诊断学理论与实践 ›› 2023, Vol. 22 ›› Issue (05): 480-485.doi: 10.16150/j.1671-2870.2023.05.010
侯怡茹1, 王敏2( ), 王春花2, 陈俞洁2
), 王春花2, 陈俞洁2
收稿日期:2023-09-04
出版日期:2023-10-25
发布日期:2024-03-15
通讯作者:
王敏 E-mail:
HOU Yiru1, WANG Min2(), WANG Chunhua2, CHEN Yujie2
Received:2023-09-04
Online:2023-10-25
Published:2024-03-15
摘要:
本文报告1例罕见的亚临床原发性醛固酮增多症(subclinical primary aldosteronism,SPA)合并亚临床库欣综合征(subclinical Cushing syndrome,SCS)患者。该患者为41岁的女性,因肾上腺偶发瘤(adrenal incidentaloma,AI)入院。患者无高血压、低血钾、糖代谢异常等典型的原发性醛固酮增多症(primary aldosteronism,PA)或库欣综合征(Cushing syndrome,CS)的临床表现,实验室检查示醛固酮肾素比值(aldosterone to renin ratio,ARR)>3.7,促肾上腺皮质激素(adrenocorticotropic hormone,ACTH)<1.6 pg/mL,最终依据术后病理学检查结果,患者被诊断为肾上腺皮质腺瘤。该病例中存在2种亚临床疾病共存的诊断,这种临床类型在目前的指南和报道中并未得到充分认识,值得关注并进行更详细的讨论。
中图分类号:
侯怡茹, 王敏, 王春花, 陈俞洁. 亚临床原发性醛固酮增多症合并亚临床库欣综合征1例并文献复习[J]. 诊断学理论与实践, 2023, 22(05): 480-485.
HOU Yiru, WANG Min, WANG Chunhua, CHEN Yujie. A case report of subclinical primary aldosterone complicating with subclinical Cushing syndrome and literature review[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(05): 480-485.
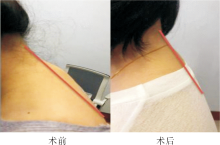
图1
患者颈背部软组织术前、术后对比
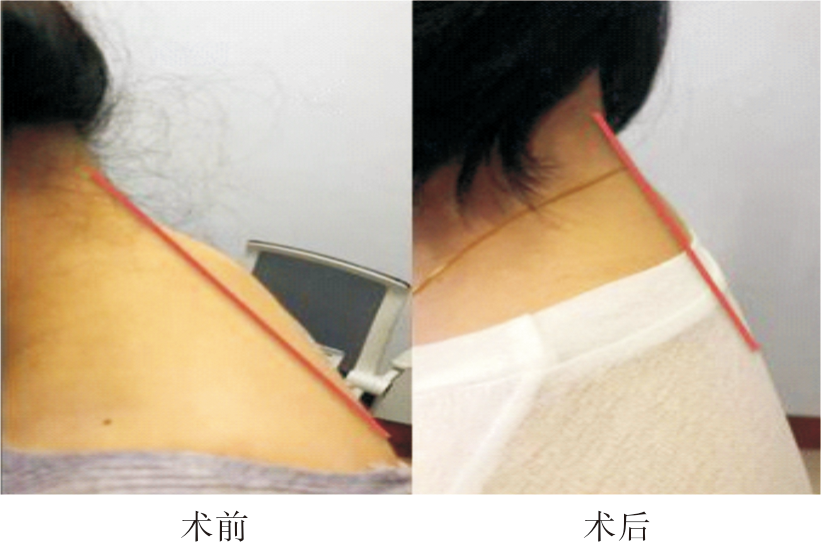
表1
肾上腺皮质激素及肾上腺髓质激素相关指标
