外科理论与实践 ›› 2022, Vol. 27 ›› Issue (03): 239-243.doi: 10.16139/j.1007-9610.2022.03.011
满高亚1, 党同科1, 吴清松1, 冯飞灵2( )
)
收稿日期:2021-10-19
出版日期:2022-06-25
发布日期:2022-08-03
通讯作者:
冯飞灵
E-mail:ffeiling@163.com.
MAN Gaoya1, DANG Tongke1, WU Qingsong1, FENG Feiling2()
Received:2021-10-19
Online:2022-06-25
Published:2022-08-03
Contact:
FENG Feiling
E-mail:ffeiling@163.com.
摘要:
目的:探讨Rouviere沟引导胆囊后隧道解剖用于困难腹腔镜胆囊切除术。方法:回顾分析2019年1月至2020年10月,滕州市中心人民医院收治的腹腔镜胆囊切除术病人1 081例,依据Gupta的术前评分系统,将评分≥6分的困难胆囊病人125例,分为Rouviere沟引导胆囊切除组(研究组)65例和传统腹腔镜胆囊切除组(对照组)60例。比较两组病人的临床资料、手术和术后并发症发生情况。结果:研究组与对照组的手术时间(61±23) min比(88±24) min(P<0.05),术中出血量(46±16) mL比(62±23) mL(P<0.05),住院时间(3.5±1.5) d比(5.8±2.2) d(P<0.05),人均住院费(12 236±316)元比(14 199±552)元(P<0.05),术后12 h和24 h疼痛视觉模拟评分(2.7±1.1)分和(3.0±1.1)分比(5.9±1.0)分和(6.4±1.5)分(P<0.05),差异均有统计学意义。中转开腹研究组1例,对照组6例。研究组无胆漏,对照组胆漏4例,差异有统计学意义(P<0.05)。研究组术后72 h肝功能较术前改善程度明显优于对照组(P<0.05)。研究组无胆管损伤,对照组胆管损伤1例(P>0.05)。结论:Rouviere沟引导胆囊后隧道解剖行困难胆囊切除术可成为安全腹腔镜胆囊切除术。
中图分类号:
满高亚, 党同科, 吴清松, 冯飞灵. Rouviere沟引导胆囊后隧道解剖用于困难腹腔镜胆囊切除术[J]. 外科理论与实践, 2022, 27(03): 239-243.
MAN Gaoya, DANG Tongke, WU Qingsong, FENG Feiling. Rouviere′s sulcus guided retro-gallbladder tunnel dissection in difficult laparoscopic cholecystectomy[J]. Journal of Surgery Concepts & Practice, 2022, 27(03): 239-243.
表1
术前评分参考指标
| 项目 | 分值 |
|---|---|
| 年龄(岁) ≤50 >50 | 0 1 |
| 性别 男 女 | 1 0 |
| 既往急性胆囊炎病史 有 无 查体触及肿大胆囊 有 无 影像学检查 胆囊壁厚度(mm) <4 ≥4 胆囊颈管结石嵌顿 无 有 胆囊周围粘连 无 有 | 4 0 1 0 0 2 0 2 0 1 |
表2
两组一般资料($\bar{x}\pm s$/n)
| 项目 | 研究组 (n) | 对照组 (n) | t/χ2 | P值 |
|---|---|---|---|---|
| 年龄(岁) | 49.5±6.1 | 49.8±5.9 | t=0.279 | >0.05 |
| 性别 男 女 | 39 26 | 37 23 | χ2=0.036 | 0.849 |
| 既往急性胆囊炎发作史 查体触及肿大胆囊 影像学检查 胆囊壁厚≥4 mm 胆囊颈管结石嵌顿 胆囊周围粘连渗出 难度评分分值(分) | 6 5 40 12 7 10.5±1.3 | 5 4 38 11 6 10.7±1.2 | χ2=0.031 χ2=0.049 χ2=0.043 χ2=0.000 χ2=0.020 t=0.378 | 0.863 0.825 0.836 0.985 0.888 >0.05 |
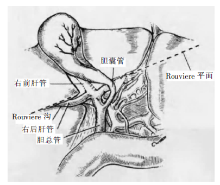
图1
Rouviere沟示意图[9]
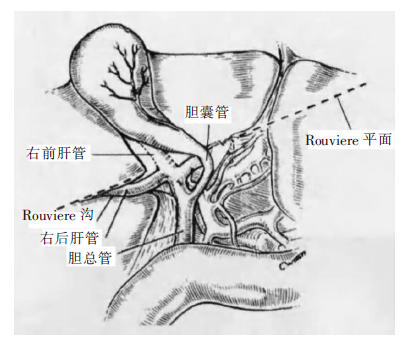
表3
两组手术及术后资料($\bar{x}\pm s$/n)
| 项目 | 研究组 | 对照组 | t/χ2 | P值 |
|---|---|---|---|---|
| 手术时间(min) | 61±23 | 88±24 | t=6.422 | <0.05 |
| 术中出血量(mL) | 46±16 | 62±23 | t=4.543 | <0.05 |
