides a unique tool to enhance our understanding of the main pathways implicated in tumors evolution and dissemination, and to identify interesting prognosis markers and therapeutic targets. The development of a CTC-derived xenograft from a metastatic Triple Negative Breast Cancer (TNBC) patient was firstly described by Tais Pereira-Veiga. This study demonstrates that CTC from TNBC are tumorigenic and highlights CDXs as a unique tool to better understand TNBC biology and develop novel therapeutic approaches [41]. CTC-derived xenografts models generated from some CTC cultures were tested for response to an array of anticancer drugs that included inhibitors of PI3K, CDK4/6, IGFR, ER, mTOR, HSP90, FGFR, PARP, and some first-line chemotherapeutic drugs like paclitaxel, capecitabine, and doxorubicin [44]. These drugs alone or in combination targeted CTC-derived cell lines both with mutated oncogenic drivers like PIK3CA, FGFR2, TP53, ESR1, and BRCA2 or non-mutated targets like HSP90 and IGFR [45]. Some of the drug sensitivity and resistance results were concordant with available clinical histories of the patients, and the combination of treatments targeted two pathways were more effective than single drug treatment in some cell lines and CTC-derived xenografts mouse models tested with specific oncogenic driver mutations.
3.3. Maintain of the mutational traits of the primary tumor for personalized drug screening
Detection and characterization of CTC have prognostic value in various tumor entities, but not all CTCs are likely to extravasate at a distance and grow into new metastatic lesions [46]. A large number of factors can affect the survival and extravasation and metastasis ability of CTC in the blood flow microenvironment [47]. Experimental models have shown that only a few CTCs survive in the bloodstream and reach distal organs to form significant metastases. To understand the underlying mechanisms of the metastatic cascade, functional characterizations of CTC forming the distal metastases are essential. Recently, the breast cancer circulating cell line CTC-ITB-01 constructed by Claudia Koch reflects that the CTC cell line expanded in vitro is highly consistent with the CTC cells in cancer patients [48], which can reflect the mutation deposition in the metastatic cascade of tumor cells in the primary lesion of patients. Vincent Faugeroux reported the first castration-resistant prostate cancer (CRPC) CTC-derived xenografts model and showed the harbored phenotypical and genetic characteristics of CRPC into an aggressive neuroendocrine disease (CRPC-NE). The CTC-derived xenografts model and the CTC-derived xenografts model derived-cell line conserve 16% of primary tumor (PT) and 56% of CTC mutations, which are likely to retain the drug sensitivity mutation and drug resistance mutation mechanism [49]. These results indicate that the CTC models retain the mutational traits of the primary tumor metastasis cascade to a certain extent, especially in genomics, which is of great significance for the personalized drug testing and evaluation of patients.
4. Tumor organoids-on-chips for high-throughput drug screening
Tumor organoids are three-dimensional cellular structures that are generated by culturing tumor cells within microfabricated devices, creating specific 3D microarchitectures. These organoids can better simulate the microstructure, dynamic mechanical properties, and biochemical functions of the tumor organization [50]. They have a wide range of applications in in vitro modeling of biological functions, drug testing, and biological modeling of diseases [51,52,53]. Patient-derived tumor organoids (PDOs) are 3D cellular aggregates obtained from the tumor cells of individual patients. These PDOs display a tissue-like structure and replicate the specific characteristics and heterogeneity of the patient's tumor. They are known for their ability to closely mimic the histological characteristics and functions of patient tumors.
Tumor organoids-on-chip is a novel technology building upon the concept of tumor organoids. The main distinction between organoids and organoids-on-chip is that the latter incorporates airways or blood channels to mimic the native microenvironment of organs. This inclusion of vascular or airway structures allows for a more realistic representation of the organ's microenvironment and facilitates studying drug delivery, perfusion, and interactions with surrounding tissues. While tumor organoids have demonstrated the ability to mimic patient tumors, they do have limitations in terms of their biomimicry, controllability, and repeatability. Tumor organoids-on-chips, on the other hand, offer superior controllability and standardization in modeling. These chips allow for precise control over various factors, such as flow rates, oxygen and nutrient gradients, and mechanical forces, providing a more controlled and reproducible experimental platform. Additionally, the co-culture technology used in tumor organoids-on-chips enables the construction of more intricate models. By incorporating multiple cell types (including tumor cells, stromal cells, immune cells, etc.) in a spatially controlled manner, researchers can mimic the complex cell-cell interactions and microenvironmental crosstalk that occur within tumors.
