诊断学理论与实践 ›› 2024, Vol. 23 ›› Issue (02): 162-172.doi: 10.16150/j.1671-2870.2024.02.010
刘娟1, 殷丽娟2, 范德生1( )
)
收稿日期:2023-11-07
出版日期:2024-04-25
发布日期:2024-07-04
通讯作者:
范德生 E-mail:hellen4099@126.com基金资助:
LIU Juan1, YIN Lijuan2, FAN Desheng1()
Received:2023-11-07
Published:2024-04-25
Online:2024-07-04
摘要:
目的:探索雄激素受体(androgen receptor,AR)、S期激酶相关蛋白2(S-phase kinase-associated protein 2,SKP2)、性别决定区Y相关的HMG盒含因子10(sry-related HMG box-containing factor 10,SOX10)、程序性死亡配体1(programmed death-ligand 1,PD-L1)及肿瘤浸润性淋巴细胞(tumor infiltrating lymphocyte,TIL)在三阴性乳腺癌(triple negative breast cancer,TNBC)表达与临床病理特征和预后的关系。方法:根据苏木精-伊红染色(hematoxylin-eosin, HE)染色切片评判109例TNBC瘤巢内TIL的比例,采用Leica Bond-Max全自动免疫组化仪检测TNBC组织中AR、SKP2、SOX10、PD-L1的表达。分析以上各生物指标与临床病理特征间的关系,并采用kaplan-Meier、Log-rank进行生存分析。结果:95例患者获得随访,中位随访时间为48个月,中位无病生存时间(disease-free survival, DFS)为42个月,中位总生存时间(overall survival, OS)48个月。在TNBC中,AR阳性表达与淋巴结转移阴性(P=0.009)、肿瘤最大径<2 cm(P=0.008)相关,TIL高表达与低级别TNBC相关(P=0.007),SKP2阳性表达与神经/脉管侵犯阳性(P=0.011)、高级别TNBC相关(P=0.002),SOX10阳性表达与淋巴结转移阳性(P=0.022)、高级别TNBC(P=0.005)相关,PD-L1阳性表达与淋巴结转移阳性(P=0.020)、神经/脉管侵犯阳性(P=0.006)、高级别TNBC(P=0.042)相关。生存分析显示,SKP2、SOX10阳性表达与更差的DFS(P=0.007、P<0.001)和OS(P=0.013、P<0.001)相关,TIL高表达与更好的DFS(P=0.016)及OS(P=0.004)相关。在生物表志物的联合表达中,AR+/SKP2-、AR+/SOX10-与更好的DFS(P=0.004、P<0.001)及OS(P=0.007、P=0.001)相关,SOX10+/低TIL、PD-L1+/低TIL与更差的DFS(P<0.001、P=0.008)及OS(P=0.001、P=0.002)相关,AR-/低TIL者具有更差的OS(P=0.014)。SKP2(HR=4.143,95%CI为1.578~10.875)、SOX10(HR=7.578,95%CI为2.067~27.782)的阳性表达是影响TNBC患者DFS的独立预后因子,SKP2(HR=3.758,95%CI为1.400~10.084)、SOX10(HR=5.131,95%CI为1.316~20.000)及TIL(HR=0.375,95%CI为0.154~0.917)的阳性表达是TNBC患者OS的独立预后因子(P均<0.05)。结论:在TNBC中,AR阳性、TIL高表达与具有更好预后的临床病理特征相关,SKP2、SOX10和PD-L1与具侵袭性的临床病理特征相关。SKP2、SOX10及TIL表达与TNBC预后相关,提示这些生物指标可能成为TNBC新的预后因子,同时它们也有可能成为潜在的治疗靶点。
中图分类号:
刘娟, 殷丽娟, 范德生. AR、SKP2、SOX10、PD-L1及TIL表达在三阴性乳腺癌中的意义[J]. 诊断学理论与实践, 2024, 23(02): 162-172.
