诊断学理论与实践 ›› 2019, Vol. 18 ›› Issue (03): 278-285.doi: 10.16150/j.1671-2870.2019.03.007
朱兰1, 顾圣佳1, 陈炽华1, 曹琪琪1, 周皛月2, 严福华1, 闵佶华1( )
)
收稿日期:2019-04-17
出版日期:2019-06-25
发布日期:2019-06-25
通讯作者:
闵佶华
E-mail:mjh40471@rjh.com.cn
ZHU Lan1, GU Shengjia1, CHEN Chihua1, CAO Qiqi1, ZHOU Xiaoyue2, YAN Fuhua1, MIN Jihua1()
Received:2019-04-17
Online:2019-06-25
Published:2019-06-25
Contact:
MIN Jihua
E-mail:mjh40471@rjh.com.cn
摘要:
目的: 探讨基于可变形图像配准(deformableregistration algorithms,DRA)算法的心肌形变分析在肥厚型心肌病(hypertrophic cardiomyopathy,HCM)中的诊断及预后预测价值。方法: 回顾性收集本院确诊的HCM患者23例,另招募23名年龄性别匹配的健康志愿者(对照组),均行心脏MRI扫描。HCM组按有无心肌延迟强化(late gadoli-nium enhancement,LGE)分为LGE(+)组和LGE(-)组。采用基于DRA算法的TrufiStrain软件进行心肌形变分析,测量整体径向应变峰值(global peak radial strain, GPRS)、整体环向应变峰值(global peak circumferential strain, GPCS)和整体纵向应变峰值(global peak longitudinal strain, GPLS)以及心尖部、中部和基底部的径向应变峰值(peak radial strain, PRS)、环向应变峰值(peak circumferential strain, PCS)和纵向应变峰值(peak longitudinal strain,PLS),探讨心肌形变参数在HCM中的诊断效能及其与心室壁厚度、LGE间的关系。结果: 除心尖部PCS外,HCM组的GPRS、GPCS、GPLS及基底部和中部PRS、PCS、PLS,以及心尖部的PRS、PLS均明显低于对照组(P<0.05),而HCM组的整体及各部分3个方向(环向、纵向、径向)的应变率比值均明显小于对照组(P<0.05),且LGE(-)组及对照组各部分的PRS、PCS、PLS及3个方向的舒张早期和晚期应变率比值[径向应变率比值(ratio of radial strain rate during early and late diastole,REL),环向应变率比值(ratio of circumferential strain rate during early and late diastole,CEL)和纵向应变率比值(ratio of longitudinal strain rate during early and late diastole,LEL)]均大于LGE(+)组(P<0.05)。GPRS、GPCS、GPLS、REL、CEL、LEL均与左心室心肌最大厚度明显相关(P<0.05)。GPRS、GPCS、GPLS、REL、CEL及LEL诊断HCM的曲线下面积分别为0.686、0.905、0.921、0.972、0.974及0.917,GPRS、GPCS、GPLS、REL、CEL及LEL预测HCM患者是否有LGE的曲线下面积均大于0.871。结论: 基于DRA的心肌形变分析在诊断HCM、预测HCM患者发生LGE中具有重要价值,且与心肌厚度密切相关。
中图分类号:
朱兰, 顾圣佳, 陈炽华, 曹琪琪, 周皛月, 严福华, 闵佶华. 基于可变形配准算法的心肌形变分析对肥厚型心肌病的诊断及预后预测的价值探讨[J]. 诊断学理论与实践, 2019, 18(03): 278-285.
ZHU Lan, GU Shengjia, CHEN Chihua, CAO Qiqi, ZHOU Xiaoyue, YAN Fuhua, MIN Jihua. The value of myocardial deformation analysis based on deformable registration algorithm in the diagnosis and prediction of prognosis of hypertrophic cardiomyopathy[J]. Journal of Diagnostics Concepts & Practice, 2019, 18(03): 278-285.
