Journal of Diagnostics Concepts & Practice ›› 2023, Vol. 22 ›› Issue (04): 348-361.doi: 10.16150/j.1671-2870.2023.04.004
• Academic trend at home and abroad • Previous Articles Next Articles
SHI Zhongwei( )
)
Received:2023-06-24
Online:2023-08-25
Published:2023-12-18
CLC Number:
SHI Zhongwei. The diagnostic threshold for hypertension should not be lowered down to 130/80 mmhg: an academic perspective[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(04): 348-361.

Figure 1
A receiver operating characteristic curve for diagnosing hypertension[31]

Figure 2
Randomized clinical trials comparing intensive versus conventional blood pressure lowering treatment in patients with diabetes[33]
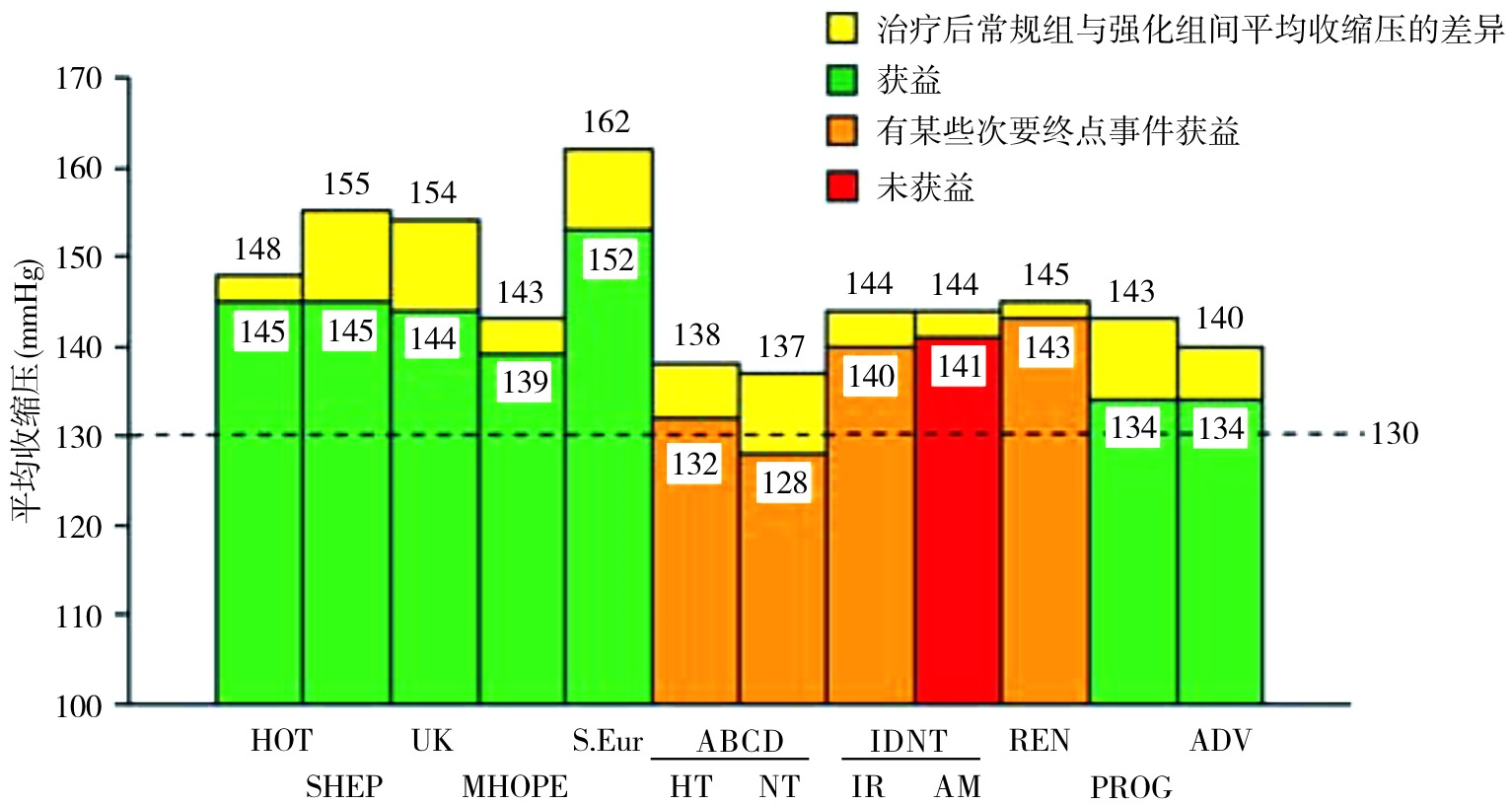
Table 1
Comparison of Attended versus Unattended Office SBP Measurement: Mean (±SD) BP Values[80???-84]
| 作者及国家 | 年份 | 例数 | 诊室收缩压平均值*(mmHg) | ||
|---|---|---|---|---|---|
| 有人诊室测压 | 无人诊室测压 | 血压差 | |||
| Filipovsky,捷克 | 2016 | 353 | 146.9±20.8 | 131.2±21.8 | 15.7±13.8 |
| Agarwal,美国 | 2017 | 275 | 134.5±19.5 | 121.7±17.9 | 12.7±12.0 |
| Bauer,德国 | 2018 | 51 | 135.7±21.5 | 134.2±19.2 | 1.5 |
| Paini,意大利 | 2019 | 329 | 129.8±15.5 | 138.4±16.7 | 8.6±7.7 |
| Cheng,美国 | 2019 | 202 | 145.6±23.5 | 135.3±23.5 | 10.3 |
Figure 3
Home morning SBP in relation to weather temperature in the two treatment groups throughout the trial in the STEP trial[95]
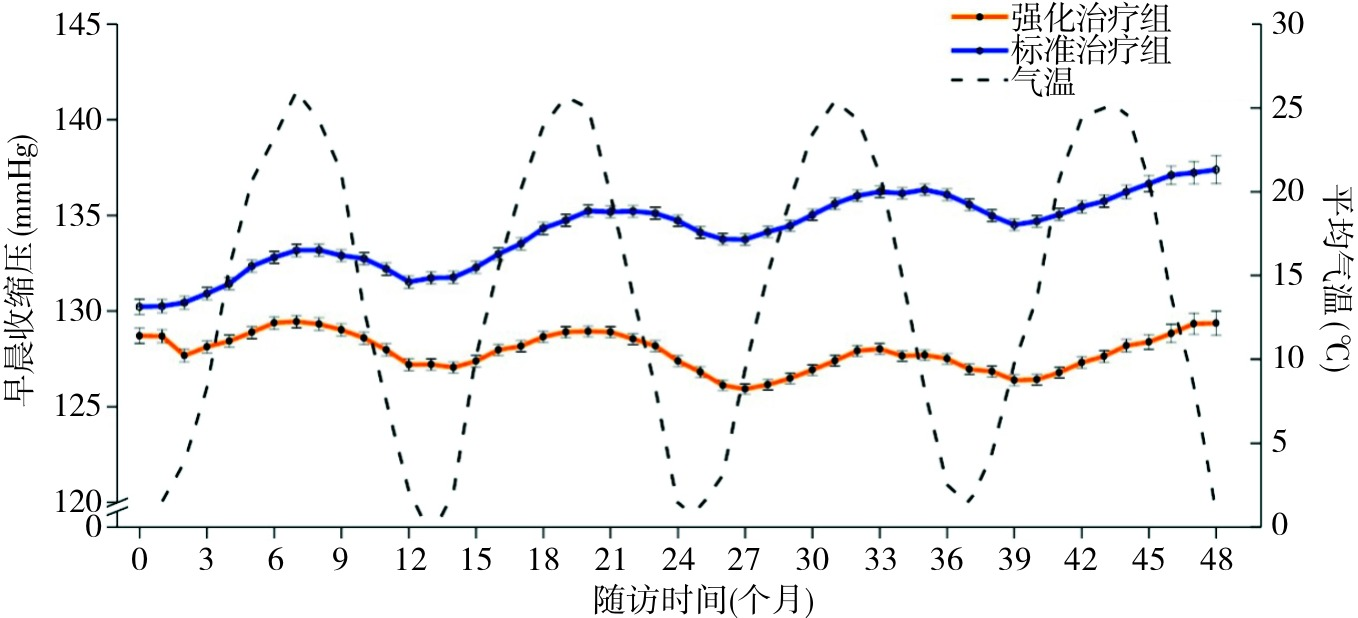

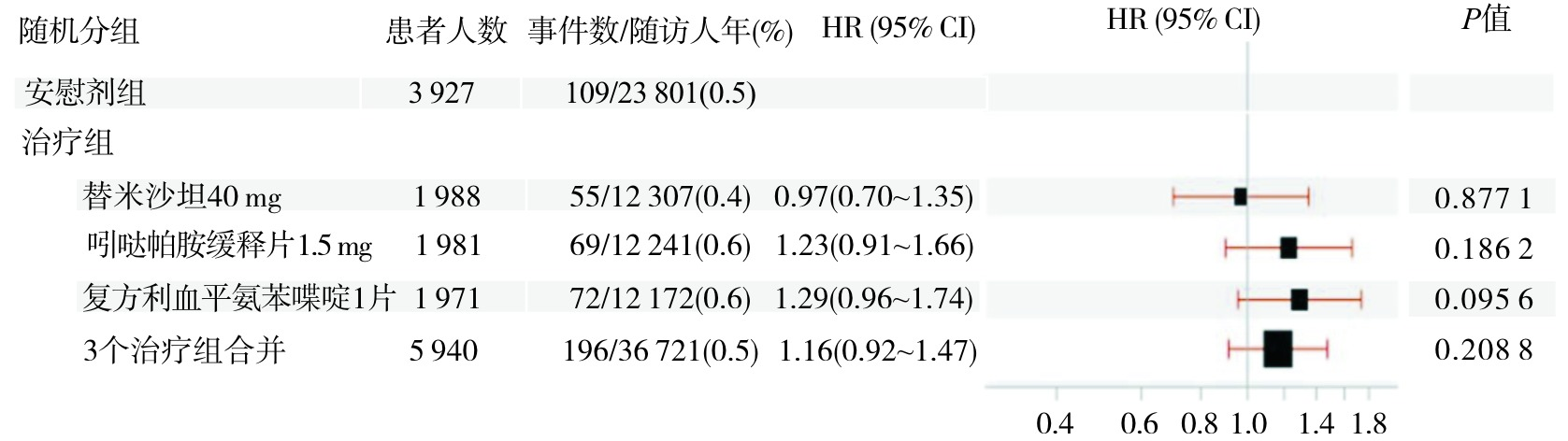
Figure 4
The incidence of primary outcome events in CHINOM trial[107]
| [1] | 王薇, 赵冬, 刘静, 等. 中国35-64岁人群血压水平与10年心血管病发病危险的前瞻性研究[J]. 中华内科杂志, 2004, 43(10):730-734. |
