诊断学理论与实践 ›› 2020, Vol. 19 ›› Issue (04): 381-385.doi: 10.16150/j.1671-2870.2020.04.011
许海敏1, 陈晓炎1( ), 张静2, 杨晓群1, 王朝夫1
), 张静2, 杨晓群1, 王朝夫1
收稿日期:2020-05-20
出版日期:2020-08-25
发布日期:2022-07-15
通讯作者:
陈晓炎
E-mail:cxy11832@rjh.com.cn
XU Haimin1, CHEN Xiaoyan1(), ZHANG Jing2, YANG Xiaoqun1, WANG Chaofu1
Received:2020-05-20
Online:2020-08-25
Published:2022-07-15
Contact:
CHEN Xiaoyan
E-mail:cxy11832@rjh.com.cn
摘要:
目的: 探讨肺微囊性纤维黏液瘤(microcystic fibromyxoma,MFM)的临床和病理组织学特征、免疫表型及鉴别诊断。方法: 分析1例肺MFM患者的临床资料,包括临床表现、病理组织学特征及免疫表型,并结合相关文献进行探讨。结果: 患者为63岁男性,常规胸部X线检查发现肺结节;胸部CT示两肺有多发的大小不等的结节灶,最大者位于左肺上叶,边界光整,增强后轻度强化。予患者行左肺上叶切除术,肉眼观察手术标本,见肿瘤位于肺外周,体积为1.5 cm×1.1 cm×0.7 cm,切面呈灰红色,质地软,边界尚清;标本切片在光学显微镜下观察,可见肿瘤边界清晰,有广泛的微囊结构形成,细胞呈梭形、星芒状,无异型性,未见核分裂相,间质富于黏液,伴丰富的小血管,见散在淋巴细胞、浆细胞、肥大细胞及巨噬细胞浸润。肿瘤旁距瘤体边缘0.2 cm处另见一小瘤灶,最大径为0.2 cm,组织形态与大者相同。肿瘤细胞波形蛋白呈弥漫强阳性,其余上皮源性、肌源性、神经源性、神经内分泌、血管内皮及间皮标志均为阴性,Ki-67低表达(<1%)。荧光原位杂交检测显示EWSR1基因未见易位。患者术后12个月及18个月时复查CT检查,均显示两肺有多发小结节,右肺结节数目略有增多及增大。结论: 肺MFM是一种罕见的肺间叶源性肿瘤,组织形态以微囊和黏液为特征,免疫组织化学(免疫组化)检测显示其表达波形蛋白,确诊提示需要综合组织学形态特征和免疫组化检查结果进行判断,目前报道的肺MFM病例虽均无肿瘤复发、转移,但本例为多发性,且影像学随访结节略有增多并增大,提示其可能具有恶性潜能。
中图分类号:
许海敏, 陈晓炎, 张静, 杨晓群, 王朝夫. 肺微囊性纤维黏液瘤一例临床病理分析及文献复习[J]. 诊断学理论与实践, 2020, 19(04): 381-385.
XU Haimin, CHEN Xiaoyan, ZHANG Jing, YANG Xiaoqun, WANG Chaofu. Pulmonary microcystic fibromyxoma: a case analysis of clinical pathology and review of literature[J]. Journal of Diagnostics Concepts & Practice, 2020, 19(04): 381-385.