LIU Juan, YIN Lijuan, FAN Desheng. The clinicopathologic significance of AR, SKP2, SOX10, PD-L1 and TILs expression in triple-negative breast cancer[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(02): 162-172.
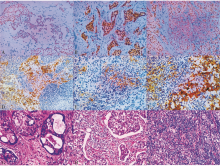
图1
AR(A)、SKP2(B)、SOX10(C)在TNBC的表达 PD-L1在TNBC肿瘤细胞(D)、间质TIL(E)、肿瘤细胞和间质TIL(F)的共同表达(Envision法,×200);TNBC中TIL的低表达(G)、中度表达(H)、高表达(I)(HE,×200)。

表1
AR、SKP2、SOX10在TNBC表达与各临床病理因素的关系
| clinicopathological features | n | AR positive (%) | χ2 | P | SKP2 positive (%) | χ2 | P | SOX10 positive (%) | χ2 | P |
|---|---|---|---|---|---|---|---|---|---|---|
| Age (year) | 1.195 | 0.274 | 0.006 | 0.940 | 1.330 | 0.249 | ||||
| <50 | 36 | 6(16.7) | 16(44.4) | 17(47.2) | ||||||
| ≥50 | 73 | 19(26.0) | 33(45.2) | 43(58.9) | ||||||
| Maximum tumor diameter (cm) | 6.960 | 0.008 | 0.097 | 0.755 | 0.614 | 0.433 | ||||
| <2 | 23 | 10(43.5) | 11(47.8) | 11(47.8) | ||||||
| ≥2 | 86 | 15(17.4) | 38(44.2) | 49(57.0) | ||||||
| Histological grade | 2.484 | 0.115 | 9.722 | 0.002 | 7.934 | 0.005 | ||||
| Low | 42 | 13(31.0) | 11(26.2) | 16(38.1) | ||||||
| High | 67 | 12(17.9) | 38(56.7) | 44(65.7) | ||||||
| Lymph node metastasis | 6.767 | 0.009 | 0.172 | 0.679 | 5.231 | 0.022 | ||||
| Negative | 58 | 19(32.8) | 25(43.1) | 26(44.8) | ||||||
| Positive | 51 | 6(11.8) | 24(47.1) | 34(66.7) | ||||||
| Nerve/vascular invasion | 1.319 | 0.251 | 6.478 | 0.011 | 1.177 | 0.278 | ||||
