外科理论与实践 ›› 2022, Vol. 27 ›› Issue (04): 351-356.doi: 10.16139/j.1007-9610.2022.04.015
韩华中1, 徐春华1, 范文阶1, 齐志鹏2, 李冰2, 周平红2, 姚礼庆2, 钟芸诗2, 陆品相1( )
)
收稿日期:2021-02-23
出版日期:2022-07-25
发布日期:2022-09-20
通讯作者:
陆品相
E-mail:2231243202@qq.com
基金资助:
HAN Huazhong1, XU Chunhua1, FAN Wenjie1, QI Zhipeng2, LI Bing2, ZHOU Pinghong2, YAO Liqing2, ZHONG Yunshi2, LU Pinxiang1()
Received:2021-02-23
Online:2022-07-25
Published:2022-09-20
Contact:
LU Pinxiang
E-mail:2231243202@qq.com
摘要:
目的:探讨结肠直肠巨大息肉内镜黏膜下剥离术,留置肛管减压对术后恢复和预防术后并发症发生的临床意义。方法:设计前瞻性临床随机对照研究。入组结肠直肠巨大息肉(直径≥3 cm)的病人,分为内镜治疗组100例和内镜治疗加预防性肛管置入组(简称内镜肛管组)92例,比较两组术后恢复和并发症发生率。结果:内镜治疗组术后发生迟发性出血5例(5.0%),内镜肛管组2例(2.2%);内镜治疗组术后发生电凝综合征7例(7.0%),内镜肛管组发生1例(1.1%)。两组术后并发症发生的差异有统计学意义,P<0.05。术后3 d内镜治疗组平均体温(37.2±0.8) ℃,内镜肛管组平均体温(37.1±0.6)℃,两组体温差异无统计学意义。内镜肛管组的肠蠕动恢复时间(22.5±5.9) h与内镜治疗组(39.3±10.4) h的差异有统计学意义,P<0.01。内镜肛管组腹痛程度评分(2.2±1.3)分与内镜治疗组(4.7±2.2)分的差异有统计学意义,P<0.01。术后第一天腹部平片显示,内镜治疗组的肠腔较内镜肛管组明显扩张。结论:内镜黏膜下剥离结肠直肠巨大息肉术后,应用肛管减压引流是一种简单有效的预防措施,有术后恢复好,并发症发生率低的临床意义。
中图分类号:
韩华中, 徐春华, 范文阶, 齐志鹏, 李冰, 周平红, 姚礼庆, 钟芸诗, 陆品相. 内镜切除结肠直肠巨大息肉术后留置肛管减压的研究[J]. 外科理论与实践, 2022, 27(04): 351-356.
HAN Huazhong, XU Chunhua, FAN Wenjie, QI Zhipeng, LI Bing, ZHOU Pinghong, YAO Liqing, ZHONG Yunshi, LU Pinxiang. Study on transanal tube drainage after endoscopic resection of giant colorectal polyp[J]. Journal of Surgery Concepts & Practice, 2022, 27(04): 351-356.
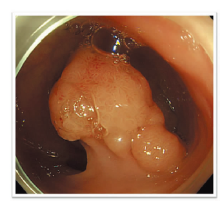
图1
结肠直肠亚蒂息肉
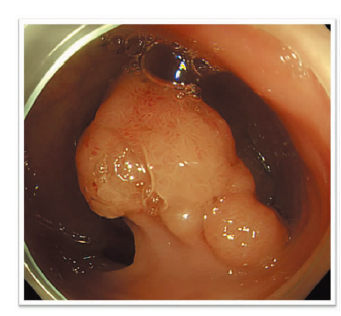
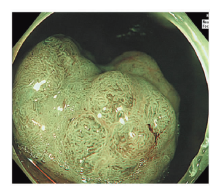
图2
结肠直肠宽基息肉
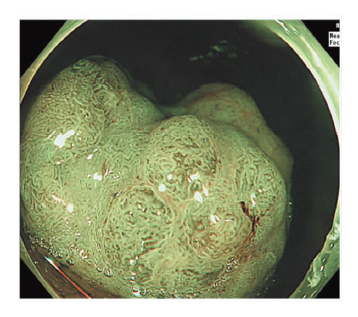
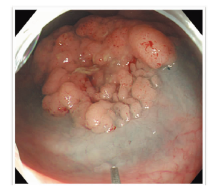
图3
结肠直肠侧向发育型息肉黏膜下注射
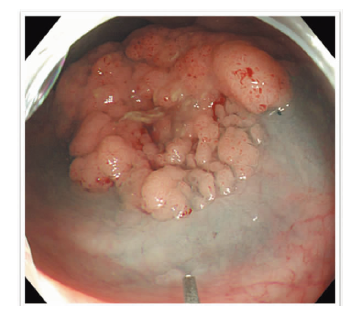