| WANG W, ZHAO D, LIU J, et al. A prospective study of relationship between blood pressure and 10-year cardiovascular risk in a Chinese cohort aged 35-64 years[J]. Zhonghua Nei Ke Za Zhi, 2004, 43(10):730-734. | |
| [2] | 曾新颖, 刘世炜, 王黎君, 等. 2013年中国人群血压升高对死亡和期望寿命的影响[J]. 中华流行病学杂志, 2017, 38(8):1011-1016. |
| ZENG X Y, LIU S W, WANG L J, et al. Mortality and life expectancy that attributable to high blood pressure in Chinese people in 2013[J]. Zhonghua Liu Xing Bing Xue Za Zhi, 2017, 38(8):1011-1016. | |
| [3] |
CAO X, ZHAO Z, KANG Y, et al. The burden of cardiovascular disease attributable to high systolic blood pressure across China, 2005-18: a population-based study[J]. Lancet Public Health, 2022, 7(12):e1027-e1040.
doi: 10.1016/S2468-2667(22)00232-8 pmid: 36462514 |
| [4] | 中国高血压防治指南修订委员会, 高血压联盟中国, 中华医学会心血管病学分会, 等. 中国高血压防治指南(2018年修订版)[J]. 中国心血管杂志, 2019, 24(1):24-56. |
| Writing Group of 2018 Chinese Guidelines for the Management of Hypertension, Chinese Hypertension League, Chinese Society of Cardiology, et al. 2018 Chinese guidelines for the management of hypertensionWriting Group of 2018[J]. Chin J Cardiovasc Med, 2019, 24(1):24-56. | |
| [5] | 罗兰. 最新发布! 中国高血压诊断标准下调![EB/OL]. 光明网.(2022-11-14) [2023-4-8]. https://m.gmw.cn/baijia/2022-11/14/1303194218.html. |
| LUO L. Latest Release! The diagnostic criteria for hypertension in China have been lowered![EB/OL]. Guangming Net.(2022-11-14) [2023-4-8]. https://m.gmw.cn/baijia/2022-11/14/1303194218.html. | |
| [6] | 钱童心. 中国高血压联盟主席: 高血压诊断标准下调不适合我国国情[N/OL]. 第一财经日报. 第A04版. (2022-11-16). https://www.yicai.com/news/101595160.html. |
| QIAN T X. Chairman of the Chinese Hypertension Alliance: Downregulation of hypertension diagnostic criteria is not suitable for China's national conditions[N/OL]. China Business News. A04. (2022-11-16). https://www.yicai.com/news/101595160.html. | |