| Negative | 91 | 19(20.9) | 36(39.6) | 48(52.7) | ||||||
| Positive | 18 | 6(33.3) | 13(72.2) | 12(66.7) |
表2
PD-L1、TIL在TNBC中的表达与各临床病理因素间的关系
| Clinicopathological features | n | PD-L1 positive (%) | χ2 | P | low TIL (%) | moderate TIL (%) | high TIL (%) | χ2 | P |
|---|---|---|---|---|---|---|---|---|---|
| Age (year) | 0.392 | 0.531 | 1.127 | 0.569 | |||||
| <50 | 36 | 14(38.9) | 15(41.7) | 16(44.4) | 5(13.9) | ||||
| ≥50 | 73 | 33(45.2) | 24(32.9) | 34(46.6) | 15(20.5) | ||||
| Maximum tumor diameter (cm) | 0.826 | 0.363 | 1.401 | 0.496 | |||||
| <2 | 23 | 8(34.8) | 7(30.4) | 13(56.5) | 3(13.0) | ||||
| ≥2 | 86 | 39(45.3) | 32(37.2) | 37(43.0) | 17(19.8) | ||||
| Histological grade | 4.124 | 0.042 | 9.894 | 0.007 | |||||
| Low | 42 | 13(31.0) | 9(21.4) | 20(47.6) | 13(31.0) | ||||
| High | 67 | 34(50.7) | 30(44.8) | 30(44.8) | 7(10.4) | ||||
| Lymph node metastasis | 5.425 | 0.020 | 2.281 | 0.320 | |||||
| Negative | 58 | 19(32.8) | 17(29.3) | 29(50.0) | 12(20.7) | ||||
| Positive | 51 | 28(54.9) | 22(43.1) | 21(41.2) | 8(15.7) | ||||
| Nerve/vascular invasion | 7.446 | 0.006 | 0.715 | 0.699 | |||||
| Negative | 91 | 34(37.4) | 31(34.1) | 43(47.3) | 17(18.7) | ||||
| Positive | 18 | 13(72.2) | 8(44.4) | 7(38.9) | 3(16.7) |
表3
TNBC各临床病理特征对DFS、OS影响的单因素分析
| Clinicopathological features | Patients n=95 | Patients with relapse and metastasis n=31(%) | Dead patients n=26(%) | DFS | OS | |||