表1
HCM组与对照组的一般临床资料、常规左心功能参数指标比较
| 分组 | 对照组 | HCM组 | P值 |
|---|---|---|---|
| 男性(n) | 18(78.26%) | 18(78.26%) | / |
| 年龄(岁) | 50.26±8.66 | 50.70±14.18 | 0.901 |
| 身高(cm) | 167.65±4.42 | 166.57±7.15 | 0.539 |
| 体重(kg) | 65.83±65.57 | 72.17±15.00 | 0.067 |
| 心率(次/分) | 65.78±7.66 | 65.61±8.94 | 0.944 |
| BSA(m2) | 1.71±0.09 | 1.79±0.22 | 0.141 |
| EDV(mL) | 109.53±20.58 | 131.08±25.93 | 0.003 |
| EDVI(mL/m2) | 63.92±11.26 | 73.81±14.02 | 0.011 |
| ESV(mL) | 45.59±13.81 | 55.55±14.86 | 0.023 |
| ESVI(mL/m2) | 26.60±7.82 | 31.31±8.66 | 0.049 |
| EDM(g) | 82.08±17.62 | 195.57±87.64 | <0.001 |
| EDMI(g/m2) | 47.73±8.88 | 109.74±17.54 | <0.001 |
| ESM(g) | 82.63±18.73 | 194.78±16.89 | <0.001 |
| ESMI(g/m2) | 48.02±9.40 | 109.15±16.38 | <0.001 |
| SV(mL) | 63.94±9.09 | 75.53±16.17 | 0.004 |
| LVEF(%) | 59.06±6.25 | 58.00±7.86 | 0.614 |
表2
HCM组与对照组心肌应变峰值及应变率比值比较
| 部位 | 组别 | 径向应变 | 环向应变 | 纵向应变 | |||||
|---|---|---|---|---|---|---|---|---|---|
| 峰值(%) | 率比值 | 峰值(%) | 率比值 | 峰值(%) | 率比值 | ||||
| 整体 | 对照组 | 29.08±5.87 | 3.42±0.67 | -15.43±1.43 | 2.67±1.45 | -12.92±1.85 | 2.28±0.55 | ||
| HCM组 | 23.77±10.14 | 1.73±0.55 | -11.15±3.55 | 1.45±0.90 | -8.16±4.34 | 1.18±0.54 | |||
| P值 | 0.037 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
| 基底部 | 对照组 | 38.33±9.02 | 3.34±0.69 | -17.15±2.53 | 2.78±0.76 | -22.90±3.34 | 2.16±0.68 | ||
| HCM组 | 23.81±11.42 | 1.66±0.99 | -11.88±3.60 | 1.67±1.36 | -15.34±5.85 | 1.41±0.79 | |||
| P值 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
| 中部 | 对照组 | 38.25±8.08 | 3.73±1.04 | -16.64±2.37 | 3.51±1.18 | -20.41±3.31 | 3.05±1.28 | ||
| HCM组 | 24.29±10.90 | 1.65±0.90 | -11.70±4.86 | 1.65±1.39 | -14.28±6.39 | 1.43±0.76 | |||
| P值 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | |||
| 心尖部 | 对照组 | 37.97±7.74 | 3.61±1.04 | -17.45±2.49 | 3.15±1.25 | -20.48±3.90 | 2.54±1.10 | ||
| HCM组 | 27.34±10.37 | 1.95±1.15 | -15.11±6.93 | 1.98±1.44 | -16.35±6.82 | 1.78±1.06 | |||
| P值 | <0.001 | <0.001 | 0.139 | 0.005 | 0.016 | 0.02 | |||
表3
不同心肌LGE组的应变峰值对比
| 部位 | LGE分组 | 例数(n) | 径向应变(%) | P值 | 环向应变(%) | 纵向应变(%) | P值 | ||
|---|---|---|---|---|---|---|---|---|---|