| [7] |
CUNNINGHAM R L. MECHANISM AND CLINICAL ASPECTS OF CHRONIC ARTERIAL HYPERTENSION[J]. Cal State J Med, 1912, 10(7):303-305.
pmid: 18735632 |
| [8] |
LÜSCHER T F. What is a normal blood pressure?[J]. Eur Heart J, 2018, 39(24):2233-2240.
doi: 10.1093/eurheartj/ehy330 pmid: 29893817 |
| [9] |
KOTCHEN T A. Historical trends and milestones in hypertension research: a model of the process of translational research[J]. Hypertension, 2011, 58(4):522-538.
doi: 10.1161/HYPERTENSIONAHA.111.177766 pmid: 21859967 |
| [10] |
MOSER M, ROCCELLA E J. The treatment of hypertension: a remarkable success story[J]. J Clin Hypertens (Greenwich), 2013, 15(2):88-91.
doi: 10.1111/jch.12033 pmid: 23339725 |
| [11] |
Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. Report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. A cooperative study[J]. JAMA, 1977, 237(3):255-261.
doi: 10.1001/jama.1977.03270300059008 URL |
| [12] |
The Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. The 1980 report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure[J]. Arch Intern Med, 1980, 140(10):1280-1285.
pmid: 6775608 |
| [13] |
The Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. The 1984 report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure[J]. Arch Intern Med, 1984, 144(5):1045-1057.
pmid: 6143542 |
| [14] |
1988 Joint National Committee. The 1988 report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure[J]. Arch Intern Med, 1988, 148(5):1023-1038.
pmid: 3365073 |
| [15] |
The Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. The fifth report of the Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure JNC V[J]. Arch Intern Med, 1993, 153(2):154-183.