In summary, tumor organoids and tumor organoids-on-chips are powerful tools in cancer research. While tumor organoids excel in replicating patient-specific tumor characteristics, tumor organoids-on-chips offer enhanced controllability, reproducibility, and the ability to mimic native organ microenvironments. These technologies hold great promise for advancing drug discovery, personalized medicine, and our understanding of tumor biology.
4.1. Construction of tumor organoids and organoids-on-chips
Organoids is a 3D cellular complex with a portion of dimensional construction formed by the differentiation of stem cells cultured in vitro. Cells collection for the organoid construction would be from solid surgical resection or biopsy, nasal brush samples, transurethral resections, or fluid samples such as urine, ascites, or broncho-alveolar lavage fluid, for solid tissue [54,55,56,57,58,59]. Tumor organoids, formed by culturing tumor cells in a 3D structured environment, can replicate the characteristic of parental tumors and have highly consistent with parental tumor in histological and genetic feature. After the generation of the biobank, organoids would be prepared for drug screening, with the therapy of interest [60]. Existing tumor organoid models are summarized in Table 4.
Table 4. Currently available tumor organoid models. |
| Cancer type | Source | Application | Ref. |
|---|---|---|---|
| Gastrointestinal cancers | Metastases | Simulate treatment response | [54] |
| Endometrial cancer | Endometriosis | Drug screening | [65] |
| Colorectal cancer | Primary tumor | Predict Chemoradiation Responses | [97] |
| Cervical cancer | Healthy cervical tissue | Model dynamics and viral oncogenesis | [98] |
| Lung cancer | Primary tumor | Therapeutic screening | [99] |
| Cholangiocarcinoma | Primary tumor | Evaluation of novel treatments | [100] |
| Prostate cancer | Metastases and CTC | Homeostasis, tumorigenesis and drug discovery | [101] |
| Liver cancer | Primary tumor | Disease modeling and drug screening | [102] |
| Breast cancer | Primary tumor | Captures disease heterogeneity | [66] |
| Pancreatic cancer | Primary tumor | Modeling and drug screening | [103] |
The organ-on-chip model, as 3D culture models that are more realistic than organoids, in which researchers build 3D channels and chambers using soft lithography or a 3D printer. Channels and chambers are filled with cell-containing hydrogels or perfusion fluids to mimic the structure and mechanical forces of human tissue. Organ-on-chip features a modular design, choice of micro channels, barrier and ECM, and precise control of physicochemical properties such as interstitial pressure, soluble factor gradients, shear stress, microenvironment stiffness or viscoelasticity and oxygen tension [61]. Some reported organ-on-chips types summarized in Table 5.
Table 5. Some reported organ-on-chip types. |
| Organ | Desired cell type | Ref. |
|---|---|---|
| Liver | hepatocytes, vascular endothelial cells, fibroblasts | [104,105] |
| Lung | alveolar epithelial cells, microvascular endothelial cells | [106] |
| Intestinal | Enterocytes, Adherent epithelium, Mononuclear Cells | [107,108] |
| Lymph node | Bulk B cells or naïve B cells, T cells and monocytes | [109] |
| Gut | Intestinal epithelial cells | [110] |
| Bone | Osteoblasts, Osteocytes | [111] |
| Breast | Mammary epithelial cells, Mammary fibroblasts, Vascular endothelial cells | [112] |
| Glomerulus | Kidney progenitor cells, human primary podocytes and glomerular endothelial cells | [113] |
| Eye | HUVECs, retinal pigment epithelium | [114,115] |
| Brain | dopaminergic neurons, astrocytes, microglia, pericytes | [116] |
The combination of microfluidic technology with 3D tumor organoid models to reproduce tumor tissue and in vivo function has led to the development of an appropriate preclinical tumor organoids-on-chip, paving the way for individualized tumor therapy. Diana Pinho's team successfully obtained a colorectal cancer organoids-on-chip by designing and assembling a special microfluidic device combined with organoid culture technology [62]. The constructed organoids-on-chip significantly improves the formation efficiency and overall size of colorectal cancer organoids, providing an alternative in vitro model for disease modeling and drug screening [62].