图1
胸部CT图像 A:CT显示左肺上叶结节(箭头);B:手术前CT显示右肺小结节(箭头);C:手术后1年CT显示右肺结节略增大(箭头)
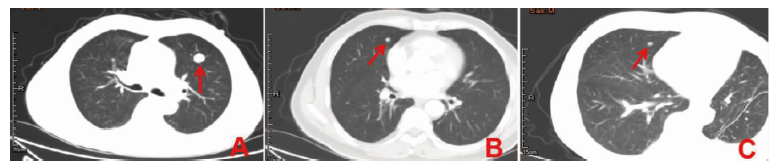

图2
肺MFM病理形态及免疫组化染色图 A:肿瘤边界清楚,肿瘤内存在广泛、大小不等的微囊(HE×100);B:肿瘤细胞呈长梭形或星芒状,异型不明显,细胞呈网络状连接,形成微囊,微囊中央为黏液(HE×400);C:肿瘤边缘可见被卷入的肺泡上皮(箭头)(HE×200);D:小瘤灶形态与大者一致(HE×100);E:肿瘤细胞呈波形蛋白弥漫强阳性(EnVision×200);F:CD34染色显示肿瘤间质富含毛细血管(EnVision法×400)
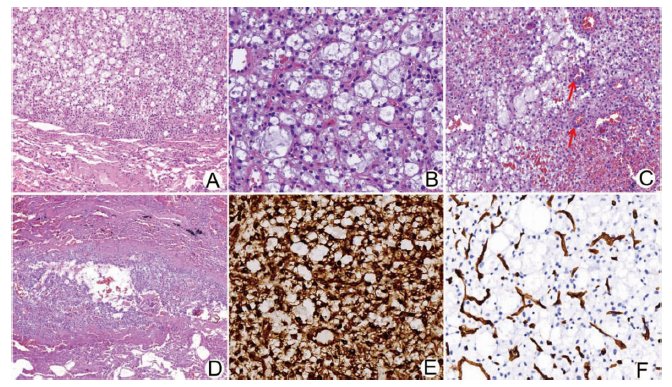
表1
肺MFM临床特征文献复习列表
| 文献 | 年龄 | 性别 | 临床症状 | 吸烟史 | 部位 | 最大径(cm)或体积(cm3) | 手术方式 | 随访 |
|---|---|---|---|---|---|---|---|---|
| Shilo等[ | 33岁 | 女 | 胸部X线检查偶然发现 | 文中未提及 | 右肺中叶周围型 | 2.3 | 楔形切除 | 术后72个月无病生存 |
| Shilo等[ | 45岁 | 男 | 胸部X线检查偶然发现 | 文中未提及 | 右肺中叶 | 1.0 | 肺叶切除 | 术后54个月无病生存 |
| Shilo等[ | 65岁 | 女 | 慢性阻塞性肺疾病 检查时发现 | 有 | 左肺下叶 | 1.3 | 楔形切除 | 术后18个月无病生存 |
| Ahn等[ | 71岁 | 男 | 偶然发现 | 文中未提及 | 左肺上叶胸膜下 | 1.0×0.8×0.7 | 楔形切除 | 术后2个月发现左肺上 叶腺癌 |
| 贡其星等[ | 58岁 | 女 | 咳嗽咳痰 | 文中未提及 | 右肺上叶 | 1.5×1.5×1.0 | 楔形切除 | 术后38个月无复发, 无转移 |
| 本例 | 63岁 | 男 | 腹股沟疝术前 检查发现 | 无 | 左肺上叶周围型 | 多灶,最大灶 1.5×1.1×0.7 | 肺叶切除 | 术后23个月无复发、无 转移,残留结节略增 多、增大 |
| [1] |
Shilo K, Miettinen M, Travis WD, et al. Pulmonary microcystic fibromyxoma: report of 3 cases[J]. Am J Surg Pathol, 2006, 30(11):1432-1435.
doi: 10.1097/01.pas.0000213279.53338.32 URL |
| [2] |
Ahn J, Kim NR, Ha SY, et al. A case of primary subpleural pulmonary microcystic myxoma coincidentally occurred with pulmonary adenocarcinoma[J]. J Pathol Transl Med, 2015, 49(3):274-278.