| 项目 | 入院第1天 | 入院第3天 | 术后4周 |
|---|---|---|---|
| 血浆醛固酮浓度(ng/dL) | 4.01 | 7.65 | 11.4 |
| 血浆肾素活性(μIU/mL) | <0.5 | 0.5 | 20.0 |
| 醛固酮肾素比值 | 15.3 | 0.57 | 无 |
| 去甲肾上腺素(pg/mL) | 23.4 | 无 | 无 |
| 肾上腺素(pg/mL) | 10.6 | 无 | 无 |
表2
手术前、后24 h动态血压对比
| 时点 | 24 h平均(mmHg) | 白天清醒时段(mmHg) | 夜间睡眠时段(mmHg) | 起床后清醒时段(mmHg) | 昼夜节律(%) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 收缩压 | 舒张压 | 收缩压 | 舒张压 | 收缩压 | 舒张压 | 收缩压 | 舒张压 | 收缩压 | 舒张压 | |||||
| 术前 | 122 | 80 | 125 | 83 | 122 | 78 | 125 | 83 | <0.1 | 2.5 | ||||
| 术后 | 113 | 77 | 118 | 82 | 103 | 66 | 110 | 80 | 12.7 | 19.5 | ||||
表3
皮质醇节律及小剂量地塞米松抑制试验
| 指标 | 入院第1天 | 入院第2天 | 入院第3天 | 小剂量地塞米松抑制试验后 | 术后第1天 | 术后第4周 | ||
|---|---|---|---|---|---|---|---|---|
| 8 AM | 4 PM | 12 PM | 无 | 无 | 8 AM | 8 AM | 8 AM | |
| 血清皮质醇(μg/dL) | 4.82 | 5.80 | 3.24 | 无 | 无 | 1.14 | 15.13 | 5.83 |
| 促肾上腺皮质激素(pg/mL) | <1.6 | 1.69 | 无 | 无 | 无 | 无 | 无 | 15.11 |
| 24小时尿游离皮质醇(μg/24 h) | 无 | 无 | 无 | 194.01 | 175.78 | 25.41 | 无 | 无 |

图2
肾上腺CT平扫加增强 注:红色箭头所指为肾上腺结节
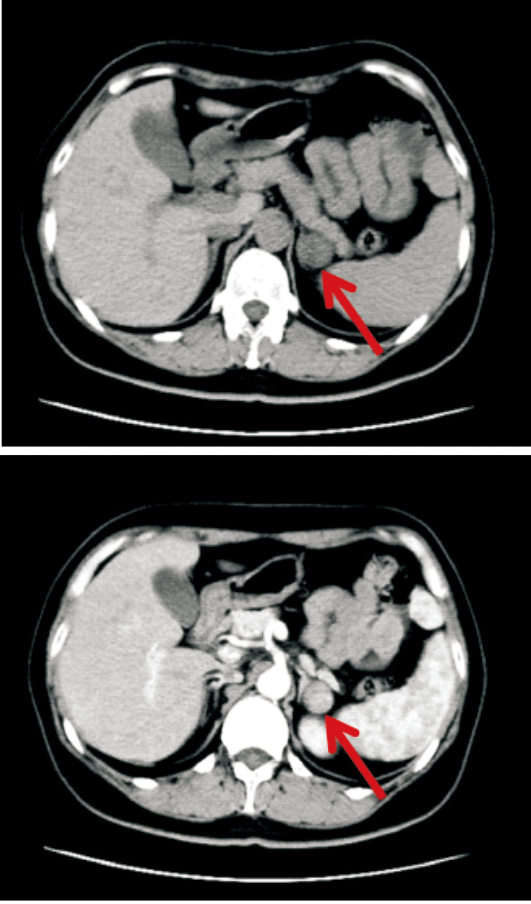
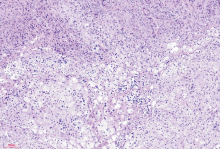
图3
肾上腺肿物病理(HE,×40) 注:此病例病理形态为典型的肾上腺皮质腺瘤(各种临床功能类型的皮质腺瘤在显微镜下没有明显的组织学差异)。显微镜下可见,肿瘤主要由透明细胞和嗜酸性的致密细胞组成,透明细胞类似正常肾上腺皮质的束状带细胞,致密细胞类似正常肾上腺皮质的网状带细胞,还有一些体积较小的细胞质空泡化的类似正常肾上腺皮质的球状带细胞。肿瘤细胞排列以巢状、条索状、小梁状为主。