| 基底部 | HCM组 | + | 16 | 18.44±8.37 | <0.001a) | -10.09±2.03 | <0.001a) | -13.61±4.17 | <0.001a) |
| - | 7 | 36.07±7.15 | <0.001b) | -15.98±3.00 | <0.001b) | -20.02±3.83 | <0.001b) | ||
| 对照组 | 23 | 38.33±9.02 | 0.538c) | -17.15±2.53 | 0.310c) | -22.90±3.34 | 0.080c) | ||
| P值 | <0.001 | <0.001 | <0.001 | ||||||
| 中部 | HCM组 | + | 16 | 18.86±5.99 | <0.001b) | -9.40±3.21 | <0.001a) | -13.26±5.66 | 0.003a) |
| - | 7 | 36.70±9.35 | <0.001b) | -16.94±3.83 | <0.001b) | -19.35±3.13 | <0.001b) | ||
| 对照组 | 23 | 38.25±8.08 | 0.633c) | -16.64±2.37 | 0.839c) | -20.41±3.31 | 0.566c) | ||
| P值 | 0.002 | <0.001 | <0.001 | ||||||
| 心尖部 | HCM组 | + | 10 | 17.5±5.22 | <0.001b) | -9.79±2.47 | <0.001a) | -10.41±3.57 | <0.001a) |
| - | 13 | 34.91±5.84 | <0.001b) | -19.2±6.45 | <0.001b) | -20.92±4.87 | <0.001b) | ||
| 对照组 | 23 | 37.97±7.74 | 0.118c) | -16.28±5.28 | 0.215c) | -20.48±3.90 | 0.772c) | ||
| P值 | <0.001 | <0.001 | <0.001 |
表4
不同部位心肌LGE的峰值应变率比值对比分析
| 部位 | 分组 | LGE | 例数 | 径向比值 | P值 | 环向比值 | P值 | 纵向比值 | P值 |
|---|---|---|---|---|---|---|---|---|---|
| 基底部 | HCM | + | 16 | 1.13±0.47 | <0.001a) | 0.90±0.49 | <0.001a) | 0.98±0.36 | <0.001a) |
| - | 7 | 2.87±0.79 | <0.001b) | 3.40±1.05 | <0.001b) | 2.41±0.55 | <0.001b) | ||
| 对照组 | 23 | 3.73±1.04 | 0.155c) | 2.78±0.76 | 0.049c) | 2.16±0.68 | 0.317c) | ||
| P值 | 0.001 | <0.001 | <0.001 | ||||||
| 中部 | HCM | + | 16 | 1.17±0.49 | <0.001a) | 0.96±0.58 | <0.001a) | 1.03±0.39 | 0.004a) |
| - | 7 | 2.75±0.56 | <0.001b) | 3.23±1.44 | <0.001b) | 2.36±0.54 | <0.001b) | ||
| 对照组 | 23 | 3.45±1.13 | 0.007c) | 3.51±1.18 | 0.896c) | 3.05±1.28 | 0.103c) | ||
| P值 | <0.001 | <0.001 | <0.001 | ||||||
| 心尖部 | HCM | + | 10 | 1.13±0.36 | <0.001a) | 2.59±1.15 | <0.001a) | 3.61±1.04 | <0.001a) |
| - | 13 | 2.59±1.15 | <0.001b) | 2.38±1.83 | <0.001b) | 3.15±1.25 | <0.001b) | ||
| 对照组 | 23 | 3.61±1.04 | 0.008c) | 3.15±1.25 | 0.426c) | 2.54±1.10 | 0.817c) | ||
| P值 | <0.001 | <0.001 | <0.001 |
图1
对照组与LGE(+)的HCM患者的对比图 A:1例男性志愿者延迟增强的中部心肌无LGE;B:同一志愿者形变分析图(彩条示径向应变);C:另1例男性HCM患者延迟增强的中部心肌明显LGE;D:同一患者形变分析图(彩条示径向应变)
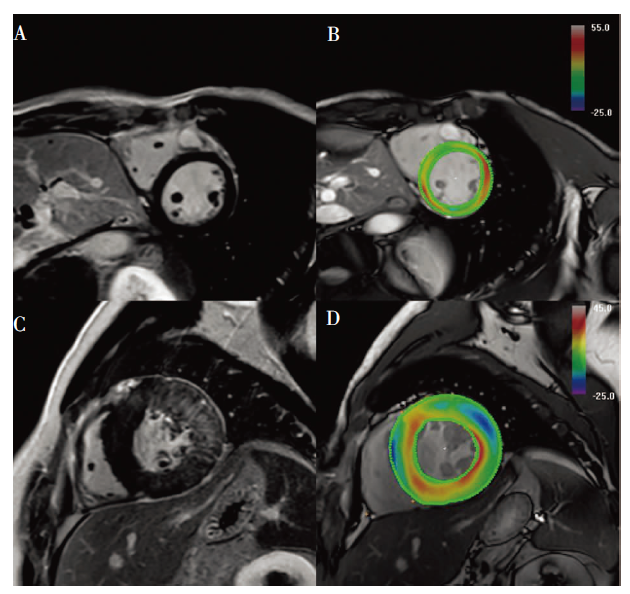
表5
HCM患者不同LGE亚组的心肌最大厚度组间差异比较
| 部位 | LGE | 例数 | 心肌最大厚度(mm) | P值 |