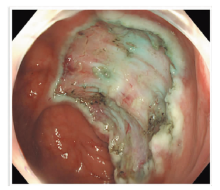
图4
剥离后创面
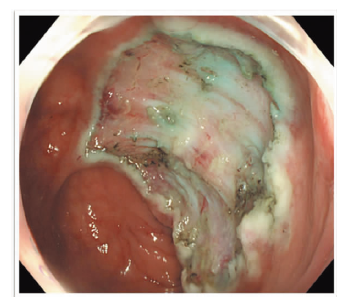
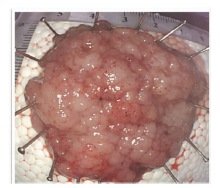
图5
切除标本
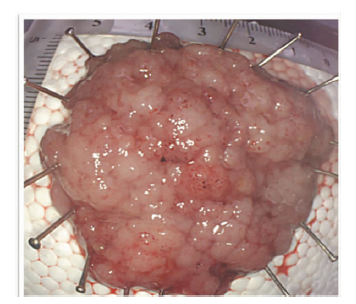
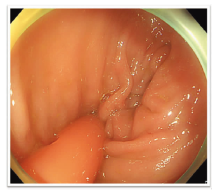
图6
内镜直视下放置肛管
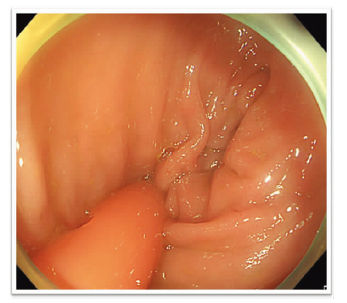

图7
疼痛评分尺

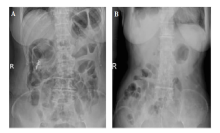
图8
腹部平片观察肠腔扩张程度 A:未留置肛管组;B:留置肛管组。
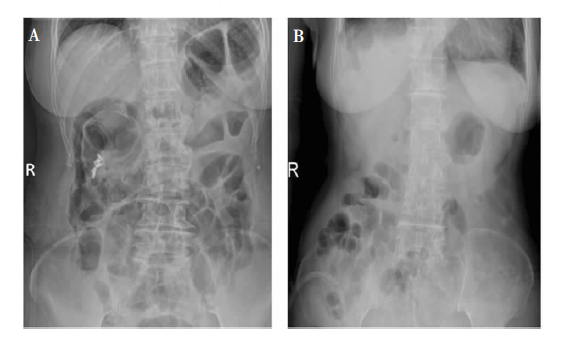
表1
两组一般资料比较[$\bar{x} \pm s$)/n(%)]
| 项目 | 内镜肛管组 (n=92) | 内镜治疗组 (n=100) | t值 | P值 |
|---|---|---|---|---|
| 病变位置 | ||||
| 右半结肠 | 19(20.7) | 22(22.0) | ||
| 左半结肠 | 23(25.0) | 27(27.0) | ||
| 直肠 | 50(54.3) | 51(51.0) | ||
| 病变直径(cm) | 4.0±0.9 | 3.9±0.9 | -0.05 | 0.96 |
| 术中穿孔 | 2a) | 0 | ||
| 术后并发症 | 3 | 12 | 17 | 0.04 |
| 迟发性出血 | 2(2.2) | 5(5.0) | ||
| 电凝综合征 | 1(1.1) | 7(7.0) | ||
| 术后3 d的体温(℃) | 37.1±0.6 | 37.2±0.8 | 0.5 | 0.7 |
| 肠蠕动恢复时间(h) | 22.5±5.9 | 39.3±10.4 | 13.7 | <0.01 |
| 腹痛程度评分(分) | 2.2±1.3 | 4.7±2.2 | 9.5 | <0.01 |
| [1] |
Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup[J]. N Engl J Med, 1993, 329(27):1977-1981.
doi: 10.1056/NEJM199312303292701 URL |
| [2] |
Heydenreich A. Endoscopic mucosal resection of flat and depressed types of early colorectal cancer[J]. Endoscopy, 1993, 25(7):455-461.
doi: 10.1055/s-2007-1010367 URL |
| [3] |
Ahmad NA, Kochman ML, Long WB, et al. Efficacy, safety, and clinical outcomes of endoscopic mucosal resection: a study of 101 cases[J]. Gastrointest Endosc, 2002, 55(3):390-396.
doi: 10.1067/mge.2002.121881 URL |
| [4] |
Zhao WT, Li NN, He D, et al. Transanal tube for the prevention of anastomotic leakage after rectal cancer surgery: a systematic review and meta-analysis[J]. World J Surg, 2017, 41(1):267-276.
