诊断学理论与实践 ›› 2021, Vol. 20 ›› Issue (03): 271-278.doi: 10.16150/j.1671-2870.2021.03.008
王也飞1, 吴蓓颖2, 夏文权1, 陈宁1, 胡翊群3
WANG Yefei1, WU Beiying2, XIA Wenquan1, HU Yiqun1
摘要:
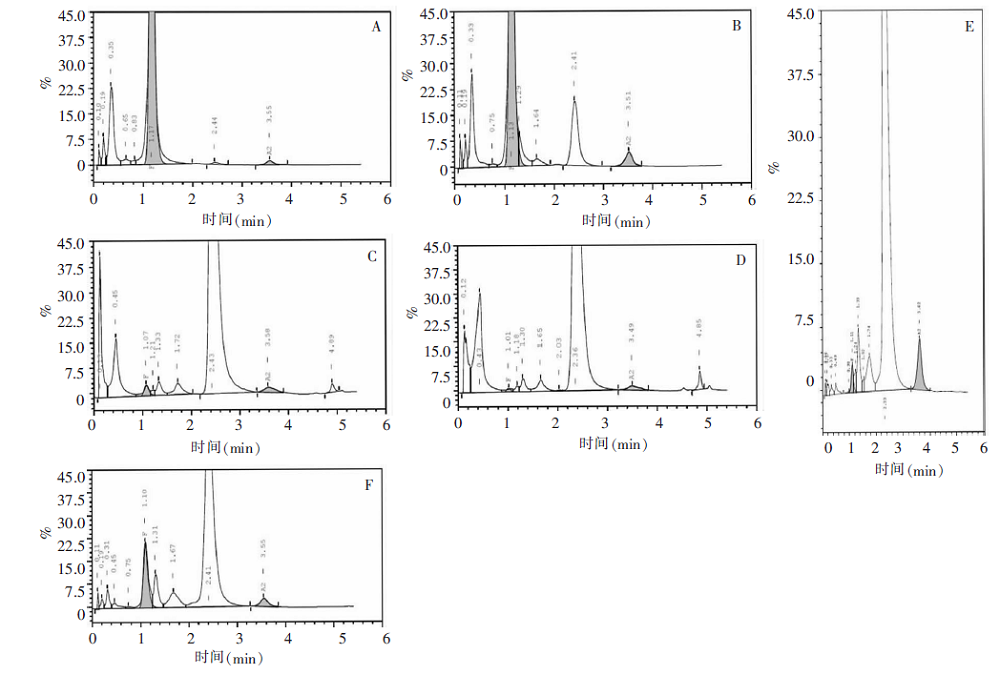
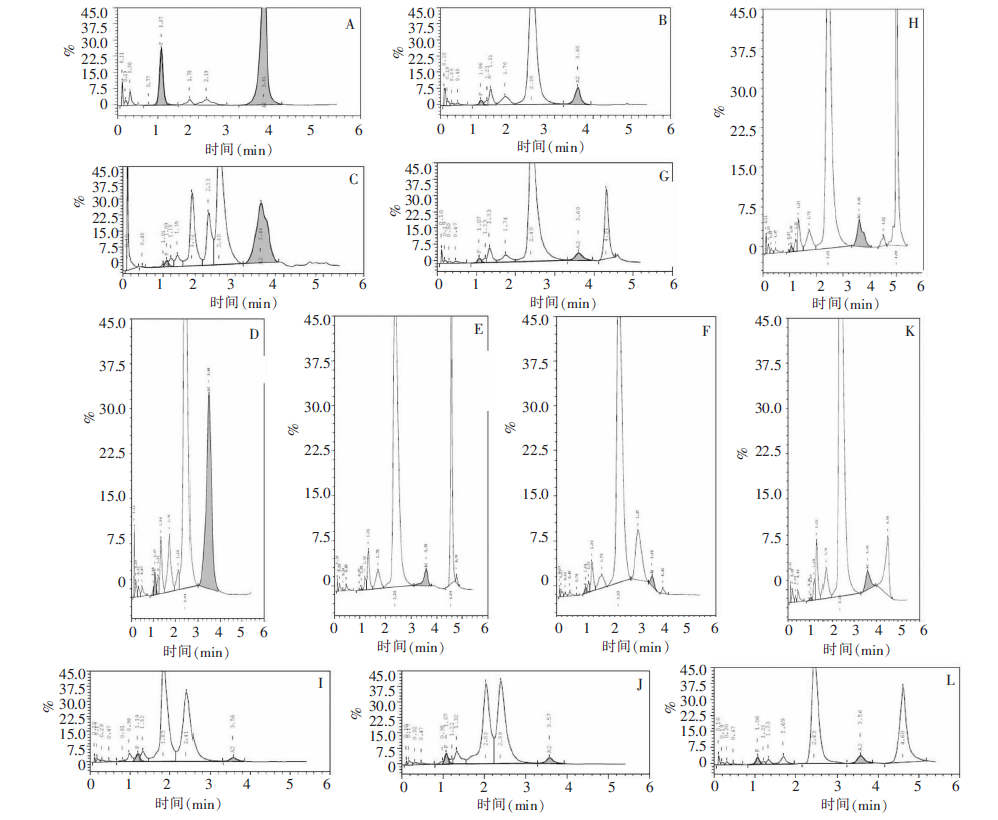
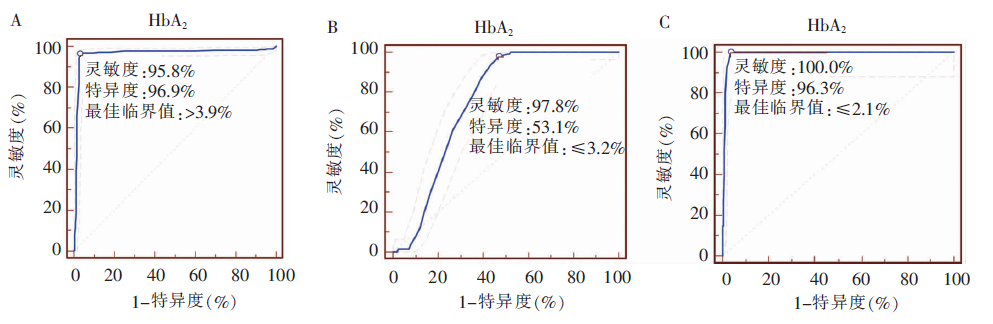
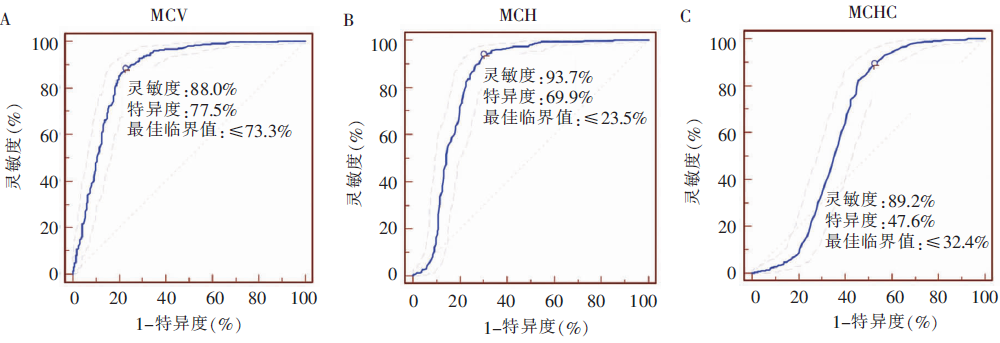
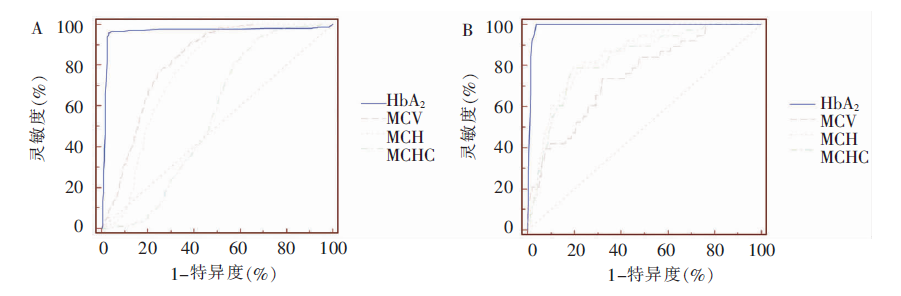
目的:探讨高效液相色谱(high performance liquid chromatography, HPLC)技术和红细胞参数在血红蛋白(hemoglobin, Hb)病筛查中的实际应用价值。方法:应用HPLC技术对1 029例临床疑似Hb病患者及进行溶血性贫血筛查者的血样本进行Hb分析,同时采用缺口聚合酶链反应、反向斑点杂交和珠蛋白基因DNA测序对样本进行基因分析;记录并分析患者的血常规红细胞参数。结果:1 029例血样本中,有591例(57.43%)确诊为珠蛋白生成障碍性贫血,14例(1.36%)确诊为异常Hb病。