诊断学理论与实践 ›› 2019, Vol. 18 ›› Issue (1): 37-43.doi: 10.16150/j.1671-2870.2019.01.008
魏晓敏1, 张媛媛1, 董樑1, 夏敬文1, 龚益1,2, 喻永平3, 李圣青1
收稿日期:2019-01-31
出版日期:2019-02-25
发布日期:2019-02-25
WEI Xiaomin1, ZHANG Yuanyuan1, DONG Liang1, XIA Jingwen1, GONG Yi1,2, YU Yongping3, LI Shengqing1
Received:2019-01-31
Online:2019-02-25
Published:2019-02-25
摘要: 目的 分析初次诊断为肺栓塞症的患者,在接受足量且超过3个月的抗凝治疗后发生慢性血栓栓塞性肺动脉高压(chronic thromboembolic pulmonary hypertension,CTEPH)的发病率,并评估促使其发生CTEPH的潜在危险因素。方法 采取前瞻性研究方式,通过3年随访,评估初次诊断为肺栓塞的292例患者发展成为CTEPH的发病率及危险因素。结果 初次诊断为肺栓塞的292例患者发展成为CTEPH的累积发病率,在3个月时为9.20%,6个月为10.40%,1年为11.30%,2年为11.90%,3年为12.90%。发生CTEPH的危险因素包括,从出现肺栓塞症状到接受治疗的时间窗≥1个月(OR=9.065),肺栓塞危险程度分层为中危(OR=37.691)和重危患者(OR=33.957),肺血管分支和小分支存在血栓栓塞(OR=6.216),存在与肺栓塞发生相关的危险因素(OR=3.659)。结论 真实世界中,肺栓塞患者发生CTEPH的3年累积发病率较高,达12.90%,临床医师需重视。
中图分类号:
魏晓敏, 张媛媛, 董樑, 夏敬文, 龚益, 喻永平, 李圣青. 真实世界中肺栓塞后慢性血栓栓塞性肺动脉高压的发病及相关危险因素前瞻性研究[J]. 诊断学理论与实践, 2019, 18(1): 37-43.
WEI Xiaomin, ZHANG Yuanyuan, DONG Liang, XIA Jingwen, GONG Yi, YU Yongping, LI Shengqing. A prospective study on incidence of chronic thromboembolic pulmonary hypertension after pulmonary thromboembolism[J]. Journal of Diagnostics Concepts & Practice, 2019, 18(1): 37-43.
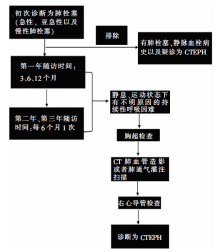
图1
患者入组流程 初次诊断为肺栓塞的患者入组后,首先排除有肺栓塞、静脉血栓以及疑诊为CTEPH的患者。随访时间为3个月、6个月、12个月,1年后至少每6个月随访1次,总随访时间为3年。随访中,患者经过至少3个月的抗凝治疗后,在静息和运动状态时出现不明原因的持续性呼吸困难,且胸部超声检查结果考虑可能为潜在的CTEPH;如果三尖瓣反流速率超过2.8 m/s,肺部灌注扫描及CT肺血管造影检查确诊存在血栓栓塞,右心导管检查诊断为肺动脉高压,则可确诊为CTEPH;所有的检查由独立的专家委员会评估
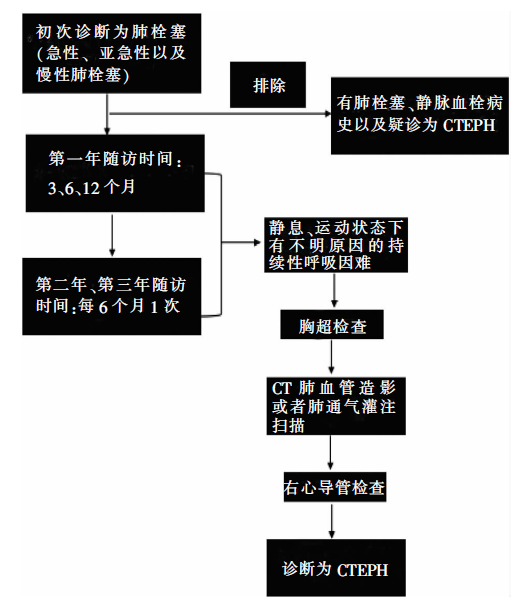
表1
PTE患者统计和临床特征
| 特征 | 肺栓塞患者(n=292) | 无肺栓塞主要危险因素(n=120) | 有肺栓塞主要危险因素(n=172) | P值 |
|---|---|---|---|---|
| 年龄 | 57.29±13.43 | 58.23±13.124 | 56.63±13.633 | 0.148秩和检验 |
| 女性 | 133(45.54%) | 60(50.00%) | 73(42.44%) | 0.202 |
| 吸烟 | 134(45.89%) | 48(40.00%) | 86(50.00%) | 0.092 |
| DVT | 225(77.05%) | 88(73.33%) | 137(79.65%) | 0.207 |
| 治疗方法 | 0.054 | |||
| 溶栓治疗 | 13(4.45%) | 2(1.67%) | 11(6.40%) | |
| 低分子量肝素+华法林 | 279(95.55%) | 118(98.33%) | 161(93.60%) | |
| 腔静脉滤器植入 | 2(0.68%) | 1(0.83%) | 1(0.58%) | 1.000Fisher检验 |
表2
肺栓塞病人危险因素发生率(n=292)
| 危险因素 | 暴露比 |
|---|---|
| 主要危险因素 | |
| Ⅴ因子增加 | 42/184(22.82%) |
| 抗凝血酶缺乏 | 28/149(18.79%) |
| 蛋白S缺乏 | 40/192(20.83%) |
| 蛋白C缺乏 | 38/186(20.43%) |
| Ⅶ因子缺乏 | 34/181(18.78%) |
| Ⅷ因子升高 | 49/180(27.22%) |
| 高同型半胱氨酸 | 134/257(52.14%) |
| 抗心磷脂抗体 | 23/194(11.86%) |
| 次要危险因素 | |
| 男性 | 159/292(54.45%) |
| 吸烟史 | 134/292(45.89%) |
| BMI≥25 | 105/292(35.96%) |
| 输血史 | 22/292(7.53%) |
| VTE史 | 7/292(2.40%) |
| 恶性肿瘤以及放化疗史 | 52/292(17.81%) |
| 血液病史 | 48/292(16.44%) |
| 传染病史 | 40/292(13.70%) |
| 慢性肺病史 | 65/292(22.26%) |
| 糖尿病史 | 24/292(8.22%) |
| 慢性心血管病史 | 86/292(29.45%) |
| 慢性肾病史 | 15/292(5.14%) |
| 慢性肝病 | 15/292(5.14%) |
| 结缔组织病 | 16/292(2.05%) |
| 外科手术史 | 68/292(23.29%) |
| 骨折固定史 | 52/292(17.81%) |
| 怀孕 | 9/292(3.08%) |
| 下肢静脉曲张 | 62/292(21.23%) |
| 高血脂 | 69/292(23.63%) |
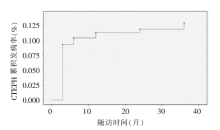
图2
初次诊断为CTEPH患者的累积发病率 CTEPH累积发病率,3个月为9.20%,6个月为10.40%,1年为11.30%,2年为11.90%,3年为12.90%
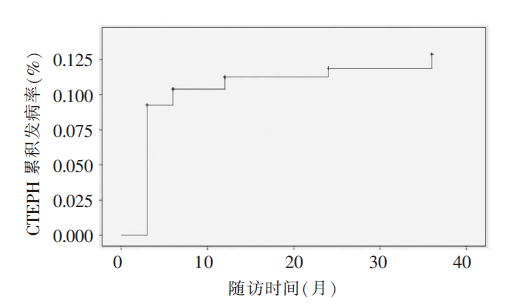
表3
CTEPH患者临床特征
| 特征 | CTEPH患者总数 (n=34) | 没有肺栓塞主要危险因素 (n=4) | 有肺栓塞主要危险因素 (n=30) | P值 |
|---|---|---|---|---|
| 年龄(岁) | 55.44±14.04 | 53.25±10.24 | 55.73±14.59 | 0.745 |
| 女性(n) | 21(61.76%) | 3(75.00%) | 18(60.00%) | 1.000 Fisher检验 |
| 深静脉血栓(n) | 20(58.82%) | 3(75.00%) | 17(56.67%) | 0.627 Fisher检验 |
| 从有症状到诊断为肺栓塞的时间(月) | 12.51±13.53 | 12.13±13.71 | 12.57±13.74 | 0.661 秩和检验 |
表4
单因素logistic回归分析CTEPH的危险因素
| 危险因素 | CTEPH(N=34) | 对照组(N=258) | OR值 | OR值95%CI | P值 |
|---|---|---|---|---|---|
| 年龄≥56(%) | 17(50.00%) | 160(62.02%) | 0.613 | (0.299~1.255) | 0.181 0 |
| 女性(%) | 21(61.76%) | 112(43.41%) | 2.106 | (1.011~4.388) | 0.047 0 |
| 有肺栓塞症状到治疗时间窗≥1个月 | 29(85.29%) | 106(41.09%) | 8.317 | (3.118~22.181) | <0.000 1 |
| 肺栓塞危险程度分层(%) | |||||
| 低度危险因素 | 1(2.94%) | 132(51.16%) | 1.000 | ||
| 中度危险因素 | 28(82.35%) | 103(39.92%) | 35.883 | (4.802~268.140) | <0.000 1 |
| 重度危险因素 | 5(14.71) | 23(8.92%) | 28.696 | (3.204~256.974) | 0.003 0 |
| 血栓定植 | |||||
| 主要分支 | 27(79.41%) | 246(95.35%) | 1.000 | ||
| 次级分支以及小分支 | 7(20.59%) | 12(4.65% ) | 5.315 | (1.929~14.641) | 0.001 0 |
| 存在肺栓塞主要危险因素 | 30(88.24%) | 142(55.04%) | 6.127 | (2.098~17.893) | 0.001 0 |
| 高同型半胱氨酸 | 26(76.47%) | 107(41.47%) | 4.182 | (1.749~9.999) | 0.001 0 |
表5
多因素logistic回归分析CTEPH的危险因素
| 危险因素 | OR值 | OR值95%CI | P值 |
|---|---|---|---|
| 肺栓塞症状到治疗时间窗<1个月 | 1.000 | ||
| 肺栓塞症状到治疗时间窗≥1个月 | 9.065 | (3.113~26.396) | <0.000 1 |
| 肺栓塞危险程度分层 | |||
| 肺栓塞低度危险 | 1.000 | ||
| 肺栓塞中度危险 | 37.691 | (4.893~290.320) | <0.000 1 |
| 肺栓塞重度危险 | 33.957 | (3.363~342.825) | 0.003 0 |
| 血栓定植部位 | |||
| 主要分支有血栓定植 | 1.000 | ||
| 次级分支以及小分支有血栓定植 | 6.216 | (1.392~27.747) | 0.017 0 |
| 肺栓塞发生相关危险因素 | |||
| 不存在肺栓塞相关危险因素 | 1.000 | ||
| 存在肺栓塞相关危险因素 | 3.659 | (1.033~12.963) | 0.044 0 |
| [1] | Konstantinides SV. 2014 ESC Guidelines on the diagnosis and management of acute pulmonary embolism[J]. Eur Heart J, 2014, 35(45):3145-3146. |
| [2] | Guérin L, Couturaud F, Parent F, et al. Prevalence of chronic thromboembolic pulmonary hypertension after acute pulmonary embolism. Prevalence of CTEPH after pulmonary embolism[J]. Thromb Haemost, 2014, 112(3):598-605. |
| [3] | Pengo V, Lensing AW, Prins MH, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism[J]. N Engl J Med, 2004, 350(22):2257-2264. |
| [4] | Poli D, Grifoni E, Antonucci E, et al. Incidence of recurrent venous thromboembolism and of chronic thromboembolic pulmonary hypertension in patients after a first episode of pulmonary embolism[J]. J Thromb Thrombolysis, 2010, 30(3):294-299. |
| [5] | Mi J, Sun ZH, Zhong MH, et al. Predictive factors of chronic thromboembolic pulmonary hypertension in patients with acute pulmonary thromboembolism[J]. Zhonghua Xin Xue Guan Bing Za Zhi, 2012, 40(6):497-501. |
| [6] | Bonderman D, Wilkens H, Wakounig S, et al. Risk factors for chronic thromboembolic pulmonary hypertension[J]. Eur Respir J, 2009, 33(2):325-331. |
| [7] | Lang I, Kerr K. Risk factors for chronic thromboembolic pulmonary hypertension[J]. Proc Am Thorac Soc, 2006, 3(7):568-570. |