| 胆管损伤 胆漏 中转开腹 住院时间(d) 人均住院费(元) | 0 0 1 3.5±1.5 12 236±316 | 1 4 6 5.8±2.2 14 199±552 | χ2=1.091 χ2=4.477 χ2=4.225 t=6.875 t=24.634 | 0.296 0.034 0.040 <0.05 <0.05 |
表4
两组术前及术后72 h肝功能比较($\bar{x}\pm s$)
| 项目 | 时间 | 研究组 | 对照组 | t值 | P值 |
|---|---|---|---|---|---|
| 天冬氨酸转 氨酶(U/L) | 术前 | 90.4±5.5 | 89.9±5.8 | ||
| 术后72 h | 23.1±5.1 | 52.3±6.1 | 32.822 | <0.05 | |
| 丙氨酸转氨 酶(U/L) | 术前 | 79.3±3.8 | 79.1±4.1 | ||
| 术后72 h | 21.8±3.6 | 47.2±7.5 | 36.110 | <0.05 | |
| 总胆红素 (mol/L) | 术前 | 16.8±2.4 | 16.7±2.5 | ||
| 术后72 h | 15.1±2.1 | 15.0±2.2 | 0 | >0.05 | |
| 碱性磷酸酶 (U/L) | 术前 | 113.3±5.7 | 112.9±5.9 | ||
| 术后72 h | 68.1±3.0 | 70.2±4.1 | 1.538 | >0.05 |
表5
两组术后VAS比较($\bar{x}\pm s$,分)
| 术后时间 | 研究组 | 对照组 | t值 | P值 |
|---|---|---|---|---|
| 术后12 h | 2.7±1.1 | 5.9±1.0 | 16.971 | <0.05 |
| 术后24 h 术后48 h | 3.0±1.1 2.9±1.5 | 6.4±1.5 3.0±1.6 | 14.582 0.361 | <0.05 >0.05 |
| [1] | Onoe S, Maeda A, Takayama Y, et al. A preoperative predictive scoring system to predict the ability to achieve view of safety during laparoscopic cholecystectomy for acute cholecystitis[J]. HPB(Oxford), 2017, 19(5):406-410. |
| [2] |
Bogacki P, Krzak J, Gotfryd-Bugajska K, et al. Evaluation of the usefulness of the SAGES Safe Cholecystectomy Program from the viewpoint of the European surgeon[J]. Videosurgery Miniinv, 2020, 15(1):80-86.
doi: 10.5114/wiitm.2019.83297 pmid: 32117489 |
| [3] | Durowicz S, Kozicki I, Ciesielski A, et al. Excision of a part of the bile duct as an iatrogenic injury typical for laparoscopic cholecystectomy-characteristics,treatment and longterm results,based on own material[J]. Videosurgery Miniinv, 2020, 15(1):70-79. |
| [4] |
Schendel J, Ball C, Dixon E, et al. Prevalence of anato-mic landmarks for orientation during elective laparoscopic cholecystectomies[J]. Surg Endosc, 2020, 34(8):3508-3512.
doi: 10.1007/s00464-019-07131-z URL |
| [5] |
Wakabayashi G, Iwashita Y, Hibi T, et al. Tokyo guidelines 2018: surgical management of acute cholecystitis: safe steps in laparoscopic cholecystectomy for acute cholecystitis (with videos)[J]. J Hepatobiliary Pancreat Sci, 2018, 25(1):73-86.