doi: 10.4132/jptm.2015.03.12 URL |
| [3] | 贡其星, 李海, 张智弘, 等. 肺微囊性纤维黏液瘤的临床病理学特征[J]. 中华病理学杂志, 2018, 47(2):110-113. |
| [4] | 魏建国, 王强, 张仁亚, 等. 新近认识具有黏液样特征的少见肺部肿瘤的临床病理学特征[J]. 中华病理学杂志, 2017, 46(5):352-356. |
| [5] | Travis WD, Brambilla E, Burke AP, et al. WHO classification of tumours of the lung, pleura, thymus and heart[M]. Lyon:IARC: 2015. |
| [6] |
Thway K, Nicholson AG, Lawson K, et al. Primary pulmonary myxoid sarcoma with EWSR1-CREB1 fusion: a new tumor entity[J]. Am J Surg Pathol, 2011, 35(11):1722-1732.
doi: 10.1097/PAS.0b013e318227e4d2 pmid: 21997693 |
| [7] |
Tsuta K, Kalhor N, Wistuba II, et al. Clinicopathological and immunohistochemical analysis of spindle-cell carcinoid tumour of the lung[J]. Histopathology, 2011, 59(3):526-536.
doi: 10.1111/j.1365-2559.2011.03966.x pmid: 22034892 |
| [8] |
Nannini N, Bertolini F, Cavazza A, et al. Atypical carcinoid with prominent mucinous stroma: a hitherto unreported variant of pulmonary neuroendocrine tumor[J]. Endocr Pathol, 2010, 21(2):120-124.
doi: 10.1007/s12022-010-9115-x URL |
| [9] |
Fracasso T, Varchmin-Schultheiss K. Sudden death due to pulmonary embolism from right atrial myxoma[J]. Int J Legal Med, 2009, 123(2):157-159.
doi: 10.1007/s00414-008-0312-9 pmid: 19125270 |
| [10] |
Geng J, Cao B, Wang L. Aggressive angiomyxoma: an unusual presentation[J]. Korean J Radiol, 2012, 13(1):90-93.
doi: 10.3348/kjr.2012.13.1.90 URL |
| [11] |
Kalebi AY, Hale MJ. Pulmonary metastasis from a deltoid subcutaneous low-grade fibromyxoid sarcoma with giant collagen rosettes[J]. Hum Pathol, 2008, 39(10):1553-1554.
doi: 10.1016/j.humpath.2008.06.017 pmid: 18774378 |
| [12] |
Tsuchie H, Kaya M, Nagasawa H, et al. Distant metastasis in patients with myxofibrosarcoma[J]. Ups J Med Sci, 2017, 122(3):190-193.
doi: 10.1080/03009734.2017.1356404 URL |
| [13] |
Kapoor N, Shinagare AB, Jagannathan JP, et al. Clinical and radiologic features of extraskeletal myxoid chondrosarcoma including initial presentation, local recurrence, and metastases[J]. Radiol Oncol, 2014, 48(3):235-242.
doi: 10.2478/raon-2014-0005 pmid: 25177237 |
| [14] |
D'Ambrosio FG, Shiu MH, Brennan MF. Intrapulmonary presentation of extraskeletal myxoid chondrosarcoma of the extremity. Report of two cases[J]. Cancer, 1986, 58(5):1144-1148.
pmid: 3731040 |
| [15] |
Nicolas M, Moran CA, Suster S. Pulmonary metastasis from liposarcoma: a clinicopathologic and immunohistochemical study of 24 cases[J]. Am J Clin Pathol, 2005, 123(2):265-275.
pmid: 15842053 |
| [16] |
Choi YD, Kim JH, Nam JH, et al. Aggressive angiomyxoma of the lung[J]. J Clin Pathol, 2008, 61(8):962-964.
doi: 10.1136/jcp.2008.056788 pmid: 18663059 |
| [17] |
Balanzá R, Arrangoiz R, Cordera F, et al. Pulmonary extraskeletal myxoid chondrosarcoma: a case report and lite-rature review[J]. Int J Surg Case Rep, 2016, 27:96-101.
