诊断学理论与实践 ›› 2022, Vol. 21 ›› Issue (01): 80-85.doi: 10.16150/j.1671-2870.2022.01.015
蔡晓婷a, 易华华a, 林佳媛b, 陈聆a
出版日期:2022-02-25
发布日期:2022-02-25
通讯作者:
陈聆
基金资助:CAI Xiaotinga, YI Huahuaa, LIN Jiayuanb, CHEN Linga
Online:2022-02-25
Published:2022-02-25
Contact:
CHEN Ling
摘要:
目的: 分析1例常染色体显性多囊肾(autosomal dominant polycystic kidndy disease,ADPKD)患者发生肺栓塞(pulmonary thromboembolism, PTE)的临床资料,并总结数据库报道的该病合并静脉血栓形成(venous thromboembolism,VTE)的诊断和治疗。目的: 分析我院收治的1例ADPKD[存在多囊肝(polycystic liver disease, PLD)]合并PTE患者,同时收集PubMed及万方等数据库中报道ADPKD合并VTE患者的临床表现及实验室检测,探讨该病的诊疗。结果: 本例患者因胸痛、气促,查肺通气灌注及下肢深静脉显像发现PTE及下肢深静脉血栓;腹部增强MRI提示下腔静脉肝段狭窄,PLD伴多囊肾;全外显子测序显示PKD1基因杂合变异,PROS1基因杂合变异。共收集数据库报道ADPKD病例15例(13例存在PLD),其中合并下腔静脉血栓者15例,合并肝静脉血栓者2例,合并下肢深静脉血栓者12例,合并PTE 2例。文献中10例患者及本例患者经过低分子肝素桥接华法林抗凝,症状缓解,5例患者需硬化剂治疗、下腔静脉滤器植入及手术治疗。结论: ADPKD不常被认为是VTE发生的原因,但患者存在多囊肾的同时,多数存在PLD,压迫下腔静脉易导致血栓形成,临床医师需注意;本病诊断有赖于影像,治疗以抗凝为主,减轻囊肿压迫为辅。
中图分类号:
蔡晓婷, 易华华, 林佳媛, 陈聆. 常染色体显性多囊肾合并肺栓塞一例并文献复习[J]. 诊断学理论与实践, 2022, 21(01): 80-85.
CAI Xiaoting, YI Huahua, LIN Jiayuan, CHEN Ling. Autosomal dominant polycystic kidney disease complicated with pulmonary embolism: a case report and literature review[J]. Journal of Diagnostics Concepts & Practice, 2022, 21(01): 80-85.
