外科理论与实践 ›› 2020, Vol. 25 ›› Issue (03): 234-238.doi: 10.16139/j.1007-9610.2020.03.012
单成祥, 李伟, 刘冰洋, 王强, 饶文胜, 查斯洛, 仇明, 张伟( )
)
收稿日期:2019-01-15
出版日期:2020-05-25
发布日期:2020-05-25
通讯作者:
张伟
E-mail:zhangwei412@aliyun.com
SHAN Chengxiang, LI Wei, LIU Bingyang, WANG Qiang, RAO WenSheng, ZHA Siluo, QIU Ming, ZHANG Wei()
Received:2019-01-15
Online:2020-05-25
Published:2020-05-25
摘要:
目的:优化甲状旁腺切除术(parathyroidectomy, PTX)治疗继发性甲状旁腺功能亢进(secondary hyperparathyroidism, SHPT)的方法。方法:将PTX术中的示踪显影(tracing/imaging)、分离(dissection)、探查(exploration)、切除(resection)4项整合为Tider方法。甲状腺注射纳米炭示踪显影,分离颈部组织,达到所需解剖界限,视、触双诊探查定位甲状旁腺,切除甲状旁腺时尽可能切除周围可疑组织。2018年3月后应用于25例SHPT病人(Tider组);回顾性对比2015年3月至2018年12月未应用Tider方法的34例SHPT病人(对照组),比较两组手术时间、手术成功率及术后第1天PTH水平。结果:Tider组中22例行甲状旁腺全切除术,3例行甲状旁腺全切除+旁腺自体移植术。共切除101枚甲状旁腺,切除甲状旁腺最大径为(1.56±0.63) cm(左上)、(1.66±0.53) cm(左下)、(1.51±0.56) cm(右上)和(1.72±0.76) cm(右下)。两组手术时间60~150 min,Tider组手术时间明显少于对照组[(82.8±9.5) min比(98.5±20.4) min,P=0.001]。除对照组1例出现拔管后窒息外,两组均无出血、喉返神经损伤、严重低钙血症等围术期并发症发生。Tider组手术均获成功,术后第1天PTH为(22.9±10.3) ng/L,均<65 ng/L。对照组有6例手术失败,术后第1天PTH为(112.3±239.6)(7.7~1 216.0) ng/L。对照组手术成功率为82.4%,两组差异无统计学意义(P=0.075)。结论:Tider方法缩短PTX手术时间,规范手术操作流程,保证手术成功率。
中图分类号:
单成祥, 李伟, 刘冰洋, 王强, 饶文胜, 查斯洛, 仇明, 张伟. Tider方法在手术治疗继发性甲状旁腺功能亢进中的应用[J]. 外科理论与实践, 2020, 25(03): 234-238.
SHAN Chengxiang, LI Wei, LIU Bingyang, WANG Qiang, RAO WenSheng, ZHA Siluo, QIU Ming, ZHANG Wei. Application of Tider process in parathyroidectomy for treatment of secondary hyperparathyroidism[J]. Journal of Surgery Concepts & Practice, 2020, 25(03): 234-238.
表1
术前基线资料
| 组别 | 性别(男/女) | 年龄(岁) | 透析时间 (年) | PTH(ng/L) | 血钙(mmol/L) | 血磷(mmol/L) |
|---|---|---|---|---|---|---|
| Tider组(n=25) | 12/13 | 50.9±10.9 | 7.4±2.3 | 1 834.1±914.8 | 2.5±0.2 | 2.6±0.7 |
| 对照组(n=34) | 15/19 | 48.7±12.6 | 7.2±3.8 | 1 772.0±954.4 | 2.5±0.2 | 2.5±0.2 |
| t值 | 0.707 | 0.215 | 0.251 | -0.369 | 0.429 | |
| χ2值 | 0.087 | |||||
| P值 | 0.767 | 0.483 | 0.830 | 0.803 | 0.714 | 0.669 |
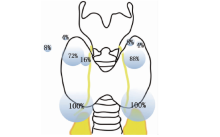
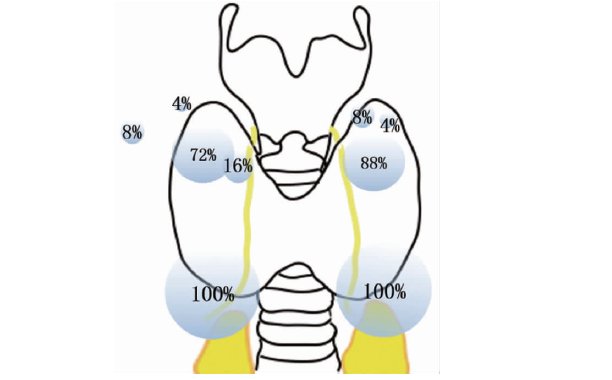
图1
甲状旁腺相对位置示意图
| [1] |
Masakane I, Nakai S, Ogata S, et al. An overview of re-gular dialysis treatment in Japan (as of 31 December 2013)[J]. Ther Apher Dial, 2015, 19(6):540-574.
doi: 10.1111/1744-9987.12378 URL |
| [2] |
Seehofer D, Rayes N, Klupp J, et al. Predictive value of intact parathyroid hormone measurement during surgery for renal hyperparathyroidism[J]. Langenbecks Arch Surg, 2005, 390(3):222-229.
doi: 10.1007/s00423-005-0541-z URL |
| [3] |
Schlosser K, Bartsch DK, Diener MK, et al. Total parathyroidectomy with routine thymectomy and autotransplantation versus total parathyroidectomy alone for secondary hyperparathyroidism: results of a nonconfirmatory multicenter prospective randomized controlled pilot trial[J]. Ann Surg, 2016, 264(5):745-753.