doi: 10.1001/archinte.1993.00410020010002 URL |
| [16] |
The Joint National Committee on Detection, Evaluation, and Treatment of High Blood Pressure. The sixth report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure[J]. Arch Intern Med, 1997, 157(21):2413-2446.
doi: 10.1001/archinte.157.21.2413 pmid: 9385294 |
| [17] |
CHOBANIAN A V, BAKRIS G L, BLACK H R, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: the JNC 7 report[J]. JAMA, 2003, 289(19):2560-2572.
doi: 10.1001/jama.289.19.2560 URL |
| [18] | BÜHLER F R, DOYLE A E, EPSTEIN F H, et al. Guidelines for the treatment of mild hypertension: memorandum from a WHO/ISH meeting[J]. Bull World Health Organ, 1983, 61(1):53-56. |
| [19] |
ZANCHETTI A, CHALMERS J P, ARAKAWA K, et al. The 1993 guidelines for the management of mild hypertension: memorandum from a WHO/ISH meeting[J]. Blood Press, 1993, 2(2):86-100.
doi: 10.3109/08037059309077535 URL |
| [20] | 刘力生, 龚兰生. 中国高血压防治指南(试行本)[J]. 中国医药导刊, 2000, 2(1):3-25. |
| LIU L S, GONG L S. Chinese Guidelines for the Prevention and Treatment of Hypertension (Trial Version)[J]. Chin J Med Guide, 2000, 2(1):3-25. | |
| [21] |
European Society of Hypertension-European Society of Cardiology Guidelines Committee. 2003 European Society of Hypertension-European Society of Cardiology guidelines for the management of arterial hypertension[J]. J Hypertens, 2003, 21(6):1011-1053.
doi: 10.1097/00004872-200306000-00001 pmid: 12777938 |
| [22] |
WILLIAMS B, MANCIA G, SPIERING W, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension[J]. Eur Heart J, 2018, 39(33):3021-3104.
doi: 10.1093/eurheartj/ehy339 pmid: 30165516 |
| [23] |
WILLIAMS B, POULTER N R, BROWN M J, et al. Guidelines for management of hypertension: report of the fourth working party of the British Hypertension Society, 2004-BHS IV[J]. J Hum Hypertens, 2004, 18(3):139-185.
doi: 10.1038/sj.jhh.1001683 pmid: 14973512 |
| [24] | National Institute for Health and Care Excellence (NICE). Hypertension in adults: diagnosis and management[EB/OL]. NICE guideline (NG 136).(2022-3-18) [2023-7-11]. https://www.nice.org.uk/guidance/ng136. |
| [25] |
EVANS J G, ROSE G. Hypertension[J]. Br Med Bull, 1971, 27(1):37-42.
doi: 10.1093/oxfordjournals.bmb.a070812 URL |
| [26] |
LEWINGTON S, CLARKE R, QIZILBASH N, et al. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies[J]. Lancet, 2002, 360(9349):1903-1913.
doi: 10.1016/s0140-6736(02)11911-8 pmid: 12493255 |
| [27] |
LIU L, ZHANG Y, LIU G, et al. The Felodipine Event Reduction (FEVER) Study: a randomized long-term placebo-controlled trial in Chinese hypertensive patients[J]. J Hypertens, 2005, 23(12):2157-2172.
doi: 10.1097/01.hjh.0000194120.42722.ac pmid: 16269957 |
| [28] |
THOMOPOULOS C, PARATI G, ZANCHETTI A. Effects at different baseline and achieved blood pressure levels--overview and meta-analyses of randomized trials[J]. J Hypertens, 2014, 32(12):2296-2304.
doi: 10.1097/HJH.0000000000000379 URL |
| [29] |
BRUNSTRÖM M, CARLBERG B. Association of Blood Pressure Lowering With Mortality and Cardiovascular Disease Across Blood Pressure Levels: A Systematic Review and Meta-analysis[J]. JAMA Intern Med, 2018, 178(1):28-36.
doi: 10.1001/jamainternmed.2017.6015 pmid: 29131895 |
| [30] | National Institute for Health and Care Excellence (NICE). Hypertension in adults: diagnosis and management[C/OL]. Evidence review for initiating treatment. NICE guideline (NG 136).(2019-8) [2023-7-11]. https://www.nice.org.uk/guidance/ng136/evidence/c-initiating-treatment-pdf-6896748208. |
| [31] |
PATER C. The Blood Pressure "Uncertainty Range"-a pragmatic approach to overcome current diagnostic uncertainties (II)[J]. Curr Control Trials Cardiovasc Med, 2005, 6(1):5.
doi: 10.1186/1468-6708-6-5 URL |
| [32] |
ZANCHETTI A, GRASSI G, MANCIA G. When should antihypertensive drug treatment be initiated and to what levels should systolic blood pressure be lowered? A critical reappraisal[J]. J Hypertens, 2009, 27(5):923-934.