|---|---|---|---|---|
| 基底部 | LGE (+) | 16 | 15.21±4.02 | 0.012 |
| LGE (-) | 7 | 21.48±5.36 | ||
| 中部 | LGE (+) | 16 | 17.83±3.27 | 0.336 |
| LGE (-) | 7 | 16.07±5.26 | ||
| 心尖部 | LGE (+) | 10 | 12.37±4.39 | 0.007 |
| LGE (-) | 13 | 17.58±3.90 |
表6
心肌厚度与应变及应变率比值之间相关关系分析
| 参数 | 基底部心肌厚度 [(19.57±5.72) mm] | 中部心肌厚度 [(17.30±3.94) mm] | 心尖部心肌厚度 [(14.64±4.87) mm] | 整体心肌厚度 [(17.17±5.23) mm] | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| r值 | P值 | r值 | P值 | r值 | P值 | r值 | P值 | ||||
| PRS | -0.454 | 0.029 | -0.348 | 0.103 | -0.410 | 0.052 | -0.422 | <0.001 | |||
| PCS | 0.513 | 0.012 | 0.350 | 0.101 | 0.413 | 0.05 | 0.446 | <0.001 | |||
| PLS | 0.408 | 0.054 | 0.363 | 0.089 | 0.588 | 0.003 | -0.498 | <0.001 | |||
| REL | -0.662 | 0.001 | -0.222 | 0.309 | -0.453 | 0.030 | -0.540 | <0.001 | |||
| CEL | -0.582 | 0.004 | -0.448 | 0.032 | -0.604 | 0.002 | 0.449 | <0.001 | |||
| LEL | -0.398 | 0.06 | -0.471 | 0.023 | -0.586 | 0.003 | -0.504 | <0.001 | |||
表7
ROC曲线分析结果
| 参数 | 特异度(%) | 灵敏度(%) | 最佳临界值 | 曲线下面积 | P值 | |
|---|---|---|---|---|---|---|
| GPRS | LGE(+)与LGE(-) | 92.59 | 90.48 | ≤25.96 | 0.965(0.890,0.994) | <0.001 |
| HCM与对照组 | 95.65 | 47.83 | ≤28.31 | 0.686(0.533,0.815) | <0.001 | |
| GPCS | LGE(+)与LGE(-) | 88.89 | 85.71 | >-11.46 | 0.922(0.832,0.973) | <0.001 |
| HCM与对照组 | 91.3 | 86.96 | >-12.44 | 0.905(0.782,0.972) | <0.001 | |
| GPLS | LGE(+)与LGE(-) | 85.19 | 78.57 | >-17.38 | 0.884(0.784,0.948) | <0.001 |
| HCM与对照组 | 100 | 78.26 | >-17.46 | 0.921(0.802,0.980) | <0.001 | |
| REL | LGE(+)与LGE(-) | 92.59 | 90.48 | ≤2.00 | 0.962(0.885,0.993) | <0.001 |
| HCM与对照组 | 100 | 86.96 | ≤2.26 | 0.972(0.874,0.999) | <0.001 | |
| CEL | LGE(+)与LGE(-) | 100 | 69.57 | ≤2.12 | 0.871(0.740,0.952) | <0.001 |
| HCM与对照组 | 92.59 | 92.86 | ≤1.67 | 0.974(0.904,0.997) | <0.001 | |
| LEL | LGE(+)与LGE(-) | 92.59 | 95.24 | ≤1.57 | 0.980(0.913,0.999) | <0.001 |
| HCM与对照组 | 86.96 | 86.96 | ≤1.46 | 0.917(0.797,0.978) | <0.001 |
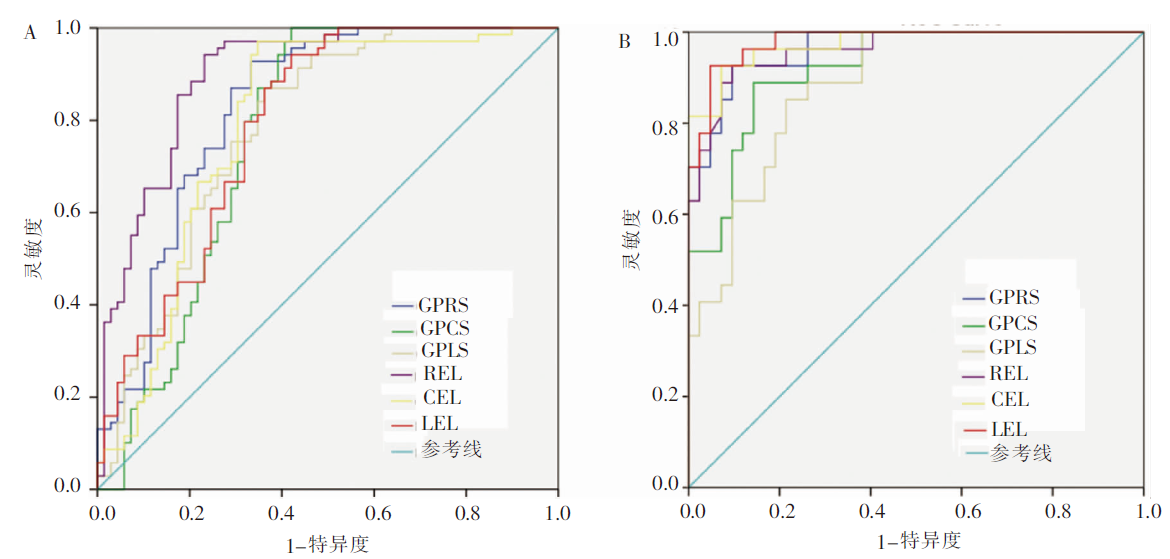
图2
ROC曲线分析 A:ROC法分析整体应变和应变率比值诊断HCM的效能;B:ROC法分析整体应变和应变率比值预测HCM患者发生心肌LGE的效能
| [1] |
Maron BJ, Maron MS. Hypertrophic cardiomyopathy[J]. Lancet, 2013, 381(9862):242-255.