|---|---|---|---|---|---|---|---|---|
| χ2 | P | χ2 | P | |||||
| Age (year) | 1.162 | 0.281 | 0.273 | 0.601 | ||||
| <50 | 29 | 12(41.4) | 9(31.0) | |||||
| ≥50 | 66 | 19(28.8) | 17(25.8) | |||||
| Maximum tumor diameter (cm) | 0.490 | 0.484 | 0.535 | 0.465 | ||||
| <2 | 18 | 5(27.8) | 4(22.2) | |||||
| ≥2 | 77 | 26(33.8) | 22(28.6) | |||||
| Histological grade | 3.285 | 0.070 | 2.714 | 0.099 | ||||
| Low | 36 | 9(25.0) | 8(22.2) | |||||
| High | 59 | 22(37.3) | 18(30.5) | |||||
| Lymph node metastasis | 9.303 | 0.002 | 7.138 | 0.008 | ||||
| Negative | 50 | 10(20.0) | 9(18.0) | |||||
| Positive | 45 | 21(46.7) | 17(37.8) | |||||
| Nerve/vascular invasion | 2.531 | 0,112 | 1.173 | 0.279 | ||||
| Negative | 80 | 24(30.0) | 21(26.2) | |||||
| Positive | 15 | 7(46.7) | 5(33.3) | |||||
| Expression of AR | 3.845 | 0.050 | 3.763 | 0.052 | ||||
| Negative | 72 | 27(37.5) | 23(31.9) | |||||
| Positive | 23 | 4(17.4) | 3(13.0) | |||||
| Expression of SKP2 | 7.372 | 0.007 | 6.107 | 0.013 | ||||
| Negative | 51 | 11(21.6) | 9(17.6) | |||||
| Positive | 44 | 20(45.5) | 17(38.6) | |||||
| Expression of SOX10 | 21.072 | 0.000 | 15.777 | 0.000 | ||||
| Negative | 42 | 3(7.1) | 3(7.1) | |||||
| Positive | 53 | 28(52.8) | 23(43.4) | |||||
| Expression of PD-L1 | 0.610 | 0.435 | 0.238 | 0.626 | ||||
| Negative | 52 | 15(28.8) | 13(25.0) | |||||
| Positive | 43 | 16(37.2) | 13(30.2) | |||||