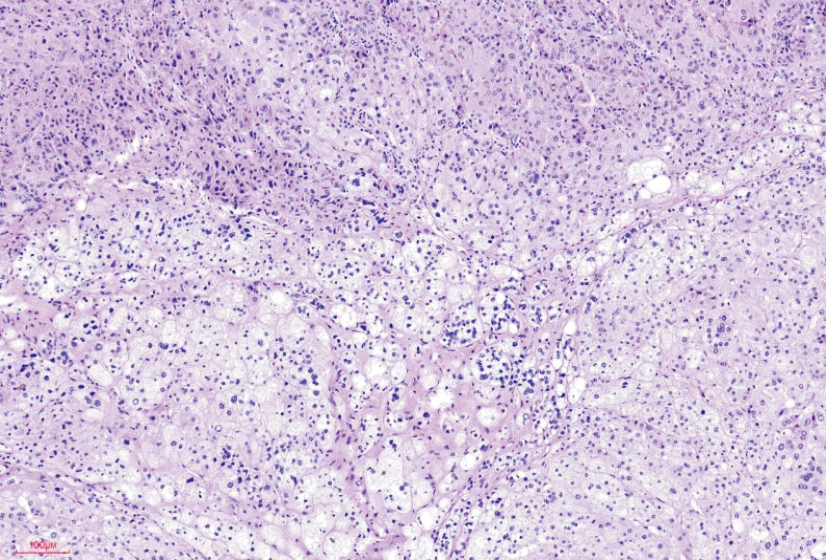
表4
Kitajima报道[8]病例与本病例的对比表
| 项目 SPA合并SCS | Kitajima 报道[ | 本病例 | |
|---|---|---|---|
| 临床表现 | 49岁女性 | 41岁女性 | |
| 因“肾上腺偶发瘤”入院 | 因“肾上腺偶发瘤”入院 | ||
| 无满月脸 | 无满月脸,无多血质面容 | ||
| 无中心型肥胖 | 项背部正中软组织增厚 | ||
| 无肢体无力 | 腹部、臀部未见紫纹 | ||
| 既往史 | 无 | 无 | |
| 实验室检查 | |||
| 血钾(mmol/L) | 4.0 | 3.7 | |
| 8 AM皮质醇(μg/dL) | 11.7 | 4.82 | |
| 4 PM皮质醇(μg/dL) | 无 | 5.80 | |
| 11 PM皮质醇(μg/dL) | 3.3 | 无 | |
| 12 PM皮质醇(μg/dL) | 无 | 3.24 | |
| 1 mg地塞米松抑制试验后皮质醇(μg/dL) | 1.8 | 无 | |
| 小剂量地塞米松抑制试验后皮质醇(μg/dL) | 无 | 1.14 | |
| 促肾上腺皮质激素(pg/mL) | <2.0 | <1.6 | |
| 血浆醛固酮浓度 | 110 pg/mL | 7.65 ng/dL | |
| 血浆肾素活性 | 0.1 ng/(mL·h) | 0.5 μIU/mL | |
| 醛固酮肾素比值 | >200 | 15.3 | |
| 卡托普利试验 | 阳性 | 无 | |
| 盐水负荷试验 | 阴性 | 无 | |
| CT | 双侧肾上腺结节(左侧结节18 mm,右侧结节13 mm) | 左侧肾上腺结节(2.5 cm×2.4 cm) | |
| 病理 | 无 | 手术标本切面呈金黄色,病理诊断为左侧肾上腺肿物皮质腺瘤 | |
| 治疗 | 无 | 手术切除 | |
| 随访 | |||
| 血钾、血压 | 恢复正常 | 恢复正常 | |
| 血浆醛固酮浓度、皮质醇、促肾上腺皮质激素 | 恢复正常 | 恢复正常 | |
| 血浆肾素活性 | 受抑制 | 恢复正常 | |
| 醛固酮肾素比值 | >200 | 恢复正常 | |
| [1] |
ITO Y, TAKEDA R, TAKEDA Y. Subclinical primary aldosteronism[J]. Best Pract Res Clin Endocrinol Metab, 2012, 26(4):485-495.