doi: 10.1097/HJH.0b013e32832aa6b5 pmid: 19381107 |
| [33] |
MANCIA G, LAURENT S, AGABITI-ROSEI E, et al. Reappraisal of European guidelines on hypertension management: a European Society of Hypertension Task Force document[J]. J Hypertens, 2009, 27(11):2121-2158.
doi: 10.1097/HJH.0b013e328333146d pmid: 19838131 |
| [34] |
BÖHM M, SCHUMACHER H, TEO K K, et al. Achieved blood pressure and cardiovascular outcomes in high-risk patients: results from ONTARGET and TRANSCEND trials[J]. Lancet, 2017, 389(10085):2226-2237.
doi: S0140-6736(17)30754-7 pmid: 28390695 |
| [35] |
MANCIA G, KJELDSEN S E, ZAPPE D H, et al. Cardiovascular outcomes at different on-treatment blood pressures in the hypertensive patients of the VALUE trial[J]. Eur Heart J, 2016, 37(12):955-964.
doi: 10.1093/eurheartj/ehv633 pmid: 26590384 |
| [36] |
VERDECCHIA P, STAESSEN J A, ANGELI F, et al. Usual versus tight control of systolic blood pressure in non-diabetic patients with hypertension (Cardio-Sis): an open-label randomised trial[J]. Lancet, 2009, 374(9689):525-533.
doi: 10.1016/S0140-6736(09)61340-4 pmid: 19683638 |
| [37] |
CARLBERG B. Time to lower treatment BP targets for hypertension?[J]. Lancet, 2009, 374(9689):503-504.
doi: 10.1016/S0140-6736(09)61467-7 pmid: 19683626 |
| [38] |
CHOBANIAN A V, BAKRIS G L, BLACK H R, et al. Seventh report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure[J]. Hypertension, 2003, 42(6):1206-1252.
doi: 10.1161/01.HYP.0000107251.49515.c2 pmid: 14656957 |
| [39] |
WRIGHT JT JR, BAKRIS G, GREENE T, et al. Effect of blood pressure lowering and antihypertensive drug class on progression of hypertensive kidney disease: results from the AASK trial[J]. JAMA, 2002, 288(19):2421-2431.
doi: 10.1001/jama.288.19.2421 URL |
| [40] |
MANCIA G, DE BACKER G, DOMINICZAK A, et al. 2007 Guidelines for the management of arterial hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2007, 28(12):1462-1536.
doi: 10.1093/eurheartj/ehm236 pmid: 17562668 |
| [41] | 中国高血压防治指南修订委员会. 中国高血压防治指南2010[J]. 中华心血管病杂志, 39(7):579-616. |
| LIU L S, Writing Group of 2010 Chinese Guidelines for the Management of Hypertension. 2010 Chinese guidelines for the management of hypertension[J]. Zhonghua Xin Xue Guan Bing Za Zhi, 39(7):579-615. | |
| [42] |
SCHRIER R W, ESTACIO R O, ESLER A, et al. Effects of aggressive blood pressure control in normotensive type 2 diabetic patients on albuminuria, retinopathy and strokes[J]. Kidney Int, 2002, 61(3):1086-1097.
doi: 10.1046/j.1523-1755.2002.00213.x pmid: 11849464 |
| [43] | WEBER M A, MATERSON B J. Hypertension guidelines: a major reappraisal critically examines the available evidence[J]. J Clin Hypertens(Greenwich), 2010, 12(4):229-236. |
| [44] |
ARONOW W S. What should the optimal blood pressure goal be in patients with diabetes mellitus or chronic kidney disease?[J]. Arch Med Sci, 2012, 8(3):399-402.
doi: 10.5114/aoms.2012.29395 pmid: 22851990 |
| [45] | 施仲伟. 血压目标将有回调,综合干预必须加强:从指南更新看高血压防治新动向[J]. 中华高血压杂志, 2012, 20(6):512-514. |
| SHI Z W. The blood pressure target will have a correction, and comprehensive intervention must be strengthened: new trends in hypertension prevention and control seen from the update of guidelines[J]. Chin J Hypertens, 2012, 20(6):512-514. | |
| [46] |
MANCIA G, FAGARD R, NARKIEWICZ K, et al. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)[J]. Eur Heart J, 2013, 34(28):2159-2219.
doi: 10.1093/eurheartj/eht151 pmid: 23771844 |
| [47] |
American Diabetes Association. Standards of medical care in diabetes—2013[J]. Diabetes Care, 2013, 36(Suppl 1):S11-S66.
doi: 10.2337/dc13-S011 URL |
| [48] | WHELTON P K, CAREY R M, ARONOW W S, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines[J]. Hypertension, 2018, 71(6):e13-e115. |
| [49] |
UMEMURA S, ARIMA H, ARIMA S, et al. The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019)[J]. Hypertens Res, 2019, 42(9):1235-1481.
doi: 10.1038/s41440-019-0284-9 pmid: 31375757 |
| [50] |
RABI D M, MCBRIEN K A, SAPIR-PICHHADZE R, et al. Hypertension Canada's 2020 Comprehensive Guidelines for the Prevention, Diagnosis, Risk Assessment, and Treatment of Hypertension in Adults and Children[J]. Can J Cardiol,2020, 36(5):596-624.