| Expression of TIL | 8.284 | 0.016 | 11.022 | 0.004 | ||||
| Low | 34 | 16(47.1) | 15(44.1) | |||||
| Moderate | 44 | 12(27.3) | 10(22.7) | |||||
| High | 17 | 3(17.6) | 1(5.9) | |||||
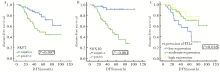
图2
SKP2(A)、SOX10(B)、TIL(C)在TNBC中的表达对DFS的影响

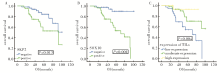
图3
SKP2(A)、SOX10(B)、TILs(C)在TNBC中表达对OS的影响
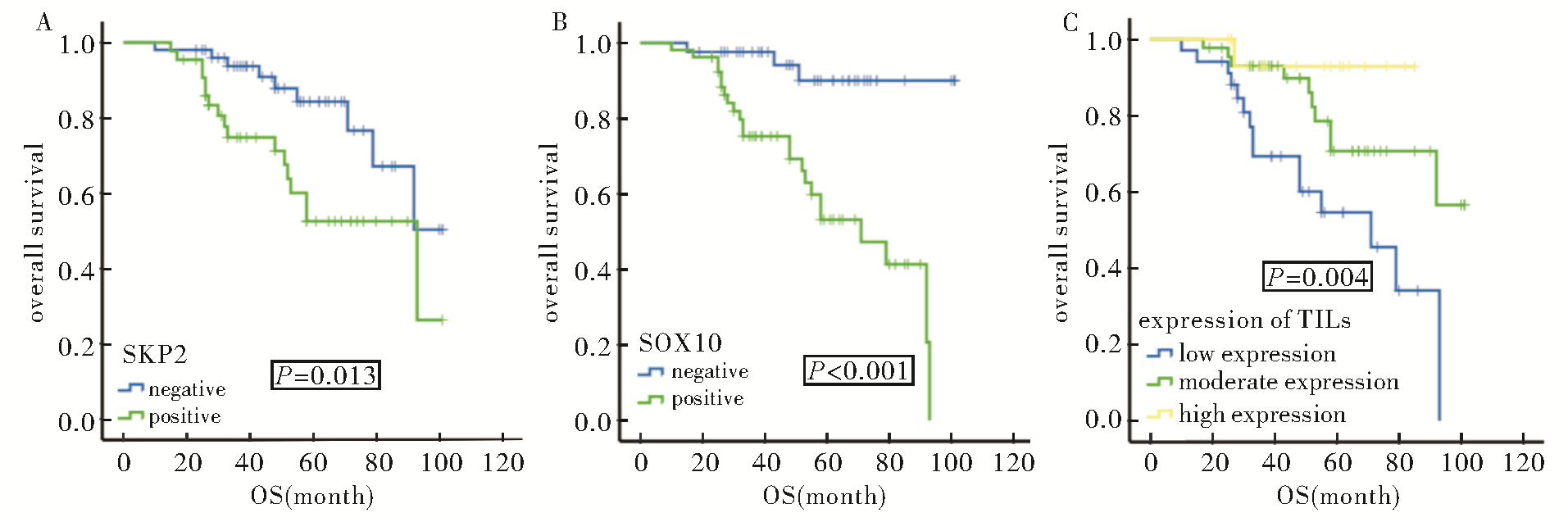

图4
生物指标联合分层的生存分析显示AR/SKP2(A)、AR/SOX10(B)、SOX10/TILs(C)、PD-L1/TILs(D)在TNBC表达对DFS的影响
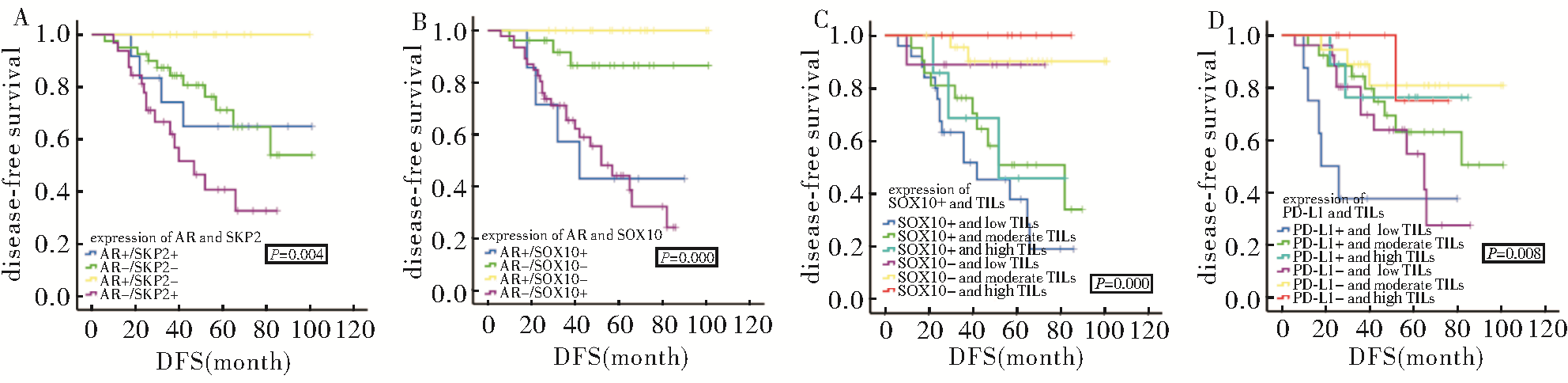
图5
生物指标联合分层的生存分析显示AR/SKP2(A)、AR/SOX10(B)、AR/TILs(C)、SOX10/TILs(D)、PD-L1/TILs(E)在TNBC表达对OS的影响
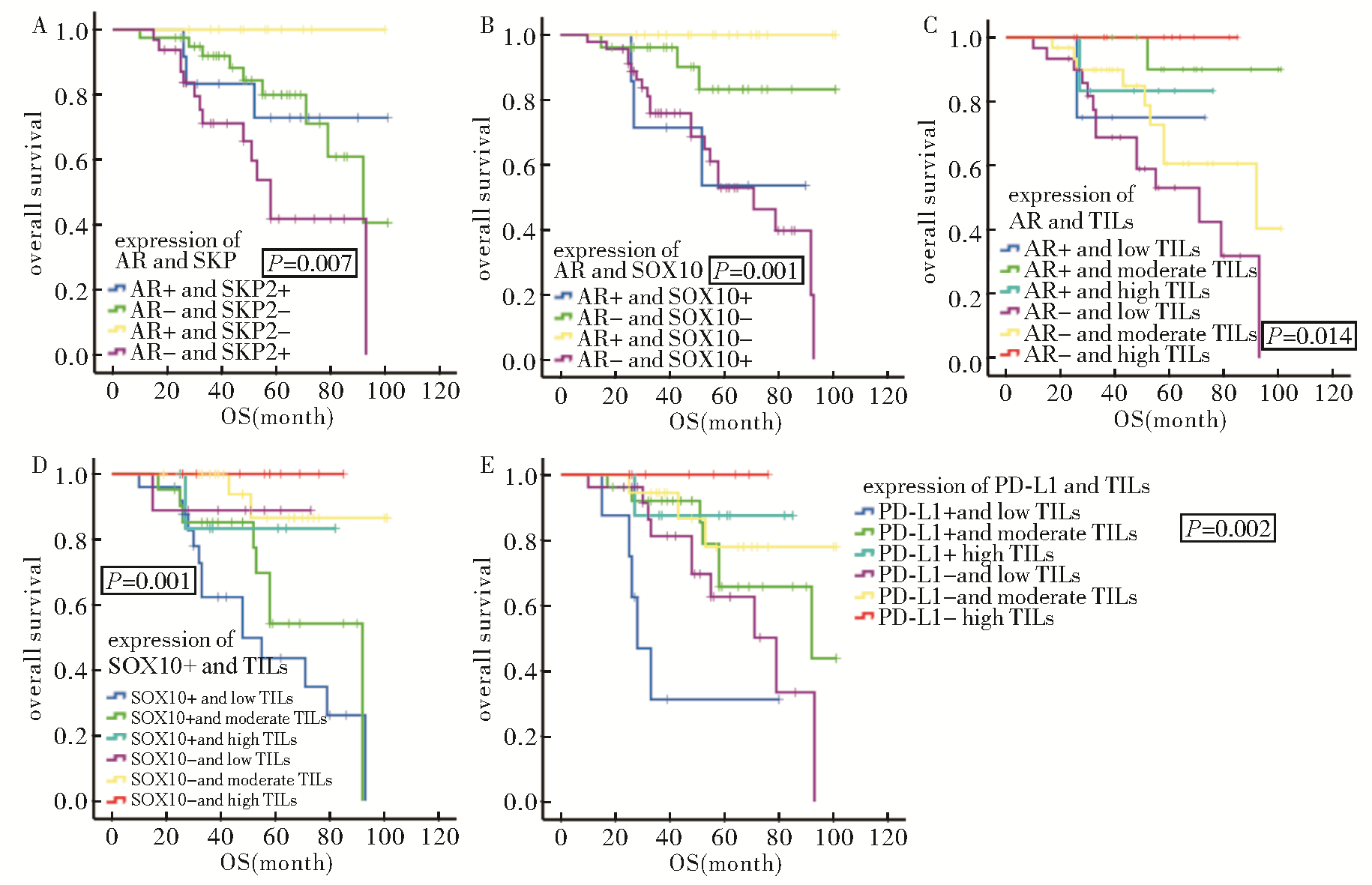
表4
TNBC各临床病理特征对DFS及OS影响的多因素分析
| Covariant | DFS | OS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Wald | P | HR | 95.0%CI of HR | Wald | P | HR | 95.0%CI of HR | ||
| Age | 3.277 | 0.070 | 0.474 | 0.212_1.064 | 1.555 | 0.212 | 0.569 | 0.234_1.381 | |
| Maximum tumor diameter | 0.338 | 0.561 | 1.098 | 0.801_1.504 | 0.032 | 0.858 | 0.968 | 0.676_1.386 | |
| Histological grade | 0.578 | 0.447 | 0.703 | 0.284_1.743 | 0.663 | 0.415 | 0.665 | 0.249_1.777 | |
| Lymph node metastasis | 4.758 | 0.029 | 2.718 | 1.107_6.676 | 4.336 | 0.037 | 2.896 | 1.065_7.876 | |
| Nerve/vascular invasion | 1.741 | 0.187 | 0.480 | 0.161_1.428 | 1.571 | 0.210 | 0.442 | 0.124_1.583 | |
| Expression of AR | 0.075 | 0.784 | 0.842 | 0.247_2.876 | 0.039 | 0.843 | 0.866 | 0.209_3.589 | |