pmid: 27741007 |
| [4] |
Burton JO, Goldsmith DJ, Ruddock N, et al. Renal association commentary on the KDIGO (2017) clinical practice guideline update for the diagnosis, evaluation, prevention, and treatment of CKD-MBD[J]. BMC Nephrol, 2018, 19(1):240.
doi: 10.1186/s12882-018-1037-8 pmid: 30236082 |
| [5] |
Komaba H, Taniguchi M, Wada A, et al. Parathyroidectomy and survival among Japanese hemodialysis patients with secondary hyperparathyroidism[J]. Kidney Int, 2015, 88(2):350-359.
doi: 10.1038/ki.2015.72 URL |
| [6] |
Chen JB, Chou FF, Yang CH, et al. Association between clinical variables and mortality after parathyroidectomy in maintenance hemodialysis patients[J]. Am J Surg, 2017, 213(1):140-145.
doi: 10.1016/j.amjsurg.2016.03.012 URL |
| [7] |
Wang B, Du ZP, Qiu NC, et al. Application of carbon nanoparticles accelerates the rapid recovery of parathyroid function during thyroid carcinoma surgery with central lymph node dissection: A retrospective cohort study[J]. Int J Surg, 2016, 36 (Pt A):164-169.
doi: S1743-9191(16)30996-7 pmid: 27989915 |
| [8] | Boyd JD. Development of the thyroid and parathyroid glands and the thymus[J]. Ann R Coll Surg Engl, 1950, 7(6):455-471. |
| [9] |
Shan CX, Qiu NC, Zha SL, et al. A novel surgical strategy for secondary hyperparathyroidism: Purge parathyroidectomy[J]. Int J Surg, 2017, 43:112-118.
doi: 10.1016/j.ijsu.2017.05.062 URL |
| [10] | Oertli D, Udelsman R. Surgery of the thyroid and parathyroid glands[M]. Berlin; New York: Springer, 2007:13-21. |
| [11] |
Okada M, Tominaga Y, Yamamoto T, et al. Location frequency of missed parathyroid glands after parathyroidectomy in patients with persistent or recurrent secondary hyperparathyroidism[J]. World J Surg, 2016, 40(3):595-599.
doi: 10.1007/s00268-015-3312-1 URL |
| [1] | 占志朋, 谢席胜, 张凌. 维持性血液透析合并难治性继发性甲状旁腺功能亢进患者甲状旁腺激素水平与骨密度的关系[J]. 内科理论与实践, 2021, 16(01): 45-48. |
| [2] | 李伟, 刘冰洋, 单成祥, 饶文胜, 张伟, 仇明. 甲状旁腺肃清术对继发性甲状旁腺功能亢进的疗效评价[J]. 外科理论与实践, 2019, 24(04): 325-329. |
| [3] | 王红鹰, 黄骏文, 邹强, 陈靖, 张敏敏, 张炜晨, 劳正胤. 甲状旁腺全切除加前臂自体移植术治疗肾性继发性甲状旁腺功能亢进的长期疗效[J]. 外科理论与实践, 2018, 23(06): 523-527. |
| [4] | 王琳, 陈东, 朱峰, 辛明徽, 刘畅, 彭程, 刘强强,. 甲状旁腺次全切除术和西那卡塞口服对难治性甲状旁腺功能亢进患者骨代谢的影响[J]. 内科理论与实践, 2018, 13(06): 364-367. |
| [5] | 田滨瑶, 徐天华, 姚丽,. 继发性甲状旁腺功能亢进的治疗与进展[J]. 内科理论与实践, 2018, 13(04): 250-254. |
| [6] | 陈靖,. 慢性肾脏病矿物质和骨异常治疗进展:合理应用维生素D受体激动剂[J]. 内科理论与实践, 2018, 13(04): 207-211. |
| [7] | 李富新, 姜若愚, 李东洋, 陈作宇, 魏铭泽, 张柏, 何向辉. 原发性甲状旁腺功能亢进症临床分析(附138例报告)[J]. 外科理论与实践, 2018, 23(02): 125-129. |
| [8] | 仝海磊, 王培松, 孟伟. 热消融治疗继发性甲状旁腺功能亢进[J]. 外科理论与实践, 2018, 23(02): 166-168. |
| [9] | 陈海珍, 陈曦. 肾性继发性甲状旁腺功能亢进症的多学科协作治疗[J]. 外科理论与实践, 2018, 23(02): 103-107. |
| [10] | 郭伯敏, 樊友本,. 甲状旁腺瘤的内镜手术治疗进展[J]. 外科理论与实践, 2009, 14(01): 111-114. |
| [11] | 王琴, 倪兆慧, 牟姗, 周文彦, 俞赞喆, 朱彩霞, 李萍,. 慢性肾脏病透析前患者的甲状旁腺功能异常及其意义[J]. 诊断学理论与实践, 2006, 5(06): 503-506. |
| [12] | 王红鹰, 邹强, 周坚, 劳正胤, 薛骏, 李铭新, 李海明, 顾勇, 张延龄,. 慢性肾功能衰竭继发甲状旁腺功能亢进的外科治疗[J]. 外科理论与实践, 2005, 10(06): 522-524. |
| [13] | 陈曦,何永刚,杨卫平,李宏为,Yves Chapuis,Philippe Bonnichon. 局麻下小切口甲状旁腺切除术:甲状旁腺手术的另一个选择[J]. 外科理论与实践, 2003, 8(04): 311-313. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||