doi: 10.1016/j.cjca.2020.02.086 URL |
| [51] |
WILMOT K A, O'FLAHERTY M, CAPEWELL S, et al. Coronary Heart Disease Mortality Declines in the United States From 1979 Through 2011: Evidence for Stagnation in Young Adults, Especially Women[J]. Circulation,2015, 132(11):997-1002.
doi: 10.1161/CIRCULATIONAHA.115.015293 URL |
| [52] |
MA J, WARD E M, SIEGEL R L, et al. Temporal Trends in Mortality in the United States, 1969-2013[J]. JAMA, 2015, 314(16):1731-1739.
doi: 10.1001/jama.2015.12319 pmid: 26505597 |
| [53] |
SIDNEY S, QUESENBERRY CP JR, JAFFE M G, et al. Recent Trends in Cardiovascular Mortality in the United States and Public Health Goals[J]. JAMA Cardiol, 2016, 1(5):594-599.
doi: 10.1001/jamacardio.2016.1326 pmid: 27438477 |
| [54] |
MATERSON B J. JNC 8 at last! No Holy Grail in hand, but useful recommendations[J]. J Clin Hypertens (Greenwich), 2014, 16(4):249-250.
doi: 10.1111/jch.12283 pmid: 24621299 |
| [55] |
FINKS S, REPLEY T L. Sorting it out: what JNC 8 is and what it is not[J]. J Manag Care Spec Pharm, 2015, 21(2):110-112.
doi: 10.18553/jmcp.2015.21.2.110 pmid: 25614999 |
| [56] |
MATERSON B J. JNC 8 transmogrified[J]. J Clin Hypertens (Greenwich), 2013, 15(10):704.
doi: 10.1111/jch.12174 pmid: 24088275 |
| [57] |
BAUCHNER H, FONTANAROSA P B, GOLUB R M. Updated guidelines for management of high blood pressure: recommendations, review, and responsibility[J]. JAMA, 2014, 311(5):477-478.
doi: 10.1001/jama.2013.284432 pmid: 24352759 |
| [58] |
GIBBONS G H, SHURIN S B, MENSAH G A, et al. Refocusing the agenda on cardiovascular guidelines: an announcement from the National Heart, Lung, and Blood Institute[J]. Circulation, 2013, 128(15):1713-1715.
doi: 10.1161/CIRCULATIONAHA.113.004587 pmid: 23785001 |
| [59] |
GIBBONS G H, HAROLD J G, JESSUP M, et al. The next steps in developing clinical practice guidelines for prevention[J]. Circulation, 2013, 128(15):1716-1717.
doi: 10.1161/CIRCULATIONAHA.113.005548 pmid: 23929910 |
| [60] |
JAMES P A, OPARIL S, CARTER B L, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8)[J]. JAMA, 2014, 311(5):507-520.
doi: 10.1001/jama.2013.284427 pmid: 24352797 |
| [61] |
BENAVENTE O R, WHITE C L, PEARCE L, et al. The Secondary Prevention of Small Subcortical Strokes (SPS3) study[J]. Int J Stroke, 2011, 6(2):164-175.
doi: 10.1111/j.1747-4949.2010.00573.x pmid: 21371282 |
| [62] |
SPS 3 Investigators; BENAVENTE O R, HART R G, MCCLURE L A, et al. Effects of clopidogrel added to aspirin in patients with recent lacunar stroke[J]. N Engl J Med, 2012, 367(9):817-825.
doi: 10.1056/NEJMoa1204133 URL |
| [63] |
SPS 3 Study Group; BENAVENTE O R, COFFEY C S, CONWIT R, et al. Blood-pressure targets in patients with recent lacunar stroke: the SPS3 randomised trial[J]. Lancet, 2013, 382(9891):507-515.
doi: 10.1016/S0140-6736(13)60852-1 pmid: 23726159 |
| [64] |
ACCORD Study Group; BUSE J B, BIGGER J T, BYINGTON R P, et al. Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial: design and methods[J]. Am J Cardiol, 2007, 99(12 A):21i-33i.
pmid: 17599422 |
| [65] |
CUSHMAN W C, GRIMM RH JR, CUTLER J A, et al. Rationale and design for the blood pressure intervention of the Action to Control Cardiovascular Risk in Diabetes (ACCORD) trial[J]. Am J Cardiol, 2007, 99(12A):44i-55i.
pmid: 17599425 |
| [66] |
ACCORD Study Group; CUSHMAN W C, EVANS G W, BYINGTON R P, et al. Effects of intensive blood-pressure control in type 2 diabetes mellitus[J]. N Engl J Med, 2010, 362(17):1575-1585.
doi: 10.1056/NEJMoa1001286 URL |
| [67] | Working Group Report: Expert Panel on a Hypertension Treatment Trial Initiative Meeting Summary[R/OL]. (2007-1-16)[2023-7-8]. https://www.nhlbi.nih.gov/sites/default/files/media/docs/hypertsnsion-full.pdf. |
| [68] |
AMBROSIUS W T, SINK K M, FOY C G, et al. The design and rationale of a multicenter clinical trial comparing two strategies for control of systolic blood pressure: the Systolic Blood Pressure Intervention Trial (SPRINT)[J]. Clin Trials, 2014, 11(5):532-546.