doi: 10.1016/S0140-6736(12)60397-3 URL |
| [2] | Maron BJ. Hypertrophic cardiomyopathy: a systematic review[J]. JAMA, 2002, 287(10):1308-1320. |
| [3] |
Basso C, Thiene G, Corrado D, et al. Hypertrophic cardiomyopathy and sudden death in the young: pathologic evidence of myocardial ischemia[J]. Hum Pathol, 2000, 31(8):988-998.
pmid: 10987261 |
| [4] |
Gersh BJ, Maron BJ, Bonow RO, et al. 2011 ACCF/AHA guideline for the diagnosis and treatment of hypertrophic cardiomyopathy: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines[J]. J Am Coll Cardiol, 2011, 58(25):2703-2738.
doi: 10.1016/j.jacc.2011.10.825 URL |
| [5] |
Authors/Task Force members, Elliott PM, Anastasakis A, et al. 2014 ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: the Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2014, 35(39):2733-2779.
doi: 10.1093/eurheartj/ehu284 pmid: 25173338 |
| [6] |
Ismail TF, Jabbour A, Gulati A, et al. Role of late gadolinium enhancement cardiovascular magnetic resonance in the risk stratification of hypertrophic cardiomyo-pathy[J]. Heart, 2014, 100(23):1851-1858.
doi: 10.1136/heartjnl-2013-305471 URL |
| [7] | 王辉, 晏子旭, 姜红, 等. 心脏磁共振应变分析在临床前期心尖肥厚型心肌病中的应用[J]. 中国医学影像学杂志, 2019, 27(1):1-5. |
| [8] | 李雪莲, 黄为, 高见书, 等. 延迟增强磁共振成像预测肥厚型心肌病心肌纤维化与不良终点事件相关性的Meta分析[J]. 临床放射学杂志, 2018, 37(11):1824-1829. |
| [9] | 李元程, 王杰, 陈玉成. 肥厚型心肌病基因型与磁共振表型的关联性研究进展[J]. 心血管病学进展, 2019, 40(2):157-161. |
| [10] | 桑银保. 磁共振成像对肥厚性心肌病诊断及临床意义的探讨研究[J]. 大家健康(下旬版), 2015, 9(9):71-72. |
| [11] |
O'Hanlon R, Grasso A, Roughton M, et al. Prognostic significance of myocardial fibrosis in hypertrophic cardiomyopathy[J]. J Am Coll Cardiol, 2010, 56(11):867-874.
doi: 10.1016/j.jacc.2010.05.010 pmid: 20688032 |
| [12] |
Kraigher-Krainer E, Shah AM, Gupta DK, et al. Impaired systolic function by strain imaging in heart failure with preserved ejection fraction[J]. J Am Coll Cardiol, 2014, 63(5):447-456.
doi: 10.1016/j.jacc.2013.09.052 pmid: 24184245 |
| [13] | Macron L, Redheuil A, Ashrafpoor G, et al. Global circumferential left ventricular strain impairment in hypertrophic cardiomyopathy: comparison to left ventricular hypertrophy and late gadolinium enhancement[J]. J of Cardiovasc Magn Reson, 2013, 15(S1). |
| [14] |
Orwat S, Kempny A, Diller GP, et al. Cardiac magnetic resonance feature tracking: a novel method to assess myocardial strain. Comparison with echocardiographic speckle tracking in healthy volunteers and in patients with left ventricular hypertrophy[J]. Kardiol Pol, 2014, 72(4):363-371.