4.2. Application of the organoids and organoids-on-chips in drug therapy
The construction and application of organoids and organoids-on-chip are shown in Fig. 3. Organoids are three-dimensional cell complexes that are structurally and functionally similar to the target organ or tissue by inducing the differentiation of stem cells or organ progenitor cells using 3D culture technology in vitro. Organoids have stable phenotypic and genetic characteristics and can be cultured in vitro for a long time. Organoids can simulate the genetic and epigenetic characteristics of target tissues or organs to a large extent, and have broad application prospects in organ development, precision medicine, regenerative medicine, drug screening, gene editing, disease modeling and other fields.
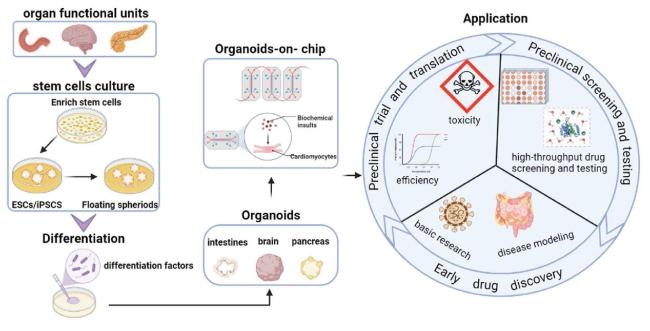
Fig. 3. Construction and application of organoids and organoids-on-chips. |
Organoids-on-chip uses microfluidic technology to control fluid flow, combine cell-cell interaction, matrix properties, biochemical and biomechanical properties, and construct a three-dimensional physiological microsystem of tumor organoids on the chip. Microfluidic chip systems can control the diameter of microtissues and organs to millimeters or even microns, enhance nutrient exchange, and prevent tumor organoids death. In other words, organoids-on-chips not only need to be reconstructed completely according to the tissue or organ in which the tumor is located, but also have the physiological activity and structural and functional characteristics of the original organs and tissues of the human body. It can become a good substitute for predicting the response of the human body to drugs and various external stimuli.
4.3. Patient-derived cancer organoids high-throughput drug screening in different tumors
PDO has recently emerged as a powerful preclinical model, with several studies demonstrating that molecular profiling of tumor organoids matches drug screening results, suggesting that PDO can complement existing approaches to define cancer vulnerability and improve treatment response. Studies have compared ex vivo organoid responses to anti-colorectal and gastroesophageal cancer drugs, as well as PDO-based orthotopic mouse tumor xenograft models with patient responses in clinical trials. The results showed that phenotypic and genotypic analysis of PDO showed high similarity to the original patient tumor [54,63].
Another study on bladder cancer confirmed that patient-derived bladder tumor organoids can recapitulate the broad histopathological and molecular profiles of human non-muscle-invasive and muscle-invasive bladder cancers. Patient-derived bladder tumor organoids typically retain significant tumor heterogeneity and readily undergo clonal evolution in culture. Organoids and orthotopic xenografts can be efficiently interconverted, allowing each model to be used when appropriate for its specific experimental strengths, including for validation of drug responses in vivo [64].
In a separate study on cervical cancer, the authors constructed an expanded biobank spanning healthy and pathological endometrium, providing promising research models and tools for drug screening and discovery. And organoids have been developed from proliferative endometrium, including Lynch syndrome, that faithfully reproduce disease genotypes and are valuable for the search for the molecular mechanisms underlying the proliferative phenotype and its progression to cancer [65].
Similar results were obtained for organoids derived from pancreatic and breast cancers, although the patient cohorts were much smaller [66,67]. Whether in vitro sensitivity to a drug can actually predict a patient's clinical response to the same drug remains to be determined. Recent data suggest that this may actually vary depending on the therapy being tested. Currently, we are waiting for more studies to investigate the predictive potential of organoids. To further characterize tumor-specific sensitivity to drugs and possible adverse effects on healthy tissue, patient-matched normal organoids may also be considered for inclusion in drug screening.
4.4. Organoids-on-chips for personalized drug testing
To evaluate drug efficacy and safety, organoids-on-chips have compelling advantages over other in vitro cell culture models. Compared with 2D cell monolayers in traditional culture models, biomimetic 3D tissue structures with physiological barrier functions more accurately mimic the delivery and penetration of pharmaceutical compounds in vivo. More importantly, these micro-organoids-on-chips models recapitulate the complex interactions between different types of cells in vivo mediated by various soluble and insoluble factors such as cytokines, nutrients, growth factors, hormones, extracellular matrix and cell-to-cell connections, all of which can be controlled within an organoids-on-chips [68].