| Expression of SKP2 | 8.334 | 0.004 | 4.143 | 1.578_10.875 | 6.910 | 0.009 | 3.758 | 1.400_10.084 | |
| Expression of SOX10 | 9.335 | 0.002 | 7.578 | 2.067_27.782 | 5.550 | 0.018 | 5.131 | 1.316_20.000 | |
| Expression of PD-L1 | 0.015 | 0.903 | 1.067 | 0.376_3.030 | 0.939 | 0.333 | 1.755 | 0.562_5.478 | |
| Expression of TILs | 2.015 | 0.156 | 0.601 | 0.298_1.214 | 4.625 | 0.032 | 0.375 | 0.154_0.917 | |
| [1] |
CHOUPANI E, MAHMOUDI GOMARI M, ZANGANEH S, et al. Newly developed targeted therapies against the androgen receptor in triple-negative breast cancer: a review[J]. Pharmacol Rev, 2023, 75(2):309-327.
doi: 10.1124/pharmrev.122.000665 pmid: 36781219 |
| [2] | NITĂ I, NITIPIR C, TOMAS A, et al. Correlation between androgen receptor expression and immunohistochemistry type as prognostic factors in a cohort of breast cancer patients: result from a single-center, cross sectional study[J]. Healthcare (Basel), 2021, 9(3):277. |
| [3] |
GOTO Y, THIKE A A, ONG C C H, et al. Characteristics, behaviour and role of biomarkers in metastatic triple-negative breast cancer[J]. J Clin Pathol, 2020, 73(3):147-153.
doi: 10.1136/jclinpath-2019-206078 pmid: 31563883 |
| [4] |
SANG M, MENG L, MA C, et al. Effect of AR antagonist combined with PARP1 inhibitor on sporadic triple-negative breast cancer bearing AR expression and methylation-mediated BRCA1 dysfunction[J]. Biomed Pharmacother, 2019, 111:169-177.