doi: 10.1007/s00268-016-3758-9 URL |
| [5] | 姚礼庆, 钟芸诗, 许剑民, 等. 经肠镜导管减压术在急性低位结直肠梗阻中的应用[J]. 中华消化内镜杂志, 2006, 23(5):325-328. |
| [6] | 方三高, 魏建国, 陈真伟. WHO(2019)消化系统肿瘤分类[J]. 诊断病理学杂志,2019, 26(12):865-870. |
| [7] | 钟芸诗, 时强, 姚礼庆, 等. 内镜黏膜下剥离术后短期内胃镜检查对防治迟发性出血的价值评价[J]. 中华消化内镜杂志, 2012, 29(5):247-250. |
| [8] |
Jung D, Youn YH, Jahng J, et al. Risk of electrocoagulation syndrome after endoscopic submucosal dissection in the colon and rectum[J]. Endoscopy, 2013, 45(9):714-717.
doi: 10.1055/s-0033-1344555 URL |
| [9] |
Kandiah K, Subramaniam S, Bhandari P. Polypectomy and advanced endoscopic resection[J]. Frontline Gastroenterol, 2017, 8(2):110-114.
doi: 10.1136/flgastro-2016-100769 URL |
| [10] |
Tanaka S, Kashida H, Saito Y, et al. JGES guidelines for colorectal endoscopic submucosal dissection/endoscopic mucosal resection[J]. Dig Endosc, 2015, 27(4):417-434.
doi: 10.1111/den.12456 URL |
| [11] | 中华人民共和国卫生健康委员会医政医管局, 中华医学会肿瘤学分会. 中国结直肠癌诊疗规范(2020 年版)[J]. 中国实用外科杂志, 2020, 40(6):601-625. |
| [12] |
Hochdörffer R, Eickhoff A, Apel D, et al. Endoscopic resection of “giant” colorectal lesions: long-term outcome and safety[J]. Z Gastroenterol, 2010, 48(7):741-747.
doi: 10.1055/s-0028-1109971 pmid: 20607630 |
| [13] | 钟芸诗, 姚礼庆, 许剑民, 等. 内镜黏膜下剥离术治疗直肠扁平癌前期疾病和黏膜内癌临床价值[J]. 中国实用外科杂志, 2011, 31(6):497-500. |
| [14] |
Franklin ME Jr, Portillo G. Laparoscopic monitored colonoscopic polypectomy: long-term follow-up[J]. World J Surg, 2009, 33(6):1306-1309.
doi: 10.1007/s00268-009-9967-8 pmid: 19280252 |
| [15] |
Wilhelm D, von Delius S, Weber L, et al. Combined la-paroscopic-endoscopic resections of colorectal polyps: 10-year experience and follow-up[J]. Surg Endosc, 2009, 23(4):688-693.
doi: 10.1007/s00464-008-0282-5 pmid: 19169747 |
| [16] |
Winter H, Lang RA, Spelsberg FW, et al. Laparoscopic colonoscopic rendezvous procedures for the treatment of polyps and early stage carcinomas of the colon[J]. Int J Colorectal Dis, 2007, 22(11):1377-1381.
pmid: 17646999 |
| [17] | 蔡世伦, 钟芸诗. 结直肠黏膜下肿瘤的内镜治疗失败病例[J]. 中华结直肠疾病电子杂志, 2014, 3(6):493-494. |
| [18] |
Mlynarsky L, Zelber-Sagi S, Miller E, et al. Kariv. Endoscopic resection of large colorectal adenomas-clinical experience of a tertiary referral centre[J]. Colorectal Dis, 2018, 20(5):391-398.
doi: 10.1111/codi.13954 pmid: 29105290 |
| [19] |
Ogasawara N, Yoshimine T, Noda H, et al. Clinical risk factors for delayed bleeding after endoscopic submucosal dissection for colorectal tumors in Japanese patients[J]. Eur J Gastroenterol Hepatol, 2016, 28(12):1407-1414.
doi: 10.1097/MEG.0000000000000723 URL |
| [20] |
Kataoka Y, Tsuji Y, Sakaguchi Y, et al. Bleeding after endoscopic submucosal dissection: risk factors and preventive methods[J]. World J Gastroenterol, 2016, 22(26):5927-5935.
doi: 10.3748/wjg.v22.i26.5927 URL |
| [21] | 李冰, 周平红, 姚礼庆, 等. 内镜黏膜下剥离治疗结直肠黏膜病变术后肛管引流减压疗效分析[J]. 中国实用外科杂志, 2017, 37(7):802-805. |
| [22] |
Ito T, Obama K, Sato T, et al. Usefulness of transanal tube placement for prevention of anastomotic leakage following laparoscopic low anterior resection[J]. Asian J Endosc Surg, 2017, 10(1):17-22.