doi: 10.1002/jhbp.517 URL |
| [6] | Kapoor VK. Mechanisms of causation of bile duct injury[M]// Kapoor VK. Post-cholecystectomy Bile Duct Injury. Singapore: Springer, 2020:21-35. |
| [7] |
Gupta N, Ranjan G, Atora MP, et al. Validation of a scoring system to predict difficult laparoscopic cholecystectomy[J]. Int J Surg, 2013, 11(9):1002-1006.
doi: 10.1016/j.ijsu.2013.05.037 URL |
| [8] |
Di Buono G, Romano G, Galia M, et al. Difficult laparoscopic cholecystectomy and preoperative predictive factors[J]. Sci Rep, 2021, 11(1):2559.
doi: 10.1038/s41598-021-81938-6 URL |
| [9] | Hugh TB, Kelly MD, Mekisic A. Rouviere′s sulcus: a useful landmark in laparoscopic cholecystectomy[J]. Br J Surg, 1997, 84(9):1253-1254. |
| [10] |
Grass K, Oeckl K, Kersting S. The critical view of safety to avoid biliary complications in laparoscopic cholecystectomy[J]. Zentralbl Chir, 2020, 145(4):336-339.
doi: 10.1055/a-1079-6060 URL |
| [11] | Hawker GA, Mian S, Kendzerska T, et al. Measures of adult pain:visual analog scale for pain(VAS pain), nume-ric rating scale for pain(NRS pain), mcgill pain questionnaire(MPQ), short form mcgill pain questionnaire(sf-MPQ), chronic pain grade scale(CPGS), short form-36 bodily pain scale[J]. Arthit Care Res, 2011, 63(11):240-252. |
| [12] |
Pisano M, Allievi N, Gurusamy K, et al. 2020 World Society of Emergency Surgery updated guidelines for the diagnosis and treatment of acute calculus cholecystitis[J]. World J Emerg Surg, 2020, 15(1):61.
doi: 10.1186/s13017-020-00336-x URL |
| [13] |
Gupta V, Jain G. Safe laparoscopic cholecystectomy: adoption of universal culture of safety in cholecystectomy[J]. World J Gastrointest Surg, 2019, 11(2):62-84.
doi: 10.4240/wjgs.v11.i2.62 URL |
| [14] | Stanisic V, Milicevic M, Kocev N, et al. A prospective cohort study for prediction of difficult laparoscopic cholecystectomy[J]. Ann Med Surg, 2020, 12(60):728-733. |
| [15] | Bhandari TR, Khan SA, Jha JL. Prediction of difficult laparoscopic cholecystectomy: an observational study[J]. Ann Med Surg (Lond), 2021, 12(72):103060. |
| [16] |
Schreuder AM, Busch OR, Besselink MG, et al. Long-term impact of iatrogenic bile duct injury[J]. Dig Surg, 2020, 37(1):10-21.
doi: 10.1159/000496432 URL |
| [17] | Christou N, Roux-David A, Naumann DN, et al. Bile duct injury during cholecystectomy: necessity to learn how to do and interpret intraoperative cholangiography[J]. Front Med (Lausanne), 2021, 2(8):637987. |
| [18] | Brunt LM, Deziel DJ, Telem DA, et al. Safe cholecystectomy multi-society practice guideline and state-of-the-art consensus conference on prevention of bile duct injury during cholecystectomy[J]. Ann Surg, 2020, 34(8):2827-2855. |
| [19] |
Cheruiyot I, Nyaanga F, Kipkorir V, et al. The prevalence of the Rouviere’s sulcus: a meta-analysis with implications for laparoscopic cholecystectomy[J]. Clin Anat, 2021, 34(4):556-564.
doi: 10.1002/ca.23605 URL |
| [20] |
Jha AK, Dewan R, Bhaduria K. Importance of Rouviere’s sulcus in laparoscopic cholecystectomy[J]. Ann Afr Med, 2020, 19(4):274-277.
doi: 10.4103/aam.aam_4_20 URL |
| [21] |
Péré G, Benvegnu V, Mercé C, et al. The sulcus of the caudate process (Rouviere’s sulcus): anatomy and clinical applications—a review of current literature[J]. Surg Radiol Anat, 2020, 42(12):1441-1446.