doi: 10.1016/j.beem.2011.11.006 pmid: 22863390 |
| [2] | 宋颖, 何文雯, 冯正平, 等. 血压正常的原发性醛固酮增多症临诊应对[J]. 中华内分泌外科杂志, 2023, 17(3):376-377. |
| SONG Y, HE W W, FENG Z P, et al. Approach to a normotensive patient with primary aldosteronism[J]. Chin J Endoc Surg, 2023, 17(3):376-377. | |
| [3] | 白求恩精神研究会内分泌和糖尿病学分会《2022年亚临床库欣综合征专家指导建议》编写组. 2022年亚临床库欣综合征专家指导建议[J]. 国际内分泌代谢杂志, 2023, 43(1):69-76. |
| Expert group for "Expert consensus on subclinical Cus-hing′s syndrome in China(2022)". Expert consensus on subclinical Cushing′s syndrome in China (2022)[J]. Int J Endocrinol Metab, 2023, 43(1):69-76. | |
| [4] |
FAVERO V, CREMASCHI A, PARAZZOLI C, et al. Pathophysiology of mild hypercortisolism: from the bench to the bedside[J]. Int J Mol Sci, 2022, 23(2):673.
doi: 10.3390/ijms23020673 URL |
| [5] |
FAVERO V, CREMASCHI A, FALCHETTI A, et al. Management and medical therapy of mild hypercortisolism[J]. Int J Mol Sci, 2021, 22(21):11521.
doi: 10.3390/ijms222111521 URL |
| [6] |
CHIODINI I, ALBANI A, AMBROGIO A G, et al. Six controversial issues on subclinical Cushing's syndrome[J]. Endocrine, 2017, 56(2):262-266.
doi: 10.1007/s12020-016-1017-3 pmid: 27406391 |
| [7] | 王冬, 王若秋, 朱兴艳, 等. 肾上腺醛固酮-皮质醇共分泌瘤2例报道并文献复习[J]. 国际内分泌代谢杂志, 2023, 43(5):418-421. |
| WANG D, WANG R Q, ZHU X Y, et al. Adrenal aldosterone and cortisol co-producing adenoma: Two cases report and literature review[J]. Int J Endocrinol Metab, 2023, 43(5):418-421. | |
| [8] | KITAJIMA N, SEKI T, YASUDA A, et al. A rare case of subclinical primary aldosteronism and subclinical Cus-hing's syndrome without cardiovascular complications[J]. Tokai J Exp Clin Med, 2016, 41(1):35-41. |
| [9] |
ICHIJO T, UESHIBA H, NAWATA H, et al. A nationwide survey of adrenal incidentalomas in Japan: the first report of clinical and epidemiological features[J]. Endocr J, 2020, 67(2):141-152.
doi: 10.1507/endocrj.EJ18-0486 pmid: 31694993 |
| [10] | PAN L H, CHEN Y Y, PAN C T, et al. Follow-up care and assessment of comorbidities and complications in patients with primary aldosteronism: The clinical practice guideline of the Taiwan Society of aldosteronism[J/OL]. J Formos Med Assoc, 2023-08-22. https://linkinghub.elsevier.com/retrieve/pii/S0929-6646(23)00324-8. |
| [11] | 中华医学会内分泌学分会. 原发性醛固酮增多症诊断治疗的专家共识(2020版)[J]. 中华内分泌代谢杂志, 2020, 36(9):727-736. |
| Chinese Society of Endocrinology. Expert consensus on the diagnosis and treatment of primary aldosteronism (2020)[J]. Chin J Endocrinol Metab, 2020, 36(9):727-736. | |
| [12] | 中国内分泌代谢病专科联盟. 原发性醛固酮增多症诊治行业标准[J]. 中华内分泌代谢杂志, 2022, 38(7):555-557. |
| China Endocrinology and Metabolism Specialist Alliance. Standard for the diagnosis and treatment of primary aldosteronism[J]. Chin J Endocrinol Metab, 2022, 38(7):555-557. | |
| [13] |
KMIEĆ P, SWORCZAK K. Autonomous aldosterone secretion as a subclinical form of primary aldosteronism: pathogenesis and clinical significance[J]. Exp Clin Endocrinol Diabetes. 2022 Jan; 130(1):7-16.