Organoids-on-chips technology has been used to test small molecule drugs to screen for potential therapeutic and regulatory options. The technology promises to facilitate the development of new therapeutics and has led to the development of multi-organ-on-chip (MOCs) for recapitulating various organs involved in drug-body interactions. The main motivation behind this is to include the gut part for simulating drug absorption and the liver part for simulating drug metabolism [69].
An orthotopic organoids-on-chips model of human non-small cell lung cancer was created that represents the in vivo microenvironment. The investigators seeded H1975, human NSCLC adenocarcinoma cells, at low cell density. At the same time have 100-fold higher primary alveolar or small airway epithelial cells on the upper surface of the ECM coating to integrate cancer cells into the tissue layer during tissue differentiation. The results showed that cancer cells grew faster in the alveolar chip, and respiratory movements inhibited cancer growth and invasion in the lungs, and altered the efficacy of rosicitinib [70]. A more sophisticated version of the device, containing three parallel channels, ECM gel lined with endothelial cells and fibroblasts, supports the formation of a 3D branching microvascular network, and enables the analysis of human lung adenocarcinoma cells against clinically relevant concentrations of the chemotherapeutic drug paclitaxel response and demonstrated tumor and endothelial cell toxicity [71].
The organoids-on-Chips field can only reach its full potential if it translates into commercial drug discovery, and organoids-on-Chips models must pass rigorous validation before they can serve as formal preclinical tests.
5. Discussion
The drug development process is characterized by a high failure rate due to the stringent criteria for success in the preclinical phase. The selection of animal models has been playing a crucial role in evaluating the target validity and the clinical efficacy of the drug, thus affecting the success rate of these phases. Despite the inability of animal models to replicate all the complexities of human disease, it is essential to assess specific aspects of the disease. Existing preclinical tumor models have certain limitations, which affect the translational potential and reliability of the results obtained from these models. For instance, preclinical tumor models such as cell lines or animal models often fail to fully recapitulate the complex tumor microenvironment observed in human patients. The lack of representativeness restricts the predictive value of these models in terms of treatment response or toxicity assessment. Additionally, many tumors exhibit significant genetic heterogeneity, with different subclones harboring distinct mutation spectra. However, most preclinical models tend to represent dominant clones or single gene alterations, which may not capture the full spectrum of tumor diversity in patients [72]. Moreover, the immune system plays a crucial role in tumor development and therapeutic response. Yet, most preclinical tumor models fail to adequately capture the interaction between tumors and the immune system, thereby limiting the ability to study immunotherapies or assess combination therapies [73]. In addition to the aforementioned common limitations, preclinical tumor models also suffer from issues such as inadequate drug penetration, time constraints, and cost limitations [74]. Addressing these limitations is vital to enhancing the translational potential of preclinical tumor models. Patient-derived tumor xenograft models have emerged as indispensable tools for biomedical research and can provide a platform for preclinical drug screening. Currently, commonly used models include CDX, PDX, organoids, and patient-derived CTC models, each with unique functions to support effective experimental studies in different research stages. It is crucial to ensure that the chosen model is fit-for-purpose when conducting researches. In this research, the above-mentioned patient-derived tumor animal models were evaluated, and their unique applications in personalized drug therapy were summarized respectively.
We comprehensively compare the advantages and disadvantages of PDX models, CTC-derived models, and tumor organoids-on-chips. Each model has its own unique advantages and limitations (as Table 6), which may affect their utility in cancer research and drug development. The PDX model is a promising preclinical tool for predicting carcinogenesis, personalized cancer therapy, and developing drugs. However, the high cost, long cycles (lasting at least 3 months), and the large number of animals required for PDX development restrict the widespread and implementation of PDX models. In addition, the humanization of mice remains a critical challenge to overcome, as the mouse matrix will gradually replace the human matrix in the tissue after the construction of models [75]. Another major obstacle is the use of immunocompromised mice to avoid xenograft rejection, which will lead to the progressive loss of patient-derived immune cells over time and significantly affect the therapeutic response. Consequently, PDX models may not be suitable for evaluating currently popular tumor immunotherapies. The establishment of organoids represents a promising avenue for providing personalized treatment strategies for patients. By obtaining samples from tumor tissues and surrounding normal tissues to establish organoids from patients, drug sensitivity tests can be conducted to generate drug dose response curves for patients, providing a valuable reference for clinical treatment [76]. In addition, the association between a patient's mutation pool and their corresponding drug responses can be explored to develop effective targeted therapies. Despite the promising results of Patient-Derived Organoids, there are still deficiencies in simulating the authenticity and integrity of tumor tissue in vivo due to the limited interaction with the tumor microenvironment [77]. Furthermore, the molecular heterogeneity of parental tumors and their corresponding organoids presents a barrier to the use of organoids in predicting the effects of antitumor drugs [78], in addition to the challenges of simulating the in vitro tumor microenvironment. CTC derived CDX model has prominent effect in investigating the tumor heterogeneity. CTC isolated from whole blood of patients can be injected into immunodeficient mice to facilitate effective anticancer drug screening and molecular analysis such as proteomics and transcriptomics [35]. To ensure the clinical relevance of CTC as a tumor model, it is essential that CTC is derived from patients rather than mice [79]. Moreover, patient to patient variability must be taken into consideration to account for differences in tumor biology. Finally, the construction of mouse tumor models by CTC requires a high number of CTC, which is not representative of patients with early-stage tumors [80].