doi: 10.1177/1740774514537404 pmid: 24902920 |
| [69] |
VERDECCHIA P, ANGELI F, REBOLDI G, et al. The SPRINT trial[J]. J Am Soc Hypertens, 2015, 9(10):750-753.
doi: S1933-1711(15)00667-1 pmid: 26506129 |
| [70] |
SPRINT Research Group; WRIGHT JT JR, WILLIAMSON J D, WHELTON P K, et al. A Randomized Trial of Intensive versus Standard Blood-Pressure Control[J]. N Engl J Med, 2015, 373(22):2103-2116.
doi: 10.1056/NEJMoa1511939 URL |
| [71] |
GREENLAND P, PETERSON E. The New 2017 ACC/AHA Guidelines “Up the Pressure” on Diagnosis and Treatment of Hypertension[J]. JAMA, 2017, 318(21):2083-2084.
doi: 10.1001/jama.2017.18605 URL |
| [72] |
Kidney Disease: Improving Global Outcomes KDIGO Blood Pressure Work Group. KDIGO 2021 Clinical Practice Guideline for the Management of Blood Pressure in Chronic Kidney Disease[J]. Kidney Int, 2021, 99(3S):S1-S87.
doi: 10.1016/j.kint.2020.11.003 URL |
| [73] |
MYERS M G, GODWIN M, DAWES M, et al. Measurement of blood pressure in the office: recognizing the problem and proposing the solution[J]. Hypertension, 2010, 55(2):195-200.
doi: 10.1161/HYPERTENSIONAHA.109.141879 pmid: 20038756 |
| [74] |
KJELDSEN S E, LUND-JOHANSEN P, NILSSON P M, et al. Unattended Blood Pressure Measurements in the Systolic Blood Pressure Intervention Trial: Implications for Entry and Achieved Blood Pressure Values Compared With Other Trials[J]. Hypertension, 2016, 67(5):808-812.
doi: 10.1161/HYPERTENSIONAHA.116.07257 pmid: 27001295 |
| [75] |
BUNDY J D, LI C, STUCHLIK P, et al. Systolic Blood Pressure Reduction and Risk of Cardiovascular Disease and Mortality: A Systematic Review and Network Meta-analysis[J]. JAMA Cardiol, 2017, 2(7):775-781.
doi: 10.1001/jamacardio.2017.1421 pmid: 28564682 |
| [76] |
BAKRIS G L. The Implications of Blood Pressure Measurement Methods on Treatment Targets for Blood Pressure[J]. Circulation, 2016, 134(13):904-905.
doi: 10.1161/CIRCULATIONAHA.116.022536 pmid: 27576778 |
| [77] | BAKRIS G L. Response by Bakris to Letter Regarding Article, "The Implications of Blood Pressure Measurement Methods on Treatment Targets for Blood Pressure"[J]. Circulation, 2017, 135(7):e47. |
| [78] |
WILLIAMSON J D, SUPIANO M A, APPLEGATE W B, et al. Intensive vs Standard Blood Pressure Control and Cardiovascular Disease Outcomes in Adults Aged ≥75 Years: A Randomized Clinical Trial[J]. JAMA, 2016, 315(24):2673-2682.
doi: 10.1001/jama.2016.7050 pmid: 27195814 |
| [79] |
JOHNSON K C, WHELTON P K, CUSHMAN W C, et al. Blood Pressure Measurement in SPRINT (Systolic Blood Pressure Intervention Trial)[J]. Hypertension, 2018, 71(5):848-857.
doi: 10.1161/HYPERTENSIONAHA.117.10479 pmid: 29531173 |
| [80] |
FILIPOVSKÝ J, SEIDLEROVÁ J, KRATOCHVÍL Z, et al. Automated compared to manual office blood pressure and to home blood pressure in hypertensive patients[J]. Blood Press, 2016, 25(4):228-234.
doi: 10.3109/08037051.2015.1134086 URL |
| [81] |
AGARWAL R. Implications of Blood Pressure Measurement Technique for Implementation of Systolic Blood Pressure Intervention Trial (SPRINT)[J]. J Am Heart Assoc, 2017, 6(2):e004536.
doi: 10.1161/JAHA.116.004536 URL |
| [82] |
BAUER F, SEIBERT F S, ROHN B, et al. Attended Versus Unattended Blood Pressure Measurement in a Real Life Setting[J]. Hypertension, 2018, 71(2):243-249.
doi: 10.1161/HYPERTENSIONAHA.117.10026 pmid: 29255074 |
| [83] |
PAINI A, BERTACCHINI F, STASSALDI D, et al. Unattended versus attended blood pressure measurement: Mean values and determinants of the difference[J]. Int J Cardiol, 2019, 274:305-310.
doi: S0167-5273(18)30951-3 pmid: 29945805 |
| [84] |
CHENG R Z, BHALLA V, CHANG T I, et al. Comparison of routine and automated office blood pressure measurement[J]. Blood Press Monit, 2019, 24(4):174-178.