doi: S0753-3322(18)37264-0 pmid: 30580238 |
| [5] |
SRIDHAR N, GLISCH C, JAWA Z, et al. Androgen receptor expression in patients with triple negative breast cancer treated with neoadjuvant chemotherapy: a single institution study[J]. J Cancer, 2022, 13(8):2472-2476.
doi: 10.7150/jca.67536 pmid: 35711833 |
| [6] | 段帅, 地力木拉提·艾斯木吐拉, 王海燕, 等. 三阴性乳腺癌新辅助化疗病理完全缓解的影响因素[J]. 中国临床研究, 2024, 37(3):354-358. |
| DUAN S, DILIMULATI A, WANG H Y, et al. Influen-cing factors of pathological complete response in triple-negative breastcancer with neoadiuvant chemotherapy[J]. Chin J Clin Res, 2024, 37(3):354-358. | |
| [7] | DAI C, ELLISEN L W. Revisiting androgen receptor signaling in breast cancer[J]. Oncologist, 2023, 28(5):383-391. |
| [8] |
LI C, DU L, REN Y, et al. SKP2 promotes breast cancer tumorigenesis and radiation tolerance through PDCD4 ubiquitination[J]. J Exp Clin Cancer Res, 2019, 38(1):76.
doi: 10.1186/s13046-019-1069-3 pmid: 30760284 |
| [9] | WANG X, ZHANG T, ZHANG S, et al. Prognostic values of F-box members in breast cancer: an online database analysis and literature review[J]. Biosci Rep, 2019, 39(1):BSR20180949. |
| [10] |
SAUNUS J M, DE LUCA X M, NORTHWOOD K, et al. Epigenome erosion and SOX10 drive neural crest phenotypic mimicry in triple-negative breast cancer[J]. NPJ Breast Cancer, 2022, 8(1):57.
doi: 10.1038/s41523-022-00425-x pmid: 35501337 |
| [11] | ALI S, RATHORE Z, RAFIQUE Z, et al. Expression of SOX10 in triple-negative breast carcinoma in Pakistan[J]. Cureus, 2022, 14(8):e27938. |
| [12] |
JIN L, QIN C, QI X, et al. Clinicopathological significance of Sox10 expression in triple-negative breast carcinoma[J]. Transl Cancer Res, 2020, 9(9):5603-5613.
doi: 10.21037/tcr-20-2634 pmid: 35117924 |
| [13] | KRIEGSMANN K, FLECHTENMACHER C, HEIL J, et al. Immunohistological expression of SOX-10 in triple-negative breast cancer: a descriptive analysis of 113 samples[J]. Int J Mol Sci, 2020, 21(17):6407. |
| [14] | PARVATHAREDDY S K, SIRAJ A K, AHMED S O, et al. PD-L1 protein expression in middle eastern breast cancer predicts favorable outcome in triple-negative breast cancer[J]. Cells, 2021, 10(2):229. |
| [15] | CHOI S H, CHANG J S, KOO J S, et al. Differential prognostic impact of strong PD-L1 expression and 18F-FDG uptake in triple-negative breast cancer[J]. Am J Clin Oncol, 2018, 41(11):1049-1057. |
| [16] |
SUNAR V, T DOGAN H, SARICI F, et al. Association between androgen receptor status and prognosis in triple negative breast cancer[J]. J BUON, 2018, 23(5):1325-1330.
pmid: 30570854 |
| [17] |
ZHONG K, YANG F, HAN Q, et al. Skp2 expression has different clinicopathological and prognostic implications in lung adenocarcinoma and squamous cell carcinoma[J]. Oncol Lett, 2018, 16(3):2873-2880.