Table 6. Advantages and disadvantages of three patient-derived tumor models. |
| Model | Advantages | Disadvantages | Ref. |
|---|---|---|---|
| PDX models | • Recapitulate tumor heterogeneity | • Time-consuming and expensive | [9,82,117] |
| • Long-term stability | • Human-to-mouse xenograft differences | ||
| • Mimics the tumor microenvironment in vivo | • Ethical concerns | ||
| CTC-derived models | • Non-invasive sampling | • Low abundance | [118,119,120] |
| • Potential for liquid biopsy | • Heterogeneity | ||
| • Disease monitoring | • Lack of tumor microenvironment | ||
| Tumor organoids-on-chips | • Tumor microenvironment mimicry | • Simplified microenvironment | [121,122] |
| • High-throughput testing | • Technical challenges | ||
| • Personalized medicine potential | • Limited clinical validation |
These models can only be used to evaluate the efficacy of drugs derived from specific tissues or organs of the patient. In recent years, researchers have focused on developing and characterizing collections of PDX models from different cancer types, which has led to the gradual emergence of organ chips as a promising alternative. By combining cancer organoid culture with microfluid device, it enables the reconstruction of tumor microenvironment in vitro. This model can connect different organ models, including lung, stomach, brain, lymph nodes, intestine, liver and spleen, thymus, kidney, and other organs, and simulate blood flow through microfluidic tubes, even incorporating CTC into the bloodstream. This innovative approach can provide a better understanding of cancer behavior in the body, thereby improving preclinical evaluation of drug efficacy. The FDA has recognized Organ chips and microphysiological systems as separate non-clinical trial evaluation systems for drugs under the bill, with organ chips and cell models, computer modeling and animal models being equally considered. However, due to the individual differences caused by different genetic background and complexed patients’ syndrome, organ chips are unable to precisely evaluate drug efficacy. Additionally, the development of a standardized construction approach for organ chips is crucial for the effective evaluation of different drugs.
In recent years, there has been a growing interest in developing PDX collections for various cancer research applications [81]. Although patient-derived tumor models have the advantages inquiring tumor heterogeneity and predicting clinical efficacy prediction, they also present some limitations, such as high modeling difficulty, long cycle, low success rate, high modeling and maintenance costs, and incomplete simulations of the original tumor. However, these shortcomings can be addressed with further research. As an example, the high modeling cost, long cycle and low success rate will be gradually improved with the large-scale application. Additionally, more areas that require further investigations include implantation procedures, mouse host strain selection, post engraftment manipulations, and the robust application of translational imaging modalities to assess PDX models towards the elucidation of imaging response biomarkers. Furthermore, nomenclature and harmonization in study design and reporting are essential for the effective dissemination of research findings in this field. Despite the critical progress made in the development of patient-derived tumor models so far, additional research is necessary to advance their applications in cancer research [82].
In the future, there will be a growing demand for the use of patient-derived models in the screening and evaluation of anti-tumor drugs, clinical medication guidance, and personalized treatment of cancer patients. Patient-derived tumor models are expected to assist in the design of clinical trials and integrate into personalized medicine strategies, and these models will eventually play a broader role in drug development.
Conflict of interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Acknowledgement
This study was supported by the National Natural Science Foundation of China (31971239, 11932014) and Sichuan Science and Technology Program (2022NSFSC0765, 2022ZYD0079).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}