doi: 10.1007/s00276-020-02529-0 URL |
| [22] | Shinde J, Pandit S. Innovative approach to a frozon calot,s triangle during laparoscopic cholecystectomy[J]. Indian J Surgery, 2015, 77(6):1-4. |
| [23] | Way LW, Stewart L, Cantert, et al. Causes and prevention of laparoscopic bile duct injuries analysis of 252 cases from a human factors and cognitive psychology perspective[J]. Ann surg, 2003, 237(4):460-469. |
| [24] |
Cengiz Y, Lund M, Janes A, et al. Fundus first as the standard technique for laparoscopic cholecystectomy[J]. Sci Rep, 2019, 9:18736.
doi: 10.1038/s41598-019-55401-6 pmid: 31822771 |
| [25] |
Ale AF, Isichei MW, Shilong DJ, et al. Fundus first laparoscopic cholecystectomy in patients with gall stone disease and the Fitz-Hugh-Curtis syndrome[J]. Inter J Res Med Sci, 2020, 8(6):2062-2066.
doi: 10.18203/2320-6012.ijrms20202244 URL |
| [26] |
Asai K, Atanabe M, Usachi S, et al. Risk factors for conversion of laparoscopic cholecystectomy to open surgery associated with the severity characteristics according to the Tokyo guidelines[J]. Surg Today, 2014, 44(12):2300-2304.
doi: 10.1007/s00595-014-0838-z URL |
| [27] | Sormaz IC, Soytaş Y, Gök AFK, et al. Fundus-first technique and partial cholecystectomy for difficult laparoscopic cholecystectomies[J]. Ulus Travma Acil Cerrahi Derg, 2018, 24(1):66-70. |
| [28] |
Mahmud S, Masaud M, Canna K, et al. Fundus-first laparoscopic cholecystectomy[J]. Surg Endosc, 2002, 16(4):581-584.
pmid: 11972192 |
| [29] |
Mannino M, Toro A, Teodoro M, et al. Open conversion for laparoscopically difficult cholecystectomy is still a valid solution with unsolved aspects[J]. World J Emerg Surg, 2019; 14(1):10-13.
doi: 10.1186/s13017-019-0224-7 URL |
| [30] | Sewefy AM, Hassanen AM, Atyia AM, et al. Retroinfundibular laparoscopic cholecystectomy versus standard laparoscopic cholecystectomy in difficult cases[J]. Int J Surg, 2017, 7(43):75-80. |
| [1] | 胡刚峰, 黄侠. LC联合ERCP一期治疗胆囊结石合并肝外胆管结石与分期ERCP+LC手术疗效比较[J]. 外科理论与实践, 2021, 26(05): 437-440. |
| [2] | 姚伟, 孔雷, 吴庆华, 陆一凡, 叶靳华, 赵良超, 徐敬慈, 李能平. 早期腹部CT检查在制定急性胆源性胰腺炎诊疗方案中的作用[J]. 外科理论与实践, 2019, 24(03): 236-241. |
| [3] | 罗颖, 钱洁敏, 陈晓薇, 马海燕, 许萍, 刘琳娜, 倪强. 气腹及病人体位对腹腔镜胆囊切除术血流动力学的影响[J]. 外科理论与实践, 2019, 24(01): 70-74. |
| [4] | 吴庆华, 包皙婷, 孔雷, 刘玉祥, 陈勇, 王赭, 项明,. 常规器械经脐腹腔镜胆囊切除术学习曲线分析[J]. 外科理论与实践, 2016, 21(02): 161-165. |
| [5] | 许淑华, 王东平,. 腹腔镜胆囊切除中对肝外胆管变异的认识及处置[J]. 外科理论与实践, 2015, 20(06): 522-524. |
| [6] | 毛志海, 蒋渝, 郑民华,. 腹腔镜下胆管横断伤一期修复:附2例报告[J]. 外科理论与实践, 2011, 16(06): 538-540. |
| [7] | 罗丁,陈训如,李胜宏,毛静熙,周正东,余少明. 复杂类型腹腔镜胆囊切除术中胆道损伤的预防与诊断[J]. 外科理论与实践, 2003, 8(02): 121-123. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||