| [8] | Yang S, Yang Y, Zhai Z, et al. Incidence and risk factors of chronic thromboembolic pulmonary hypertension in patients after acute pulmonary embolism[J]. J Thorac Dis, 2015, 7(11):1927-1938. |
| [9] | Klok FA, Dzikowska-Diduch O, Kostrubiec M, et al. Derivation of a clinical prediction score for chronic thromboembolic pulmonary hypertension after acute pulmonary embolism[J]. J Thromb Haemost, 2016, 14(1):121-128. |
| [10] | Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension[J]. Kardiol Pol, 2015, 73(12):1127-1206. |
| [11] | Fernandes T, Auger W, Fedullo P. Epidemiology and risk factors for chronic thromboembolic pulmonary hypertension[J]. Thromb Res, 2018, 164:145-149. |
| [12] | Fedullo PF, Auger WR, Kerr KM, et al. Chronic thromboembolic pulmonary hypertension[J]. N Engl J Med, 2001, 345(20):1465-1472. |
| [13] | Pengo V, Lensing AW, Prins MH, et al. Incidence of chronic thromboembolic pulmonary hypertension after pulmonary embolism[J]. N Engl J Med, 2004, 350(22):2257-2264. |
| [14] | Klok FA, Zondag W, van Kralingen KW, et al. Patient outcomes after acute pulmonary embolism. A pooled survival analysis of different adverse events[J]. Am J Respir Crit Care Med, 2010, 181(5):501-506. |
| [15] | Golpe R, Pérez-de-Llano LA, Castro-Añón O, et al. Right ventricle dysfunction and pulmonary hypertension in hemodynamically stable pulmonary embolism[J]. Respir Med, 2010, 104(9):1370-1376. |
| [16] | Korkmaz A, Ozlu T, Ozsu S, et al. Long-term outcomes in acute pulmonary thromboembolism: the incidence of chronic thromboembolic pulmonary hypertension and associated risk factors[J]. Clin Appl Thromb Hemost, 2012, 18(3):281-288. |
| [17] | Lang IM, Pesavento R, Bonderman D, et al. Risk factors and basic mechanisms of chronic thromboembolic pulmonary hypertension: a current understanding[J]. Eur Respir J, 2013, 41(2):462-468. |
| [18] | Ghaffary MR, Ansarin K, Sakhinia E, et al. Association of chronic thromboembolic pulmonary hypertension with hereditary and acquired risk factors for thromboembolism[J]. Acta Med Iran, 2015, 53(3):144-148. |