以基因分析结果为诊断金标准,应用HPLC检测β-珠蛋白生成障碍性贫血,以血红蛋白A2(hemoglobin A2, HbA2)3.9%为临界值, HbA2>3.9%诊断β-珠蛋白生成障碍性贫血的灵敏度为95.84%,特异度为96.87%,阳性预测值为95.40%,阴性预测值为97.20%,受试者操作特征曲线下面积(area under curve, AUC)为0.962;以HbA2 2.1%为临界值,HbA2≤2.1%结合出现快速区带来诊断中间型α-珠蛋白生成障碍性贫血[又称血红蛋白H(hemoglobin H, HbH)病]的灵敏度为100.00%,特异度为96.32%,阳性预测值为52.60%,阴性预测值为100.00%,AUC为0.990;以HbA2 3.2%为临界值,HbA2≤3.2%诊断静止型和标准型α-珠蛋白生成障碍性贫血的灵敏度为97.76%,特异度为53.11%,阳性预测值为24.0%,阴性预测值为99.4%,AUC为0.753。分别以平均红细胞体积(mean corpuscular volume, MCV)≤73.3 fl,平均红细胞血红蛋白量(mean corpuscular hemoglobin, MCH)≤23.5 pg,平均红细胞血红蛋白浓度(mean corpuscular hemoglobin contentration, MCHC)≤324 g/L诊断珠蛋白生成障碍性贫血,其灵敏度和特异度分别为87.98%和77.51%,93.73%和69.86%,89.20%和47.61%。结论:在红细胞参数测定的基础上,应用HPLC检测筛查β-珠蛋白生成障碍性贫血、HbH病和异常Hb病的灵敏度、特异度高,与基因分析结果间有较高的一致性,且操作简便、快速,适用于临床快速筛查;但对于静止型和标准型α-珠蛋白生成障碍性贫血,HPLC检测的筛查特异度和阳性预测值均较低,易造成漏诊。
中图分类号: