诊断学理论与实践 ›› 2023, Vol. 22 ›› Issue (06): 573-578.doi: 10.16150/j.1671-2870.2023.06.010
倪仲馨, 陈慧( )
)
收稿日期:2023-06-05
出版日期:2023-12-25
发布日期:2024-03-18
通讯作者:
陈慧 E-mail:ruienyun@163.com基金资助:
NI Zhongxin, CHEN Hui()
Received:2023-06-05
Published:2023-12-25
Online:2024-03-18
摘要:
目的: 研究国际卵巢肿瘤分析组织(International Ovarian Tumor Analysis,IOTA)附件多元模型(Assessment of Different NEoplasias in the adneXa, ADNEX)术前鉴别转移性卵巢癌与原发性卵巢癌的临床价值。方法: 收集2016年3月至2021年4月在我院行手术治疗的卵巢恶性肿瘤患者术前予超声检查,并记录模型预判结果,以术后病理结果为金标准,计算ADNEX模型纳入、不纳入CA125时鉴别转移性与原发性卵巢癌的灵敏度、特异度及受试者操作特征(receiver operating characteristic,ROC)曲线下面积。结果: 本研究纳入卵巢恶性肿瘤患者共197例,其中原发性卵巢癌153例(Ⅰ期36例,Ⅱ~Ⅳ期117例),转移性卵巢癌44例。ADNEX模型不纳入CA125时,鉴别转移性与原发性卵巢癌的ROC曲线下面积为0.621(95%置信区间为0.534~0.708),灵敏度为93.2%,特异度为31.4%;ADNEX模型纳入CA125时,鉴别转移性与原发性卵巢癌的ROC曲线下面积为0.810(95%置信区间为0.747~0.872),灵敏度为79.5%,特异度为69.3%。ADNEX模型纳入与不纳入CA125结果间差异有统计学意义(P<0.001)。结论: ADNEX模型对于转移性与原发性卵巢癌的鉴别有较好的临床价值,纳入CA125能提高模型的诊断效能。
中图分类号:
倪仲馨, 陈慧. ADNEX模型鉴别转移性与原发性卵巢癌的诊断效能研究[J]. 诊断学理论与实践, 2023, 22(06): 573-578.
NI Zhongxin, CHEN Hui. Study on the diagnostic efficacy of ADNEX model in differentiating metastatic and primary ovarian cancer[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(06): 573-578.
表1
197例卵巢癌的肿瘤分类
| Histological type | n (%) |
|---|---|
| Primary ovarian malignant | 153 (77.66) |
| Serous carcinoma | 105 (53.30) |
| Clear cell carcinoma | 15 (7.61) |
| Ovarian endometrioid carcinoma | 15 (7.61) |
| Carcinosarcoma | 3 (1.52) |
| Mucinous carcinoma | 6 (3.05) |
| Neuroendocrine carcinomas | 2 (1.02) |
| Immature teratomas | 2 (1.02) |
| Granular cell tumor | 2 (1.02) |
| Dysgerminomas | 1 (0.51) |
| Malignant Brenner tumor | 1 (0.51) |
| Ovarian endometrioid carcinoma + clear cell carcinoma | 1 (0.51) |
| Ovarian metastasis | 44 (22.34) |
表2
原发性与转移性卵巢癌的临床及超声特征
| Variables | Overall | OC Stages Ⅰ | OC Stages Ⅱ-Ⅳ | Ovarian metastasis | P |
|---|---|---|---|---|---|
| Overall [n (%)] | 197 (100%) | 36 (18.27) | 117 (59.39) | 44 (22.34) | - |
| Age [years, median (IQR)] | 55.00(48.00-63.00) | 56.50(47.00-63.00) | 58.00(51.00-64.00) | 50.00(38.75-56.50) | <0.001 |
| Menopause [n (%)] | 0.014 | ||||
| Yes | 126 (63.96) | 24 (66.67) | 82 (70.09) | 20 (45.45) | |
| No | 71 (36.04) | 12 (33.33) | 35 (29.91) | 24 (54.55) | |
| CA125 [U/mL, median (IQR)] | 210.60(39.10-883.30) | 59.30(15.08-311.68) | 596.20(122.20-2162.80) | 37.95(13.25-102.68) | <0.001 |
| Maximum diameter of lesion, mm, median (IQR) | 77.00(51.00-111.00) | 91.00(70.00-148.00) | 70.00(44.00-100.00) | 80.50(57.50-117.75) | 0.017 |
| Solid tissue present [n (%)] | 195 (98.98) | 35 (97.22) | 117 (100.00) | 43 (97.73) | 0.164 |
| Maximum diameter of largest solid component, if present, mm, median (IQR) | 56.00(37.00-82.00) | 50.00(33.00-63.50) | 52.00(34.00-85.00) | 68.00(51.50-90.50) | 0.038 |
| Papillary projections present [n (%)] | 0.260 | ||||
| 0 | 161 (81.73) | 26 (72.22) | 95 (81.20) | 40 (90.91) | |
| 1 | 7 (3.55) | 1 (2.78) | 5 (4.27) | 1 (2.27) | |
| 2 | 3 (1.52) | 0 (0.00) | 3 (2.56) | 0 (0.00) | |
| ≥3 | 26 (13.20) | 9 (25.00) | 14 (11.97) | 3 (6.82) | |
| More than 10 locules [n (%)] | 33 (16.75) | 7 (19.44) | 15 (12.82) | 11 (25.00) | 0.163 |
| Ascites [n (%)] | 48 (24.37) | 3 (8.33) | 41 (35.04) | 4 (9.09) | <0.001 |
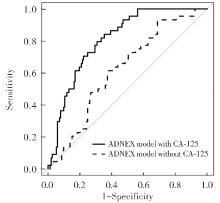
图1
ADNEX模型鉴别原发与转移癌ROC曲线
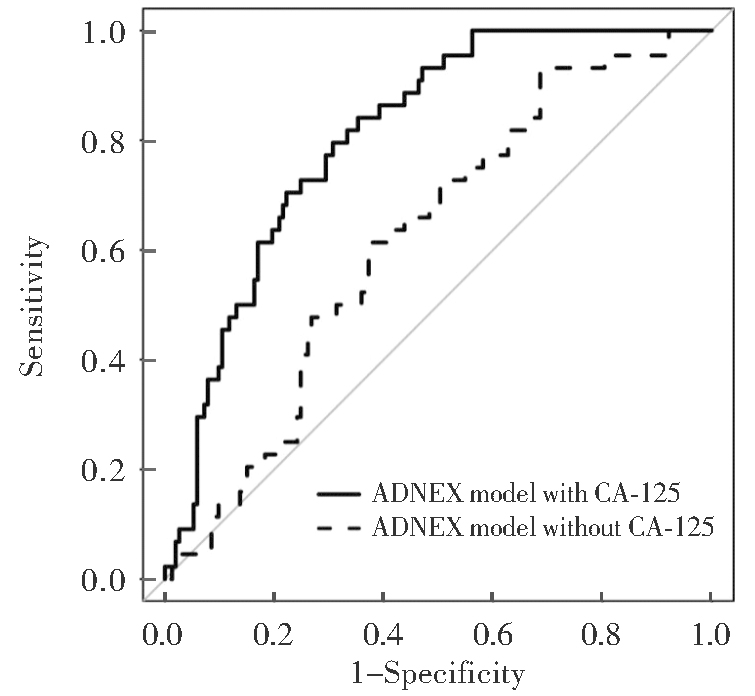
表3
ADNEX模型纳入与不纳入CA125 的ROC曲线下面积
| Discrimination | AUC (95%CI) | P | |
|---|---|---|---|
| ADNEX model with CA125 | ADNEX model without CA125 | ||
| Primary OC vs metastasis | 0.810 (0.747-0.872) | 0.621 (0.534-0.708) | <0.001 |
| Stage Ⅰ OC vs stages Ⅱ-Ⅳ OC | 0.826 (0.745-0.907) | 0.771 (0.687-0.854) | 0.156 |
| Stage Ⅰ OC vs metastasis | 0.620 (0.486-0.754) | 0.654 (0.524-0.784) | 0.033 |
| Stages Ⅱ-Ⅳ OC vs metastasis | 0.890 (0.839-0.940) | 0.710 (0.624-0.796) | <0.001 |
表4
ADNEX模型对原发和转移性卵巢癌的鉴别效能
| Discrimination | ADNEX model | Sensitivity (95%CI) | Specificity (95%CI) | PPV (95%CI) | NPV (95%CI) | LR+ (95%CI) | LR- (95%CI) | Optimal cutoff value |
|---|---|---|---|---|---|---|---|---|
| Primary OC vs metastasis | With CA125 | 0.795 (0.676-0.915) | 0.693 (0.620-0.766) | 0.427 (0.320-0.534) | 0.922 (0.873-0.971) | 2.589 (1.955-3.430) | 0.295 (0.163-0.534) | 0.140 |
| Without CA125 | 0.932 (0.857-1.000) | 0.314 (0.240- 0.387) | 0.281 (0.208- 0.354) | 0.941 (0.877-1.006) | 1.358 (1.188-1.552) | 0.217 (0.071-0.664) | 0.110 | |
| Stage Ⅰ OC vs stages Ⅱ-Ⅳ OC | With CA125 | 0.701 (0.618-0.784) | 0.833 (0.712- 0.955) | 0.932 (0.879-0.984) | 0.462 (0.340-0.583) | 4.205 (2.006-8.813) | 0.359 (0.262-0.491) | 0.840 |
| Without CA125 | 0.821 (0.751-0.890) | 0.639 (0.482-0.796) | 0.881 (0.820-0.942) | 0.523 (0.375-0.670) | 2.272 (1.459-3.538) | 0.281 (0.178-0.444) | 0.691 | |
| Stage Ⅰ OC vs metastasis | With CA125 | 0.727 (0.596-0.859) | 0.639 (0.482-0.796) | 0.711 (0.579-0.844) | 0.657 (0.500-0.814) | 2.014 (1.258-3.225) | 0.427 (0.248-0.734) | 0.381 |
| Without CA125 | 0.841 (0.733-0.949) | 0.556 (0.393-0.718) | 0.698 (0.575-0.822) | 0.741 (0.575-0.906) | 1.892 (1.285-2.787) | 0.286 (0.137-0.600) | 0.297 | |
| Stages Ⅱ-Ⅳ OC vs metastasis | With CA125 | 0.841 (0.733-0.949) | 0.803 (0.731-0.875) | 0.617 (0.494-0.740) | 0.931 (0.881-0.980) | 4.278 (2.901-6.307) | 0.198 (0.100-0.393) | 0.239 |
| Without CA125 | 0.795 (0.676-0.915) | 0.607 (0.518-0.695) | 0.432 (0.324-0.540) | 0.887 (0.818-0.957) | 2.023 (1.544-2.651) | 0.337 (0.185-0.615) | 0.208 |
表5
ADNEX模型在不同临界值时纳入和不纳入CA125的总体效能
| ADNEX model | Cutoff value | Sensitivity (95%CI) | Specificity (95%CI) | PPV(95%CI) | NPV(95%CI) | LR+(95%CI) | LR-(95%CI) |
|---|---|---|---|---|---|---|---|
| With CA125 | 0.10 | 0.886 (0.793-0.980) | 0.549 (0.470-0.628) | 0.361 (0.271-0.452) | 0.944 (0.896-0.992) | 1.965 (1.602-2.411) | 0.207 (0.090-0.478) |
| 0.15 | 0.750 (0.622-0.878) | 0.706 (0.634-0.778) | 0.423 (0.313-0.533) | 0.908 (0.856-0.960) | 2.550 (1.891-3.438) | 0.354 (0.210-0.597) | |
| 0.20 | 0.614 (0.470-0.758) | 0.810 (0.748-0.873) | 0.482 (0.351-0.613) | 0.879 (0.826-0.933) | 3.237 (2.164-4.844) | 0.477 (0.326-0.697) | |
| 0.25 | 0.477 (0.330-0.625) | 0.876 (0.824-0.928) | 0.525 (0.370-0.680) | 0.854 (0.798-0.909) | 3.843 (2.280-6.479) | 0.597 (0.447-0.797) | |
| Without CA125 | 0.10 | 0.932 (0.857-1.000) | 0.288 (0.216-0.359) | 0.273 (0.202-0.345) | 0.936 (0.866-1.006) | 1.308 (1.150-1.487) | 0.237 (0.077-0.727) |
| 0.15 | 0.727 (0.596-0.859) | 0.477 (0.398-0.556) | 0.286 (0.202-0.369) | 0.859 (0.785-0.933) | 1.391 (1.099-1.761) | 0.572 (0.343-0.952) | |
| 0.20 | 0.250 (0.122-0.378) | 0.778 (0.712-0.844) | 0.244 (0.119-0.370) | 0.783 (0.717-0.848) | 1.125 (0.623-2.032) | 0.964 (0.797-1.167) | |
| 0.25 | 0.045 (0.000- 0.107) | 0.967 (0.939-0.995) | 0.286 (0.000-0.620) | 0.779 (0.720-0.838) | 1.391 (0.279-6.925) | 0.987 (0.919-1.059) |
| [1] | HEINTZ A, ODICINO F, MAISONNEUVE P, et al. Carcinoma of the Ovary[J]. INT J GYNECOL OBSTET, 2006, 95:S161-S192. |
| [2] |
JAYSON G C, KOHN E C, KITCHENER H C, et al. Ovarian cancer[J]. The Lancet, 2014, 384(9951):1376-1388.
doi: 10.1016/S0140-6736(13)62146-7 URL |
| [3] |
SIEGEL R L, MILLER K D, JEMAL A. Cancer statistics, 2019[J]. CA Cancer J Clin, 2019, 69(1):7-34.
doi: 10.3322/caac.v69.1 URL |
| [4] |
TESTA A C, FERRANDINA G, TIMMERMAN D, et al. Imaging in gynecological disease (1): ultrasound features of metastases in the ovaries differ depending on the origin of the primary tumor[J]. Ultrasound Obstet Gynecol, 2007, 29(5):505-511.
doi: 10.1002/uog.v29:5 URL |
| [5] |
CHEONG J H, HYUNG W J, CHEN J, et al. Survival benefit of metastasectomy for Krukenberg tumors from gastric cancer[J]. Gynecol Oncol, 2004, 94(2):477-482.
pmid: 15297191 |
| [6] | TIMMERMAN D, PLANCHAMP F, BOURNE T, et al. ESGO/ISUOG/IOTA/ESGE Consensus Statement on preoperative diagnosis of ovarian tumors[J]. Ultrasound Obstet Gynecol, 2021, 58(1):148-168. |
| [7] |
FROYMAN W, LANDOLFO C, DE COCK B, et al. Risk of complications in patients with conservatively managed ovarian tumours (IOTA5): a 2-year interim analysis of a multicentre, prospective, cohort study[J]. Lancet Oncol, 2019, 20(3):448-458.
doi: S1470-2045(18)30837-4 pmid: 30737137 |
| [8] |
TIMMERMAN D, VALENTIN L, BOURNE T H, et al. Terms, definitions and measurements to describe the sonographic features of adnexal tumors: a consensus opi-nion from the International Ovarian Tumor Analysis (IOTA) Group[J]. Ultrasound Obstet Gynecol, 2000, 16(5):500-505.
doi: 10.1046/j.1469-0705.2000.00287.x URL |
| [9] |
TIMMERMAN D, TESTA A C, BOURNE T, et al. Logistic regression model to distinguish between the benign and malignant adnexal mass before surgery: a multicenter study by the International Ovarian Tumor Analysis Group[J]. J Clin Oncol. 2005, 23(34):8794-8801.
doi: 10.1200/JCO.2005.01.7632 pmid: 16314639 |
| [10] |
TIMMERMAN D, TESTA A C, BOURNE T, et al. Simple ultrasound-based rules for the diagnosis of ovarian cancer[J]. Ultrasound Obstet Gynecol, 2008, 31(6):681-690.
doi: 10.1002/uog.5365 pmid: 18504770 |
| [11] |
VAN CALSTER B, VAN HOORDE K, VALENTIN L, et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: prospective multicentre diagnostic study[J]. BMJ, 2014, 349:g5920.
doi: 10.1136/bmj.g5920 URL |
| [12] |
MEINHOLD-HEERLEIN I, FOTOPOULOU C, HARTER P, et al. The new WHO classification of ova-rian, fallopian tube, and primary peritoneal cancer and its clinical implications[J]. Arch Gynecol Obstet, 2016, 293(4):695-700.
doi: 10.1007/s00404-016-4035-8 URL |
| [13] |
PRAT J; FIGO Committee on Gynecologic Oncology. Staging classification for cancer of the ovary, fallopian tube, and peritoneum[J]. Int J Gynaecol Obstet, 2014, 124(1):1-5.
doi: 10.1016/j.ijgo.2013.10.001 pmid: 24219974 |
| [14] |
MORO F, PASCIUTO T, DJOKOVIC D, et al. Role of CA125/CEA ratio and ultrasound parameters in identifyi-ng metastases to the ovaries in patients with multilocular and multilocular-solid ovarian masses[J]. Ultrasound Obstet Gynecol, 2019, 53(1):116-123.
doi: 10.1002/uog.2019.53.issue-1 URL |
| [15] |
SZUBERT S, WOJTOWICZ A, MOSZYNSKI R, et al. External validation of the IOTA ADNEX model performed by two independent gynecologic centers[J]. Gynecol Oncol, 2016, 142(3):490-495.
doi: 10.1016/j.ygyno.2016.06.020 pmid: 27374142 |
| [16] |
EPSTEIN E, VAN CALSTER B, TIMMERMAN D, et al. Subjective ultrasound assessment, the ADNEX model and ultrasound-guided tru-cut biopsy to differentiate disseminated primary ovarian cancer from metastatic non-ovarian cancer[J]. Ultrasound Obstet Gynecol, 2016, 47(1):110-116.
doi: 10.1002/uog.14892 pmid: 25925783 |
| [17] |
MEYS E M J, JEELOF L S, ACHTEN N M J, et al. Estimating risk of malignancy in adnexal masses: external validation of the ADNEX model and comparison with other frequently used ultrasound methods[J]. Ultrasound Obstet Gynecol, 2017, 49(6):784-792.
doi: 10.1002/uog.17225 pmid: 27514486 |
| [18] |
ARAUJO K G, JALES R M, PEREIRA P N, et al. Performance of the IOTA ADNEX model in preoperative discrimination of adnexal masses in a gynecological oncolo-gy center[J]. Ultrasound Obstet Gynecol, 2017, 49(6):778-783.
doi: 10.1002/uog.2017.49.issue-6 URL |
| [19] |
CHEN H, QIAN L, JIANG M, et al. Performance of IOTA ADNEX model in evaluating adnexal masses in a gynecological oncology center in China[J]. Ultrasound Obstet Gynecol, 2019, 54(6):815-822.
doi: 10.1002/uog.20363 pmid: 31152572 |
| [20] |
WESTWOOD M, RAMAEKERS B, LANG S, et al. Risk scores to guide referral decisions for people with suspected ovarian cancer in secondary care: a systematic review and cost-effectiveness analysis[J]. Health Technol Assess, 2018, 22(44):1-264.
doi: 10.3310/hta22440 pmid: 30165935 |
| [21] |
SAYASNEH A, FERRARA L, DE COCK B, et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model: a multicentre external validation study[J]. Br J Cancer, 2016, 115(5):542-548.
doi: 10.1038/bjc.2016.227 |
| [22] | VAN CALSTER B, VALENTIN L, FROYMAN W, et al. Validation of models to diagnose ovarian cancer in patients managed surgically or conservatively: multicentre cohort study[J]. BMJ, 2020,370:m2614. |
| [23] |
NUNES N, AMBLER G, FOO X, et al. Use of IOTA simple rules for diagnosis of ovarian cancer: meta-analysis[J]. Ultrasound Obstet Gynecol, 2014, 44(5):503-514.
doi: 10.1002/uog.13437 pmid: 24920435 |
| [24] |
ZIKAN M, FISCHEROVA D, PINKAVOVA I, et al. Ultrasonographic appearance of metastatic non-gynecological pelvic tumors[J]. Ultrasound Obstet Gynecol, 2012, 39(2):215-225.
doi: 10.1002/uog.10068 pmid: 21845744 |
| [25] | 薛改琴, 陈敏华, 苗润琴, 等. 超声对胃肠道恶性肿瘤继发卵巢转移癌的诊断价值[J]. 中国超声医学杂志, 2002, 18(12):946-948. |
| XUE G Q, CHEN M H, MIAO R Q, et al. Diagnostic value of ultrasound in ovarian metastatic carcinoma secondary to gastrointestinal malignancy[J]. Chin J Ultrasound Med, 2002, 18(12):946-948. | |
| [26] |
HART W R. Diagnostic challenge of secondary (metastatic) ovarian tumors simulating primary endometrioid and mucinous neoplasms[J]. Pathol Int, 2005, 55(5):231-243.
pmid: 15871720 |
| [1] | 李伟伟, 詹维伟, 周伟, 陶玲玲, 王怡, 樊金芳, 费圆欣, 况李君, 徐文颖. 超微血管三维立体成像技术在乳腺癌血流分布模式中的应用[J]. 诊断学理论与实践, 2019, 18(2): 139-143. |
| [2] | 漆玖玲, 徐辉雄, 崔爱平, 周毓青, 赵学军,. 早孕期超声法判断双胎绒毛膜性的临床研究[J]. 诊断学理论与实践, 2013, 12(05): 504-507. |
| [3] | 龚菁菁, 崔爱平, 周毓青,. 产前超声在诊断先天性肺囊腺瘤畸形及预后分析中的价值[J]. 诊断学理论与实践, 2013, 12(01): 100-103. |
| [4] | 李俊来, 宋阳光,. 超声检查在诊断下肢深静脉急性血栓中的应用[J]. 诊断学理论与实践, 2008, 7(03): 258-262. |
| [5] | 金亚萍,龚新环,陈克敏. 急性胰腺炎致门静脉血栓形成的超声诊断[J]. 诊断学理论与实践, 2004, 3(04): 75-77. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||