| [19] | Wong CL, Szydlo R, Gibbs S, et al. Hereditary and acquired thrombotic risk factors for chronic thromboembolic pulmonary hypertension[J]. Blood Coagul Fibrinolysis, 2010, 21(3):201-206. |
| [20] | Kim NH, Lang IM. Risk factors for chronic thromboembolic pulmonary hypertension[J]. Eur Respir Rev, 2012, 21(123):27-31. |
| [21] | Martinez C, Wallenhorst C, Teal S, et al. Incidence and risk factors of chronic thromboembolic pulmonary hypertension following venous thromboembolism, a population-based cohort study in England[J]. Pulm Circ, 2018, 8(3): 2045894018791358. |
| [1] | 石峰, 郭竹英, 郭海艳. 新型冠状病毒肺炎患者外周血淋巴细胞亚群变化的临床意义[J]. 诊断学理论与实践, 2022, 21(05): 619-624. |
| [2] | 孙艳艳, 兰信堂. 肺癌颅脑转移患者接受放射治疗后前庭功能受损1例[J]. 诊断学理论与实践, 2022, 21(05): 632-634. |
| [3] | 张祥钦, 江勇. 宏基因组第二代测序技术诊断鹦鹉热衣原体肺炎1例[J]. 诊断学理论与实践, 2022, 21(05): 635-637. |
| [4] | 车稳, 柳蒋书, 陈晓炎, 王朝夫, 袁菲, 王璇. 肺混合性鳞状细胞和腺性乳头状瘤2例临床病理特征及冷冻切片病理诊断误诊分析[J]. 诊断学理论与实践, 2022, 21(04): 476-481. |
| [5] | 包志瑶, 孟文凯, 沈继敏, 李庆云. 成人继发于化脓性扁桃体炎的血行播散性肺炎1例报道并文献复习[J]. 诊断学理论与实践, 2022, 21(04): 520-523. |
| [6] | 丁燕飞, 忻笑容, 周郁芬, 谢玲, 谷雷雷, 吴云林, 陈平. 上消化道溃疡伴出血患者溃疡愈合延迟的危险因素分析[J]. 诊断学理论与实践, 2022, 21(03): 312-316. |
| [7] | 杜燕然, 焦景, 任芸芸, 周建桥. 超声影像组学技术在评估胎肺成熟度中的应用[J]. 诊断学理论与实践, 2022, 21(03): 326-330. |
| [8] | 新冠病毒定点医院公共学科工作模式撰写组. 上海交通大学医学院附属瑞金医院抗击新型冠状病毒定点医院公共学科工作模式[J]. 诊断学理论与实践, 2022, 21(02): 118-127. |
| [9] | 中华医学会内分泌学分会. 新型冠状病毒肺炎疫情下骨质疏松症管理专家建议[J]. 诊断学理论与实践, 2022, 21(02): 133-135. |
| [10] | 中华医学会内分泌学分会. 新型冠状病毒肺炎疫情下肾上腺疾病管理专家建议[J]. 诊断学理论与实践, 2022, 21(02): 139-142. |
| [11] | 陈长强, 孟俊, 金佩佩, 戴菁. 定点医院新型冠状病毒肺炎患者核酸检测工作的实践和探索[J]. 诊断学理论与实践, 2022, 21(02): 143-149. |
| [12] | 施莺莺, 钟旭, 刘嘉琳, 何乐, 熊少洁, 翁懿, 丁成唯, 杨溢, 陈伟红, 邱力萍, 辛海光. 新型冠状病毒疫情相关防疫工作人员感染防控实践调查分析及对策[J]. 诊断学理论与实践, 2022, 21(02): 178-183. |
| [13] | 蒋琰, 林薇, 黄晨, 景峰. 疫情下急诊科应急物资管理模式的探索与实践[J]. 诊断学理论与实践, 2022, 21(02): 212-215. |
| [14] | 于平, 裘卫宇, 王旭, 张徐婧, 尚寒冰, 顾志冬, 林靖生, 景峰, 杨之涛, 毕宇芳, 陈尔真. 大型方舱医院药品保障管理的实践与探索[J]. 诊断学理论与实践, 2022, 21(02): 221-224. |
| [15] | 万瑾, 林婧, 丁芸, 陆琳, 成杰. 特大型城市综合性医院疫情防控期间涉医电话咨询应对模式与实践[J]. 诊断学理论与实践, 2022, 21(02): 225-228. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||