doi: 10.1111/ases.12310 URL |
| [23] |
Wang Z, Liang J, Chen J, et al. Effectiveness of a transanal drainage tube for the prevention of anastomotic leakage after laparoscopic low anterior resection for rectal cancer[J]. Asian Pac J Cancer Prev, 2020, 21(5):1441-1444.
doi: 10.31557/APJCP.2020.21.5.1441 URL |
| [24] |
Shigeta K, Okabayashi K, Baba H, et al. A meta-analysis of the use of a transanal drainage tube to prevent anastomotic leakage after anterior resection by double-stapling technique for rectal cancer[J]. Surg Endosc, 2016, 30(2):543-550.
doi: 10.1007/s00464-015-4237-3 pmid: 26091985 |
| [25] |
Wang S, Zhang Z, Liu M, et al. Efficacy of transanal tube placement after anterior resection for rectal cancer: a systematic review and meta-analysis[J]. World J Surg Oncol, 2016, 14:92.
doi: 10.1186/s12957-016-0854-0 URL |
| [26] |
Choy KT, Yang TWW, Heriot A, et al. Does rectal tube/transanal stent placement after an anterior resection for rectal cancer reduce anastomotic leak? A systematic review and meta-analysis[J]. Int J Colorectal Dis, 2021, 36(6):1123-1132.
doi: 10.1007/s00384-021-03851-8 pmid: 33515307 |
| [27] |
Xiao L, Zhang WB, Jiang PC, et al. Can transanal tube placement after anterior resection for rectal carcinoma reduce anastomotic leakage rate? A single-institution prospective randomized study[J]. World J Surg, 2011, 35(6):1367-1377.
doi: 10.1007/s00268-011-1053-3 URL |
| [28] | 中华医学会外科学分会结直肠外科学组. 中国直肠癌手术吻合口漏诊断、预防及处理专家共识(2019版)[J]. 中华胃肠外科杂志, 2019, 22(3):201-206. |
| [29] |
Kang CY, Halabi WJ, Chaudhry OO, et al. Risk factors for anastomotic leakage after anterior resection for rectal cancer[J]. JAMA Surg, 2013, 148(1):65-71.
doi: 10.1001/2013.jamasurg.2 URL |
| [30] |
Matthiessen P, Hallböök O, Andersson M, et al. Risk factors for anastomotic leakage after anterior resection of the rectum[J]. Colorectal Dis, 2004, 6(6):462-469.
pmid: 15521937 |
| [31] |
den Dulk M, Marijnen CA, Collette L, et al. Multicentre analysis of ontological and survival outcomes following anastomotic leakage after rectal cancer surgery[J]. Br J Surg, 2009, 96(9):1066-1075.
doi: 10.1002/bjs.6694 pmid: 19672927 |
| [32] | 林志东. 预防性回肠造瘘在腹腔镜中低位直肠癌切除术中的应用价值[J]. 福建医药杂志, 2018, 40(4):47-50. |
| [33] | 于浩, 王新建, 隋国龙, 等. 留置肛管与末端回肠造瘘预防中低位直肠癌前切除术后吻合口瘘的效果比较[J]. 中国实用医刊, 2018, 45(2):61-65. |
| [34] |
Zhou PH, Yao LQ, Qin XY. Endoscopic submucosal dissection for colorectal epithelial neoplasm[J]. Surg Endosc, 2009, 23(7):1546-1551.
doi: 10.1007/s00464-009-0395-5 URL |
| [1] | 徐凯, 李百文. 早期胃癌及胃癌前病变的内镜黏膜下剥离术治疗[J]. 内科理论与实践, 2023, 18(02): 102-106. |
| [2] | 李为光, 孙蕴伟, 孙菁, 张本炎, 王华枫, 钱爱华. 直径≤1 cm的直肠神经分泌肿瘤2种内镜治疗方法的比较[J]. 内科理论与实践, 2022, 17(04): 289-294. |
| [3] | 何牧野 王涵 曲明悦 王春仁. 生物材料应用于内镜黏膜下注射液的研究进展[J]. 组织工程与重建外科杂志, 2021, 17(2): 165-. |
| [4] | 孙迪, 钟芸诗. 内镜黏膜下剥离术治疗早期胃癌的现状及发展[J]. 外科理论与实践, 2019, 24(01): 27-32. |
| [5] | 周平红, 蔡明琰, 姚礼庆, 执笔,. 消化道黏膜病变内镜黏膜下剥离术的专家共识意见[J]. 诊断学理论与实践, 2012, 11(05): 531-535. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||