doi: 10.5603/KP.a2013.0319 URL |
| [15] |
Haland TF, Almaas VM, Hasselberg NE, et al. Strain echocardiography is related to fibrosis and ventricular arrhythmias in hypertrophic cardiomyopathy[J]. Eur Heart J Cardiovasc Imaging, 2016, 17(6):613-621.
doi: 10.1093/ehjci/jew005 pmid: 26873460 |
| [16] |
Gao H, Allan A, McComb C, et al. Left ventricular strain and its pattern estimated from cine CMR and validation with DENSE[J]. Phys Med Biol, 2014, 59(13):3637-3656.
doi: 10.1088/0031-9155/59/13/3637 URL |
| [17] |
Wang J, Li W, Sun J, et al. Improved segmental myocardial strain reproducibility using deformable registration algorithms compared with feature tracking cardiac MRI and speckle tracking echocardiography[J]. J Magn Reson Imaging, 2018, 48(2):404-414.
doi: 10.1002/jmri.25937 pmid: 29283466 |
| [18] | Meng L, Lin K, Collins J, et al. Automated Description of Regional Left Ventricular Motion in Patients With Cardiac Amyloidosis: A Quantitative Study Using Heart Deformation Analysis[J]. Am J Roentgenol, 2017, 209(2):W57-W63. |
| [19] | 陈炎, 陈亚蓓, 陶荣芳. 欧洲心脏病学会2014年肥厚性心肌病诊断管理指南要点介绍[J]. 中国实用内科杂志, 2015, 35(S1):170-172. |
| [20] |
Nucifora G, Muser D, Gianfagna P, et al. Systolic and diastolic myocardial mechanics in hypertrophic cardiomyopathy and their link to the extent of hypertrophy, replacement fibrosis and interstitial fibrosis[J]. Int J Cardiovasc Imaging, 2015, 31(8):1603-1610.
doi: 10.1007/s10554-015-0720-0 pmid: 26210792 |
| [21] |
Hinojar R, Fernández-Golfín C, González-Gómez A, et al. Prognostic implications of global myocardial mechanics in hypertrophic cardiomyopathy by cardiovascular magnetic resonance feature tracking. Relations to left ventricular hypertrophy and fibrosis[J]. Int J Cardiol, 2017, 249:467-472.
doi: S0167-5273(17)30710-6 pmid: 29121751 |
| [22] |
Popescu BA, Ro?ca M. Imaging of myocardial fibrosis in hypertrophic cardiomyopathy: what is the gold standard?[J]. Heart, 2014, 100(8):605-606.
doi: 10.1136/heartjnl-2013-305359 pmid: 24459293 |
| [23] |
Germans T, Rüssel IK, Gütte MJ, et al. How do hypertrophic cardiomyopathy mutations affect myocardial function in carriers with normal wall thickness? Assessment with cardiovascular magnetic resonance[J]. J Cardiovasc Magn Reson, 2010, 12:13.
doi: 10.1186/1532-429X-12-13 URL |
| [24] | Kino A, Carr J, Bonow R, et al. Association of Left Ventricular Wall Thickness and Myocardial Fibrosis/Scar with Adverse Events in Hypertrophic Cardiomyopathy: Interaction of Maximal Wall Thickness and Late Gadolinium Enhancement by Cardiac Magnetic Resonance[C]. J Am College Cardiol, 2012, 59(13):. |
| [25] |
Bogarapu S, Puchalski MD, Everitt MD, et al. Novel Cardiac Magnetic Resonance Feature Tracking (CMR-FT) Analysis for Detection of Myocardial Fibrosis in Pediatric Hypertrophic Cardiomyopathy[J]. Pediatr Cardiol, 2016, 37(4):663-673.
doi: 10.1007/s00246-015-1329-8 URL |
| [26] |
Reant P, Mirabel M, Lloyd G, et al. Global longitudinal strain is associated with heart failure outcomes in hypertrophic cardiomyopathy[J]. Heart, 2016, 102(10):741-747.
doi: 10.1136/heartjnl-2015-308576 URL |
| [1] | 刘鹏, 严福华, 秦乐, 肖瑞杰. 肥厚型心肌病左室舒张功能的心脏磁共振心肌应变率参数与猝死风险关系的研究[J]. 诊断学理论与实践, 2022, 21(03): 317-325. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||