doi: 10.1055/a-1556-7784 URL |
| [14] |
FASSNACHT M, ARLT W, BANCOS I, et al. Management of adrenal incidentalomas: European Society of Endocrinology Clinical Practice Guideline in collaboration with the European Network for the study of adrenal tumors[J]. Eur J Endocrinol, 2016, 175(2):G1-G34.
doi: 10.1530/EJE-16-0467 URL |
| [15] |
YANASE T, OKI Y, KATABAMI T, et al. New diagnostic criteria of adrenal subclinical Cushing's syndrome: opinion from the Japan Endocrine Society[J]. Endocr J, 2018, 65(4):383-393.
doi: 10.1507/endocrj.EJ17-0456 pmid: 29576599 |
| [16] |
YOUNG W F. Primary aldosteronism: renaissance of a syndrome[J]. Clin Endocrinol (Oxf), 2007, 66(5):607-618.
doi: 10.1111/cen.2007.66.issue-5 URL |
| [17] |
STOWASSER M, GORDON R D. Primary aldosteronism-careful investigation is essential and rewarding[J]. Mol Cell Endocrinol, 2004, 217(1-2):33-39.
doi: 10.1016/j.mce.2003.10.006 URL |
| [18] |
MOSSO L, CARVAJAL C, GONZÁLEZ A, et al. Primary aldosteronism and hypertensive disease[J]. Hypertension, 2003, 42(2):161-165.
doi: 10.1161/01.HYP.0000079505.25750.11 pmid: 12796282 |
| [19] |
BROWN J M, ROBINSON-COHEN C, LUQUE-FERNANDEZ M A, et al. The spectrum of subclinical primary aldosteronism and incident hypertension: a cohort study[J]. Ann Intern Med, 2017, 167(9):630-641.
doi: 10.7326/M17-0882 pmid: 29052707 |
| [20] |
KMIEĆ P, ZALEWSKA E, KUNICKA K, et al. Autonomous aldosterone secretion in patients with adrenal incidentaloma[J]. Biomedicines, 2022, 10(12):3075.
doi: 10.3390/biomedicines10123075 URL |
| [21] | 李乐乐, 韩白玉, 窦京涛, 等. 午夜1 mg地塞米松抑制试验对肾上腺意外瘤中亚临床库欣综合征的诊断价值[J]. 中华医学杂志, 2015, 95(48):3912-3916. |
| LI L L, HAN B Y, DOU J T, et al. Evaluation of the 1 mg overnight dexamethasone suppression test in the diagnosis of the subclinical Cushing's syndrome in patients with adrenal incidentaloma[J]. Natl Med J China, 2015, 95(48):3912-3916. | |
| [22] |
OJEDA N B, GRIGORE D, ROBERTSON E B, et al. Estrogen protects against increased blood pressure in postpubertal female growth restricted offspring[J]. Hypertension, 2007, 50(4):679-685.
doi: 10.1161/HYPERTENSIONAHA.107.091785 pmid: 17724277 |
| [1] | 胡哲, 陈歆, 罗芳秀, 初少莉, 王继光. 肾上腺醛固酮和皮质醇共分泌瘤一例报告[J]. 诊断学理论与实践, 2020, 19(05): 525-527. |
| [2] | Anoj Adhikari, 陈克敏,. 肾上腺偶发瘤的影像学诊断与治疗进展[J]. 诊断学理论与实践, 2015, 14(05): 473-478. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||