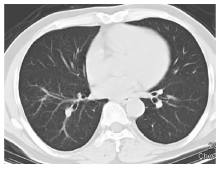
图1
胸部CT平扫显示肺实质未见异常(2019年8月12日)


图2
肺通气显像(2019年9月5日)
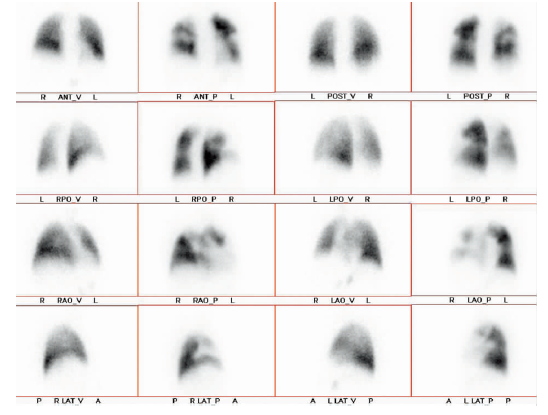
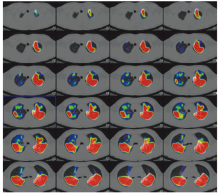
图3
肺灌注显像(2019年9月5日)
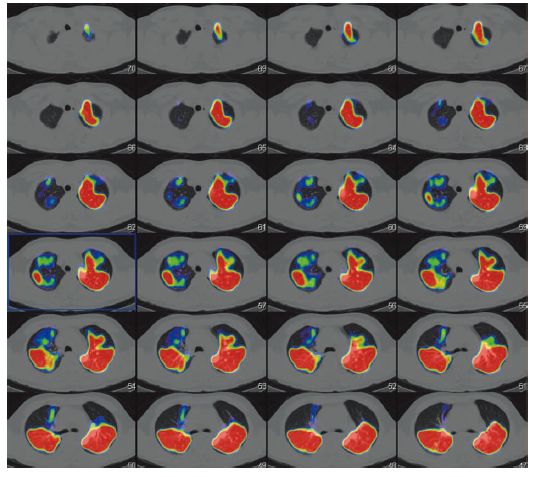
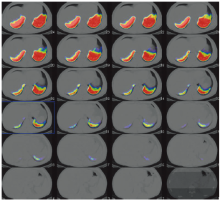
图4
肺通气灌注显像 2019年9月5日 肺灌注显像显示右肺上叶前段及尖段局部、中叶各段、下叶各基底段和左肺上叶前段局部、上舌段、下舌段、下叶前基底段通气显像与灌注显像不匹配,提示PTE高度可能。
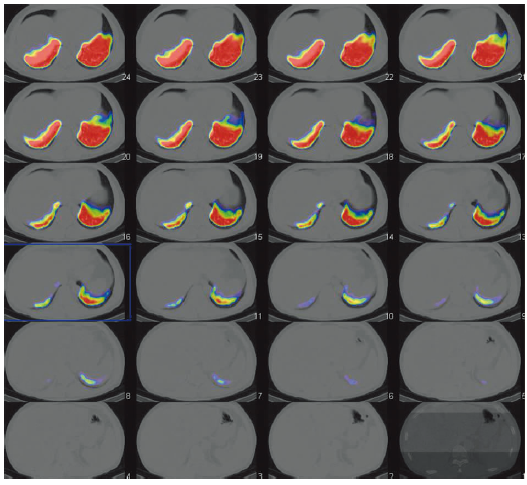
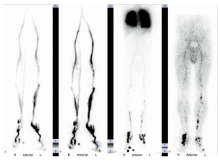
图5
下肢深静脉显像显示双侧下肢深静脉不完全梗阻可能(2019年9月5日)
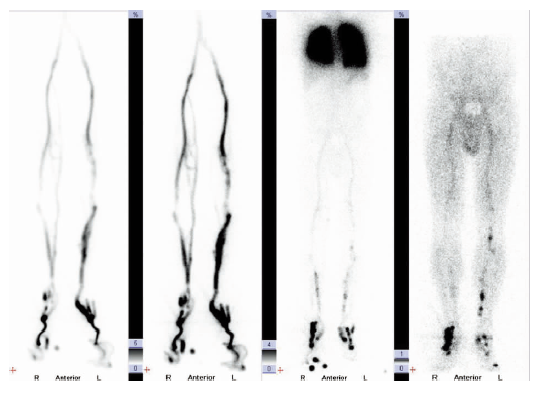
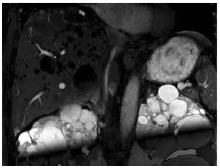
图6
腹部MRI增强显示下腔静脉肝段狭窄、多发肝囊肿伴多囊肾
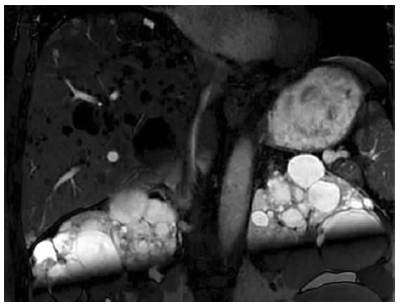

图7
全外显子测序结果 PKD1c.12674A>C(p.Gln4225Pro)杂合变异;PROS1 c.1159C>T(p.Arg387Cys)杂合变异。
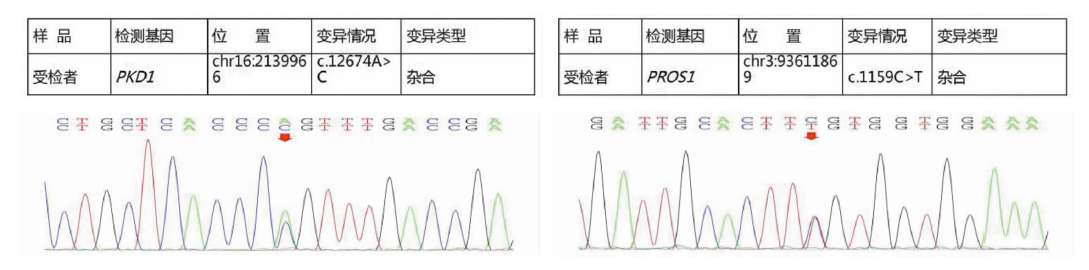
表1
16例多囊肾或多囊肝合并静脉血栓患者临床特征
| 病例(参考文献) | 年龄(岁) | 性别 | ADPKD | PLD | IVCT | DVT | PTE | HVT | 除抗凝外其他治疗 | 预后(至发稿) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1[ | 58 | 男 | + | + | + | + | - | 无 | 症状缓解 | |
| 2[ | 71 | 女 | + | + | + | - | - | 囊肿硬化剂,囊肿壁切除 | 症状缓解 | |
