诊断学理论与实践 ›› 2020, Vol. 19 ›› Issue (05): 487-493.doi: 10.16150/j.1671-2870.2020.05.008
李宙童1,2, 张炜1, 王继光1( )
)
收稿日期:2019-08-22
出版日期:2020-10-25
发布日期:2022-07-14
通讯作者:
王继光
E-mail:jiguangwang@aim.com
基金资助:
LI Zhoutong1,2, ZHANG Wei1, WANG Jiguang1()
Received:2019-08-22
Online:2020-10-25
Published:2022-07-14
Contact:
WANG Jiguang
E-mail:jiguangwang@aim.com
摘要:
目的: 探究家庭血压测量和24 h动态血压(以下称动态血压)监测诊断白大衣高血压及隐匿性高血压的准确性。方法: 研究对象为全国多中心动态血压及家庭血压登记研究中上海地区的受试者,均接受动态血压监测,并进行了诊室血压测量和7 d家庭血压测量。本组总计纳入1 067例患者,平均年龄为57.5岁,男性占39.9%。依据相关高血压指南,白大衣高血压定义为诊室测平均收缩压≥140 mmHg和(或)平均收缩压≥90 mmHg,而动态血压监测正常(平均收缩压<130 mmHg且平均舒张压<80 mmHg)或家庭血压测量正常(平均收缩压<135 mmHg且平均舒张压<85 mmHg);隐匿性高血压为诊室测量血压正常而动态血压升高或家庭血压升高。结果: 在1 067例患者中,接受降压药物治疗的高血压患者为867例,未治疗患者200例。在未治疗患者中,动态血压监测和家庭血压测量诊断白大衣高血压的患病率分别为10.0%和17.0%(P=0.04),动态血压监测和家庭血压测量诊断隐匿性高血压的患病率分别为26.5%和14.5%(P=0.003)。以动态血压监测为标准,无论未治疗患者还是治疗患者,家庭血压测量诊断白大衣及隐匿性高血压的灵敏度都较低(43%~86%),特异度较高(91%~99%),阳性预测值较低(46%~91%),阴性预测值较高(84%~100%)。动态血压监测与家庭血压测量间的诊断一致性为81%~90%,Kappa值为0.43到0.78。结论: 家庭血压测量诊断白大衣及隐匿性高血压的灵敏度较低,但特异度较高。因此,尽管家庭血压测量不能替代动态血压监测,但可作为其有益的补充。
中图分类号:
李宙童, 张炜, 王继光. 家庭血压测量诊断白大衣高血压及隐匿性高血压的准确性研究[J]. 诊断学理论与实践, 2020, 19(05): 487-493.
LI Zhoutong, ZHANG Wei, WANG Jiguang. Accuracy of home versus ambulatory blood pressure monitoring in the diagnosis of white-coat and masked hypertension[J]. Journal of Diagnostics Concepts & Practice, 2020, 19(05): 487-493.
表1
治疗组和未治疗组患者的临床基本特征
| 临床特征 | 治疗组 (n=867) | 未治疗组 (n=200) | P值 |
|---|---|---|---|
| 男性[n (%)] | 335(38.6) | 94(47.0) | 0.030 0 |
| 年龄 (岁) | 59.0±10.2 | 50.8±13.4 | <0.000 1 |
| 体质量指数 (kg/m2) | 24.7±3.3 | 24.1±3.2 | 0.010 0 |
| 吸烟[n (%)] | 105(12.1) | 27(13.5) | 0.630 0 |
| 饮酒[n (%)] | 83(9.6) | 25(12.5) | 0.240 0 |
| 糖尿病[n (%)] | 107(12.3) | 8(4.0) | 0.000 3 |
| 高血压病程(年) | 11.3(0~62.6) | 3.3(0.02~50.5) | <0.000 1 |
| 服用降压药种类 | 2.1±1.1 | - | - |
| 心血管疾病史[n (%)] | 129(14.9) | 8(4.0) | <0.000 1 |
| 诊室血压 (mmHg) | |||
| 收缩压 | 136.7±16.7 | 136.8±14.3 | 0.970 0 |
| 舒张压 | 78.2±10.7 | 81.5±10.7 | <0.000 1 |
| 动态血压 (mmHg) | |||
| 读数 | 58.9±5.0 | 61.0±3.8 | <0.000 1 |
| 收缩压 (mmHg) | 127.0±14.2 | 128.3±10.4 | 0.130 0 |
| 舒张压 (mmHg) | 77.4±9.8 | 80.9±7.8 | <0.000 1 |
| 家庭血压 (mmHg) | |||
| 读数 | 67.9±5.5 | 66.4±8.6 | 0.020 0 |
| 收缩压 (mmHg) | 132.6±14.4 | 130.8±10.8 | 0.040 0 |
| 舒张压 (mmHg) | 77.8±9.5 | 80.6±8.6 | 0.020 0 |