doi: 10.3892/ol.2018.9000 pmid: 30127874 |
| [18] | SHI Y, LI N, REN H, et al. Prognostic role of s-phase kinase-associated protein 2 in breast cancer: A meta-analysis[J]. Indian J Cancer, 2015, 52 Suppl 3:E153-E157. |
| [19] | FENG W, LIU S, ZHU R, et al. SOX10 induced Nestin expression regulates cancer stem cell properties of TNBC cells[J]. Biochem Biophys Res Commun, 2017, 485(2):522-528. |
| [20] | RAMMAL R, GOEL K, ELISHAEV E, et al. The utility of SOX10 immunohistochemical staining in breast patho-logy[J]. Am J Clin Pathol, 2022, 158(5):616-625. |
| [21] | 刘建兰, 陈黛诗, 成志强, 等. SOX10和GATA3在乳腺癌中的表达及意义[J]. 中华病理学杂志, 2022, 51(6):536-541. |
| LIU J L, CHEN D S, CHENG Z Q, et al. Expression of SOX10 and GATA3 in breast cancer and their significance[J]. Chin J Pathol, 2022, 51(6):536-541. | |
| [22] | LI Y, OPYRCHAL M, YAO S, et al. The role of programmed death ligand-1 and tumor-infiltrating lymphocytes in breast cancer overexpressing HER2 gene[J]. Breast Cancer Res Treat, 2018, 170(2):293-302. |
| [23] | MANGIA A, SAPONARO C, VAGHEGGINI A, et al. Should tumor infiltrating lymphocytes, androgen receptor, and FOXA1 expression predict the clinical outcome in triple negative breast cancer patients?[J]. Cancers (Basel), 2019, 11(9):1393. |
| [24] | TOMIOKA N, HATANAKA K C, OKUYAMA D, et al. Programmed death ligand 1-positive immune cells in primary tumor or metastatic axillary lymph nodes can predict prognosis of triple-negative breast cancer even when present at <1% in the tumor region[J]. Breast Cancer, 2023, 30(3):497-505. |
| [25] | YAZAKI S, SHIMOI T, YOSHIDA M, et al. Integrative prognostic analysis of tumor-infiltrating lymphocytes, CD8, CD20, programmed cell death-ligand 1, and tertiary lymphoid structures in patients with early-stage triple-negative breast cancer who did not receive adjuvant chemotherapy[J]. Breast Cancer Res Treat, 2023, 197(2):287-297. |
| [26] | MORI H, KUBO M, YAMAGUCHI R, et al. The combination of PD-L1 expression and decreased tumor-infiltra-ting lymphocytes is associated with a poor prognosis in triple-negative breast cancer[J]. Oncotarget, 2017, 8(9):15584-15592. |
| [27] | 袁杰, 张华, 王群, 等. 影响乳腺癌新辅助化疗后前哨淋巴结活检准确率的因素[J]. 中国临床研究, 2023, 36(11):1683-1687. |
| YUAN J, ZHANG H, WANG Q, et al. Factors influen-cing the accuracy of sentinel lymph node biopsy after neoadjuvant chemotherapy in breast cancer[J]. Chin J Clin Res, 2023, 36(11):1683-1687. |
| [1] | 欧丹, 蔡钢, 陈佳艺. RAD51AP1基因表达在三阴性乳腺癌脑转移中的生物信息分析[J]. 诊断学理论与实践, 2024, 23(02): 146-154. |
| [2] | 沈琳辉, 崔斌, 赵咏桔, 颜美珠, 林云, 巩云霞, 吴方,. 老年男性雄激素受体基因CAG重复序列长度多态性与代谢综合征的关系[J]. 诊断学理论与实践, 2007, 6(05): 412-416. |
| [3] | 于琦, 牛昀, 方志沂,. X染色体的克隆性分析及其在乳腺肿瘤研究中的应用[J]. 诊断学理论与实践, 2005, 4(06): 510-512. |
| [4] | 路光中,胡宏慧,张雪梅,陈嘉薇,杨兆瑞. 脑膜瘤中三种性激素受体的表达及其意义[J]. 诊断学理论与实践, 2005, 4(04): 313-316. |
| [5] | 吕艳,牛昀,丁秀敏,肖绪祺,于泳. Skp2在导管上皮不典型增生和乳腺癌表达及意义的初步研究[J]. 诊断学理论与实践, 2005, 4(03): 202-205. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||