| 3[ | 76 | 男 | + | + | + | + | - | - | 无 | 症状缓解 |
| 4[ | 47 | 女 | + | + | + | + | - | - | 无 | 症状缓解 |
| 5[ | 53 | 女 | + | + | + | + | + | - | 肺动脉取栓 | 症状缓解 |
| 6[ | 53 | 女 | + | + | + | + | - | - | 囊肿切除 | 症状缓解 |
| 7[ | 61 | 女 | + | + | + | + | - | - | 囊肿切除 | 症状缓解 |
| 8[ | 58 | 女 | + | + | + | - | - | - | 囊肿切除 | 症状缓解 |
| 9[ | 73 | 女 | + | + | + | + | - | + | 囊肿切除 | 死于术后感染 |
| 10[ | 68 | 女 | + | + | + | + | - | + | 门脉分流 | 腹水消失 |
| 11[ | 65 | 女 | + | + | + | + | - | - | 囊肿硬化剂,下腔静脉滤器 | 死于肾衰 |
| 12[ | 71 | 女 | + | + | + | + | - | - | 囊肿硬化剂,下腔静脉滤器 | 死亡原因不详 |
| 13[ | 48 | 女 | + | + | + | - | - | - | 囊肿硬化剂,下腔静脉滤器 | 症状缓解 |
| 14[ | 35 | 男 | + | + | + | + | - | - | 下腔静脉滤器 | 症状缓解 |
| 15[ | 59 | 男 | + | + | + | - | - | - | 囊肿硬化剂,下腔静脉滤器 | 症状缓解 |
| 16(本例) | 45 | 男 | + | + | + | + | 无 | 死于脑血管意外 |
| [1] |
Chen Y, Yang K, Marušic A, et al. A Reporting Tool for Practice Guidelines in Health Care: The RIGHT Statement[J]. Ann Intern Med, 2017, 166(2):128-132.
doi: 10.7326/M16-1565 URL |
| [2] |
Paul BM, Vanden Heuvel GB. Kidney: polycystic kidney disease[J]. Wiley Interdiscip Rev Dev Biol, 2014, 3(6):465-87.
doi: 10.1002/wdev.152 URL |
| [3] | O′Sullivan DA, Torres VE, Heit JA, et al. Compression of the inferior vena cava by right renal cysts: an unusual cause of IVC and/or iliofemoral thrombosis with pulmonary embolism in autosomal dominant polycystic kidney disease[J]. Clin Nephrol, 1998, 49(5):332-334. |
| [4] |
Maeda T, Uchida Y, Oyamada K, et al. Thrombosis in inferior vena cava due to enlarged renal cysts in autosomal dominant polycystic kidney disease[J]. Intern Med, 2010, 49(17):1891-1894.
doi: 10.2169/internalmedicine.49.3748 URL |
| [5] |
Iguchi S, Kasai A, Kishimoto H, et al. Thrombosis in inferior vena cava (IVC) due to intra-cystic hemorrhage into a hepatic local cyst with autosomal dominant polycystic kidney disease(ADPKD)[J]. Intern Med, 2004, 43(3):209-212.
doi: 10.2169/internalmedicine.43.209 URL |
| [6] |
Yaqoob M, Saffman C, Finn R, et al. Inferior vena caval compression by hepatic cysts: an unusual complication of adult polycystic kidney disease[J]. Nephron, 1990, 54(1):89-91.
pmid: 2296350 |
| [7] |
Yamasaki K, Haruyama N, Taniguchi M, et al. Subacute pulmonary embolism in a hemodialysis patient, successfully treated with surgical thrombectomy[J]. CEN Case Rep, 2016, 5(1):74-77.
doi: 10.1007/s13730-015-0195-9 URL |
| [8] |
Torres VE, Rastogi S, King BF, et al. Hepatic venous outflow obstruction in autosomal dominant polycystic kidney disease[J]. J Am Soc Nephrol, 1994, 5(5):1186-1192.
doi: 10.1681/ASN.V551186 pmid: 7873728 |
| [9] |
Jalal DI, Chonchol M, Targher G. Disorders of hemostasis associated with chronic kidney disease[J]. Semin Thromb Hemost, 2010, 36(1):34-40.
doi: 10.1055/s-0030-1248722 URL |
| [10] |
Coresh J, Selvin E, Stevens LA, et al. Prevalence of chronic kidney disease in the United States[J]. JAMA, 2007, 298(17):2038-2047.
doi: 10.1001/jama.298.17.2038 pmid: 17986697 |
| [11] |
Sørensen HT, Horvath-Puho E, Pedersen L, et al. Venous thromboembolism and subsequent hospitalisation due to acute arterial cardiovascular events: a 20-year cohort study[J]. Lancet, 2007, 370(9601):1773-1779.
pmid: 18037081 |
| [12] |
Mahmoodi BK, Gansevoort RT, Næss IA, et al. Association of mild to moderate chronic kidney disease with venous thromboembolism: pooled analysis of five prospective general population cohorts[J]. Circulation, 2012, 126(16):1964-1971.
doi: 10.1161/CIRCULATIONAHA.112.113944 URL |
| [13] |
Christiansen CF, Schmidt M, Lamberg AL, et al. Kidney disease and risk of venous thromboembolism: a nationwide population-based case-control study[J]. J Thromb Haemost, 2014, 12(9):1449-1454.
doi: 10.1111/jth.12652 pmid: 25040558 |
| [14] |
ten Kate MK, van der Meer J. Protein S deficiency: a clinical perspective[J]. Haemophilia, 2008, 14(6):1222-1228.
doi: 10.1111/j.1365-2516.2008.01775.x pmid: 18479427 |
| [15] |
Ikejiri M, Tsuji A, Wada H, et al. Analysis three abnormal Protein S genes in a patient with pulmonary embolism[J]. Thromb Res, 2010, 125(6):529-532.
doi: 10.1016/j.thromres.2009.12.025 pmid: 20181378 |
| [16] |
Mateo J, Oliver A, Borrell M, et al. Laboratory evaluation and clinical characteristics of 2,132 consecutive unselected patients with venous thromboembolism--results of the Spanish Multicentric Study on Thrombophilia (EMET-Study)[J]. Thromb Haemost, 1997, 77(3):444-451.
doi: 10.1055/s-0038-1655986 URL |
| [17] |
Konstantinides SV, Barco S, Lankeit M, et al. Management of Pulmonary Embolism: An Update[J]. J Am Coll Cardiol, 2016, 67(8):976-990.
doi: 10.1016/j.jacc.2015.11.061 pmid: 26916489 |
| [18] |
Demir E, Alan C, Kilciler M, et al. Comparison of ethanol and sodium tetradecyl sulfate in the sclerotherapy of renal cyst[J]. J Endourol, 2007, 21(8):903-905.
doi: 10.1089/end.2006.0462 URL |
| [19] |
Okeke AA, Mitchelmore AE, Keeley FX, et al. A comparison of aspiration and sclerotherapy with laparoscopic de-roofing in the management of symptomatic simple renal cysts[J]. BJU Int, 2003, 92(6):610-613.
pmid: 14511045 |
| [20] |
Kohli V, Pande GK, Dev V, et al. Management of hepatic venous outflow obstruction[J]. Lancet, 1993, 342(8873):718-722.
pmid: 8103826 |
| [1] | 陈纯娟, 张曹进. 慢性血栓栓塞性肺动脉高压的诊治现状及治理[J]. 诊断学理论与实践, 2019, 18(1): 28-33. |
| [2] | 杨媛华. 肺栓塞的鉴别诊断体会[J]. 诊断学理论与实践, 2019, 18(1): 6-9. |
| [3] | 郑敏文. 肺栓塞的影像学诊断认识及策略[J]. 诊断学理论与实践, 2019, 18(1): 21-27. |
| [4] | 张姗姗, 杨玲. 肺栓塞误诊为肺炎的原因分析[J]. 诊断学理论与实践, 2017, 16(05): 549-552. |
| [5] | 晁慧娟, 陈长强, 陈聆, 程齐俭. Wells量表和修正Geneva量表及其简化版对肺栓塞临床可能性评估的应用[J]. 诊断学理论与实践, 2017, 16(04): 414-418. |
| [6] | 郁胜强, 贺靓靓,. 多囊肾病发病机制转化治疗策略[J]. 诊断学理论与实践, 2011, 10(03): 202-206. |
| [7] | 陈建, 俞国庆,. 肾病综合征并发肺血栓栓塞的诊断[J]. 诊断学理论与实践, 2007, 6(06): 555-557. |
| [8] | 陈建, 俞国庆, 彭卫华, 王丽萍, 庄永泽, 林沁, 张勇, 李俊霞,. 肾病综合征合并急性肺血栓栓塞、急性肾功能衰竭抢救成功1例报告及文献复习[J]. 诊断学理论与实践, 2007, 6(06): 547-549. |
| [9] | 郁胜强, 梅长林,. 纤毛在多囊肾病发病中的作用[J]. 诊断学理论与实践, 2007, 6(06): 507-509. |
| [10] | 冯莹,. 肺栓塞诊断剖析[J]. 诊断学理论与实践, 2006, 5(05): 458-460. |
| [11] | 吴达明, 张华, 靳勇, 吴志远, 董海鹏, 陈克敏,. 多排CT对肺动脉栓塞和下肢深静脉血栓检出的研究[J]. 诊断学理论与实践, 2006, 5(03): 221-224. |
| [12] | 方怡, 王鸿利,. D-二聚体不同检测方法在深静脉血栓和肺栓塞诊断中的选择及其意义[J]. 诊断学理论与实践, 2005, 4(05): 420-422. |
| [13] | 汤兵,梅长林,张玲,章建全,孙田美,张树忠. 多囊肾病患者肾脏体积与临床表现关系的研究[J]. 诊断学理论与实践, 2003, 2(04): 43-45. |
| [14] | 梅长林,李林. 常染色体显性遗传性多囊肾病诊治进展[J]. 诊断学理论与实践, 2003, 2(04): 18-20. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||