表2
治疗组和未治疗组分别以动态血压监测和家庭血压测量诊断的白大衣高血压及隐匿性、持续性高血压的患病率[n(%)]
| 家庭血压测量诊断 | 动态血压监测诊断的各高血压亚型 | ||||||
|---|---|---|---|---|---|---|---|
| 治疗组 (n=867) | 未治疗组 (n=200) | ||||||
| 是 | 否 | 总计 | 是 | 否 | 总计 | ||
| 白大衣高血压 | |||||||
| 是 | 57 (6.6%) | 46 (5.3%) | 103 (11.9%) | 17(8.5%) | 17(8.5%) | 34 (17.0%) | |
| 否 | 52 (6.0%) | 712 (82.1%) | 764 (88.1%) | 3 (1.5%) | 163 (81.5%) | 166 (83.0%) | |
| 总计 | 109 (12.6%) | 758 (87.4%) | 867 (100%) | 20 (10.0%) | 180 (90.0%) | 200 (100%) | |
| 隐匿性高血压 | |||||||
| 是 | 97 (11.2%) | 45 (5.2%) | 142 (16.4%) | 22 (11.0%) | 7 (3.5%) | 29 (14.5%) | |
| 否 | 95 (11.0%) | 630 (72.7%) | 725 (83.6%) | 31 (15.5%) | 140 (70.0%) | 171 (85.5%) | |
| 总计 | 192 (22.1%) | 675 (77.9%) | 867 (100%) | 53 (26.5%) | 147 (73.5%) | 200 (100%) | |
| 持续性高血压 | |||||||
| 是 | 205 (23.6%) | 52 (6.0%) | 257 (29.6%) | 58 (29.0%) | 3 (1.5%) | 61 (30.5%) | |
| 否 | 46 (5.3%) | 564 (65.1%) | 610 (70.4%) | 17 (8.5%) | 122 (61.0%) | 139 (69.5%) | |
| 总计 | 251 (29.0%) | 616 (71.0%) | 867 (100%) | 75 (37.5%) | 125 (62.5%) | 200 (100%) | |
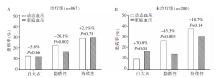
图1
治疗组(A)和未治疗组(B)中动态血压监测和家庭血压测量诊断白大衣高血压及隐匿性、持续性高血压的患病率
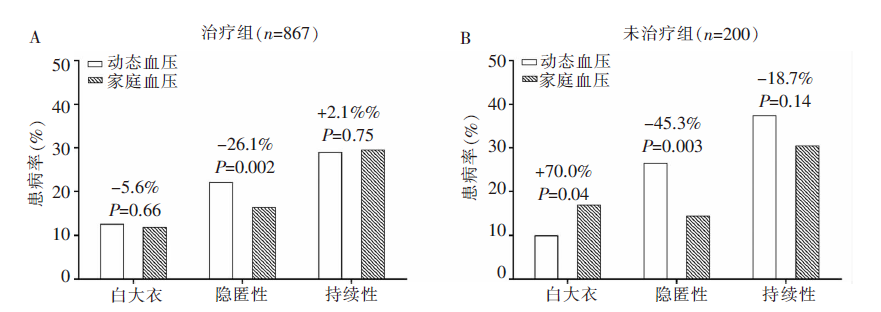
表3
治疗组和未治疗组中家庭血压测量诊断白大衣高血压及隐匿性高血压的效能[%(95%置信区间)]
| 分组及高血压亚型 | 灵敏度 (%) | 特异度 (%) | 阳性预测值 (%) | 阴性预测值 (%) | 一致性 (%) | Kappa值 |
|---|---|---|---|---|---|---|
| 已治疗患者 | ||||||
| 白大衣高血压 | 52 (43~62) | 94 (92~96) | 55 (46~65) | 93 (91~95) | 89 | 0.47a) |
| 隐匿性高血压 | 51 (43~58) | 93 (91~95) | 68 (61~76) | 87 (84~89) | 84 | 0.48a) |
| 持续性高血压 | 82 (77~86) | 92 (90~94) | 80 (75~85) | 93 (91~95) | 89 | 0.73a) |
| 未治疗患者 | ||||||
| 白大衣高血压 | 85 (69~100) | 91 (86~95) | 50 (33~67) | 98 (96~100) | 90 | 0.58a) |
| 隐匿性高血压 | 42 (28~55) | 95 (92~99) | 76 (60~91) | 82 (76~88) | 81 | 0.43a) |
| 持续性高血压 | 77 (68~87) | 98 (95~100) | 95 (90~100) | 88 (82~93) | 90 | 0.78a) |
表4
治疗组和未治疗组动态血压监测和家庭血压测量分别诊断白大衣高血压及隐匿性高血压的影响因素
| 参数 | 动态血压 | 家庭血压 | |||
|---|---|---|---|---|---|
| OR值 (95%置信区间) | P值 | OR值 (95%置信区间) | P值 | ||
| 治疗组 | |||||
| 白大衣高血压 | |||||
| 高血压病程 | 0.98 (0.96~0.99) | 0.050 0 | 0.98 (0.96~1.00) | 0.070 0 | |
| 诊室收缩压 | 1.06 (1.05~1.08) | <0.000 1 | 1.05 (1.04~1.07) | <0.000 1 | |
| 诊室舒张压 | 0.97 (0.94~0.99) | 0.020 0 | - | - | |
| 吸烟 | - | - | 2.2 (0.92~5.28) | 0.080 0 | |
| 体质量指数 | - | - | 0.94 (0.88~1.01) | 0.080 0 | |