doi: 10.1016/j.ijscr.2016.08.025 URL |
| [18] | 刘有, 张晓欢, 宋志刚, 等. 肺原发性骨外黏液样软骨肉瘤临床病理观察[J]. 诊断病理学杂志, 2019, 26(8):523-527. |
| [1] | 谢吻, 梁怀予, 董磊, 袁菲, 王朝夫, 郭滟. 胰腺导管腺癌重要驱动基因突变与临床病理特征、预后间相关性的分析[J]. 诊断学理论与实践, 2022, 21(05): 581-587. |
| [2] | 石峰, 郭竹英, 郭海艳. 新型冠状病毒肺炎患者外周血淋巴细胞亚群变化的临床意义[J]. 诊断学理论与实践, 2022, 21(05): 619-624. |
| [3] | 孙艳艳, 兰信堂. 肺癌颅脑转移患者接受放射治疗后前庭功能受损1例[J]. 诊断学理论与实践, 2022, 21(05): 632-634. |
| [4] | 张祥钦, 江勇. 宏基因组第二代测序技术诊断鹦鹉热衣原体肺炎1例[J]. 诊断学理论与实践, 2022, 21(05): 635-637. |
| [5] | 车稳, 柳蒋书, 陈晓炎, 王朝夫, 袁菲, 王璇. 肺混合性鳞状细胞和腺性乳头状瘤2例临床病理特征及冷冻切片病理诊断误诊分析[J]. 诊断学理论与实践, 2022, 21(04): 476-481. |
| [6] | 包志瑶, 孟文凯, 沈继敏, 李庆云. 成人继发于化脓性扁桃体炎的血行播散性肺炎1例报道并文献复习[J]. 诊断学理论与实践, 2022, 21(04): 520-523. |
| [7] | 杜燕然, 焦景, 任芸芸, 周建桥. 超声影像组学技术在评估胎肺成熟度中的应用[J]. 诊断学理论与实践, 2022, 21(03): 326-330. |
| [8] | 新冠病毒定点医院公共学科工作模式撰写组. 上海交通大学医学院附属瑞金医院抗击新型冠状病毒定点医院公共学科工作模式[J]. 诊断学理论与实践, 2022, 21(02): 118-127. |
| [9] | 中华医学会内分泌学分会. 新型冠状病毒肺炎疫情下骨质疏松症管理专家建议[J]. 诊断学理论与实践, 2022, 21(02): 133-135. |
| [10] | 中华医学会内分泌学分会. 新型冠状病毒肺炎疫情下肾上腺疾病管理专家建议[J]. 诊断学理论与实践, 2022, 21(02): 139-142. |
| [11] | 陈长强, 孟俊, 金佩佩, 戴菁. 定点医院新型冠状病毒肺炎患者核酸检测工作的实践和探索[J]. 诊断学理论与实践, 2022, 21(02): 143-149. |
| [12] | 施莺莺, 钟旭, 刘嘉琳, 何乐, 熊少洁, 翁懿, 丁成唯, 杨溢, 陈伟红, 邱力萍, 辛海光. 新型冠状病毒疫情相关防疫工作人员感染防控实践调查分析及对策[J]. 诊断学理论与实践, 2022, 21(02): 178-183. |
| [13] | 蒋琰, 林薇, 黄晨, 景峰. 疫情下急诊科应急物资管理模式的探索与实践[J]. 诊断学理论与实践, 2022, 21(02): 212-215. |
| [14] | 于平, 裘卫宇, 王旭, 张徐婧, 尚寒冰, 顾志冬, 林靖生, 景峰, 杨之涛, 毕宇芳, 陈尔真. 大型方舱医院药品保障管理的实践与探索[J]. 诊断学理论与实践, 2022, 21(02): 221-224. |
| [15] | 万瑾, 林婧, 丁芸, 陆琳, 成杰. 特大型城市综合性医院疫情防控期间涉医电话咨询应对模式与实践[J]. 诊断学理论与实践, 2022, 21(02): 225-228. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||