| 心血管疾病史 | - | - | 1.78 (1.01~3.13) | 0.050 0 | |
| 服用降压药数目 | - | - | 0.75 (0.59~0.95) | 0.020 0 | |
| 隐匿性高血压 | |||||
| 年龄 | 0.82 (0.66~1.01) | 0.070 0 | - | - | |
| 体质量指数 | 1.05 (0.99~1.11) | 0.080 0 | 1.09 (1.03~1.16) | 0.006 0 | |
| 糖尿病 | 1.78 (1.06~2.97) | 0.030 0 | - | - | |
| 诊室收缩压 | 0.93 (0.92~0.95) | <0.001 0 | 0.96 (0.94~0.97) | <0.000 1 | |
| 诊室舒张压 | 1.03 (1.00~1.06) | 0.030 0 | - | - | |
| 动态血压有效读数 | 1.04 (1.00~1.07) | 0.060 0 | - | - | |
| 高血压病程 | 1.01 (1.00~1.02) | 0.080 0 | - | - | |
| 吸烟 | - | - | 0.41 (0.23~0.75) | 0.004 0 | |
| 未治疗组 | |||||
| 白大衣高血压 | |||||
| 男性 | 0.26 (0.06~1.15) | 0.080 0 | 0.40 (0.14~1.13) | 0.090 0 | |
| 诊室收缩压 | 1.07 (1.02~1.12) | 0.005 0 | 1.06 (1.02~1.10) | 0.004 0 | |
| 隐匿性高血压 | |||||
| 男性 | 4.4 (1.70~11.61) | 0.002 0 | - | - | |
| 诊室收缩压 | 0.92 (0.88~0.96) | <0.000 1 | 0.95 (0.91~0.99) | 0.020 0 | |
| 心血管疾病史 | 4.68 (0.90~24.38) | 0.070 0 | - | - | |
| [1] | Joint Committee for Guideline Revision. 2018 Chinese Guidelines for Prevention and Treatment of Hypertension-A report of the Revision Committee of Chinese Guidelines for Prevention and Treatment of Hypertension[J]. J Geriatr Cardiol, 2019, 16(3):182-241. |
| [2] |
O'Brien E1, Parati G, Stergiou G, et al. European Society of Hypertension position paper on ambulatory blood pressure monitoring[J]. J Hypertens, 2013, 31(9):1731-1768.
doi: 10.1097/HJH.0b013e328363e964 pmid: 24029863 |
| [3] | Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines[J]. Hypertension, 2018, 71(6):e13-e115. |
| [4] |
Williams B, Mancia G, Spiering W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension[J]. Eur Heart J, 2018, 39(33):3021-3104.
doi: 10.1093/eurheartj/ehy339 pmid: 30165516 |
| [5] |
Mancia G, Facchetti R, Bombelli M, et al. Long-term risk of mortality associated with selective and combined elevation in office, home, and ambulatory blood pressure[J]. Hypertension, 2006, 47(5):846-853.
doi: 10.1161/01.HYP.0000215363.69793.bb URL |
| [6] |
Franklin SS, Thijs L, Hansen TW, et al. Significance of white-coat hypertension in older persons with isolated systolic hypertension: a meta-analysis using the international database on ambulatory blood pressure monito-ring in relation to cardiovascular outcomes population[J]. hypertension, 2012, 59(3):564-571.
doi: 10.1161/HYPERTENSIONAHA.111.180653 pmid: 22252396 |
| [7] |
Parati G, Omboni S, Bilo G. Why is out-of-office blood pressure measurement needed?[J]. Hypertension, 2009, 54(2):181-187.
doi: 10.1161/HYPERTENSIONAHA.108.122853 URL |
| [8] |
Nasothimiou EG, Tzamouranis D, Rarra V, et al. Diagnosis accuracy of home vs. ambulatory blood pressure monitoring in untreated and treated hypertension[J]. Hypertension Res, 2012, 35(7):750-755.
doi: 10.1038/hr.2012.19 URL |
| [9] |
Hänninen MR, Niiranen TJ, Puukka PJ, et al. Comparison of home and ambulatory blood pressure measurement in the diagnosis of masked hypertension[J]. J Hypertens, 2010, 28(4): 709-714.
doi: 10.1097/HJH.0b013e3283369faa URL |
| [10] |
Bayó J, Cos FX, Roca C, et al. Home blood pressure self-monitoring: diagnostic performance in white-coat hypertension[J]. Blood Press Monit, 2006, 11(2): 47-52.
doi: 10.1097/01.mbp.0000200479.19046.94 URL |
| [11] |
Stergiou GS, Salgami EV, Tzamouranis DG, et al. Masked hypertension assessed by ambulatory blood pressure versus home blood pressure monitoring: is it the same phenomenon?[J]. Am J Hypertens, 2005, 18(6):772-778.
pmid: 15925734 |
| [12] |
Parati G, Stergiou GS. Self measured and ambulatory blood pressure in assessing the 'white-coat' phenomen[J]. J Hypertens, 2003, 21(4):677-682.
doi: 10.1097/00004872-200304000-00005 URL |
| [13] |
Stergiou GS, Nasothimiou E, Giovas P, et al. Diagnosis of hypertension in children and adolescents based on home versus ambulatory blood pressure monitoring[J]. J Hypertens, 2008, 26(8):1556-1562.
doi: 10.1097/HJH.0b013e328301c411 pmid: 18622232 |
| [14] |
Verdecchia P, Angeli F, Mazzotta G, et al. Home blood pressure measurements will not replace 24-hour ambulatory blood pressure monitoring[J]. Hypertension, 2009, 54(2):188-195.
doi: 10.1161/HYPERTENSIONAHA.108.122861 pmid: 19581513 |
| [1] | 沈小钰, 沙莎, 殷蕾, 周纬, 骆凝馨, 王雪峰. 儿童原发性肾病综合征动态血压变化特点的临床分析[J]. 诊断学理论与实践, 2022, 21(05): 613-618. |
| [2] | 中国高血压联盟《动态血压监测指南》委员会. 2020中国动态血压监测指南[J]. 诊断学理论与实践, 2021, 20(01): 21-36. |
| [3] | 黄剑峰, 盛长生, 黄绮芳, 程艾邦, 郭芊卉, 张冬燕, 王继光, 李燕. 门诊患者血压昼夜节律变化及相关影响因素分析[J]. 诊断学理论与实践, 2019, 18(03): 313-318. |
| [4] | 李燕, 张冬燕. 重视隐匿性高血压的筛查诊断与治疗[J]. 诊断学理论与实践, 2017, 16(06): 571-575. |
| [5] | 郭统帅, 褚超, 汪洋, 任珂宇, 牟建军. 高盐摄入及补钾干预对盐敏感个体血压昼夜节律的影响[J]. 诊断学理论与实践, 2017, 16(06): 582-586. |
| [6] | 陈卉, 郭芊卉, 许杰, 程艾邦, 张冬燕, 王颖, 黄绮芳, 盛长生, 李燕. 经颅多普勒超声研究无症状性颅内动脉狭窄的患病情况及影响因素[J]. 诊断学理论与实践, 2017, 16(06): 592-595. |
| [7] | 魏方菲, 张璐, 韩静岭, 李燕,. 单纯舒张期高血压的患病率及临床特征[J]. 诊断学理论与实践, 2012, 11(06): 568-571. |
| [8] | 张敏, 顾刚, 夏仁海, 路亘, 林玲, 付凯, 王静妮, 周沛然,. 白大衣高血压患者心率变异性的分析[J]. 诊断学理论与实践, 2010, 9(04): 372-374. |
| [9] | 张欣, 曹久妹, 王鸿珍, 何汝敏,. 老年高血压病患者动态血压参数与颈动脉内膜-中层厚度的相关性研究[J]. 诊断学理论与实践, 2007, 6(03): 228-231. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||