doi: 10.1097/MBP.0000000000000392 pmid: 31116155 |
| [85] |
YUSUF S, LONN E. The SPRINT and the HOPE-3 Trial in the Context of Other Blood Pressure-Lowering Trials[J]. JAMA Cardiol, 2016, 1(8):857-858.
doi: 10.1001/jamacardio.2016.2169 pmid: 27602555 |
| [86] |
FILIPPONE E J, FOY A J. Blood pressure management in the wake of SPRINT[J]. Clev Clin J Med, 2016, 83(3):196-198.
doi: 10.3949/ccjm.83a.16015 pmid: 26974990 |
| [87] |
KJELDSEN S E, NARKIEWICZ K, HEDNER T, et al. The SPRINT study: Outcome may be driven by difference in diuretic treatment demasking heart failure and study design may support systolic blood pressure target below 140 mmHg rather than below 120 mmHg[J]. Blood Press, 2016, 25(2):63-66. 88.
doi: 10.3109/08037051.2015.1130775 URL |
| [88] |
LONN E M, YUSUF S. Should Patients With Cardiovascular Risk Factors Receive Intensive Treatment of Hypertension to <120/80 mm Hg Target? An Antagonist View From the HOPE-3 Trial (Heart Outcomes Evaluation-3)[J]. Circulation, 2016, 134(18):1311-1313.
doi: 10.1161/CIRCULATIONAHA.116.023264 URL |
| [89] |
SHAPIRO B P, AMBROSIUS W T, BLACKSHEAR J L, et al. Impact of Intensive Versus Standard Blood Pressure Management by Tertiles of Blood Pressure in SPRINT (Systolic Blood Pressure Intervention Trial)[J]. Hypertension, 2018, 71:1064-1074.
doi: 10.1161/HYPERTENSIONAHA.117.10646 pmid: 29712745 |
| [90] | LONN E, BOSCH J, POGUE J, et al. Novel Approaches in Primary Cardiovascular Disease Prevention: The HOPE-3 Trial Rationale, Design, and Participants' Baseline Characteristics[J]. Can J Cardiol, 2016, 36(3):311-318. |
| [91] |
LONN E M, BOSCH J, LÓPEZ-JARAMILLO P, et al. Blood-Pressure Lowering in Intermediate-Risk Persons without Cardiovascular Disease[J]. N Engl J Med, 2016, 374(21):2009-2020.
doi: 10.1056/NEJMoa1600175 URL |
| [92] |
PAIS P, JUNG H, DANS A, et al. Impact of blood pressure lowering, cholesterol lowering and their combination in Asians and non-Asians in those without cardiovascular disease: an analysis of the HOPE 3 study[J]. Eur J Prev Cardiol, 2019, 26(7):681-697.
doi: 10.1177/2047487318819019 pmid: 30537846 |
| [93] |
ZHANG S, WU S, REN J, et al. Strategy of blood pressure intervention in the elderly hypertensive patients (STEP): Rational, design, and baseline characteristics for the main trial[J]. Contemp Clin Trials, 2020, 89:105913.
doi: 10.1016/j.cct.2019.105913 URL |
| [94] | 张宇清, 苗欢欢, 杨世杰, 等. 谋定后动——新近高血压重要研究中的启示[J]. 中国介入心脏病学杂志, 2022, 30(7):518-521. |
| ZHANG Y Q, MIAO H H, YANG S J, et al. Planning after Action: Enlightenment from Recent Important Research on Hypertension[J]. Chin J Interv Cardiol, 2022, 30(7):518-521. | |
| [95] |
ZHANG W, ZHANG S, DENG Y, et al. Trial of Intensive Blood-Pressure Control in Older Patients with Hypertension[J]. N Engl J Med, 2021, 385(14):1268-1279.
doi: 10.1056/NEJMoa2111437 URL |
| [96] |
NELSON M R. Moving the Goalposts for Blood Pressure-Time to Act[J]. N Engl J Med, 2021, 385(14):1328-1329.
doi: 10.1056/NEJMe2112992 URL |
| [97] |
BENETOS A, PERSU A, KREUTZ R. Hypertension in older patients: a STEP forward?[Formula: see text][J]. Blood Press, 2022, 31(1):118-120.
doi: 10.1080/08037051.2022.2075826 URL |
| [98] |
UNGER T, BORGHI C, CHARCHAR F, et al. 2020 International Society of Hypertension global hypertension practice guidelines[J]. J Hypertens, 2020, 38(6):982-1004.
doi: 10.1097/HJH.0000000000002453 pmid: 32371787 |
| [99] |
AL-MAKKI A, DIPETTE D, WHELTON P K, et al. Hypertension Pharmacological Treatment in Adults: A World Health Organization Guideline Executive Summary[J]. Hypertension, 2022, 79(1):293-301.
doi: 10.1161/HYPERTENSIONAHA.121.18192 URL |
| [100] |
MANCIA G, KREUTZ R, BRUNSTRÖM M, et al. 2023 ESH Guidelines for the management of arterial hypertension The Task Force for the management of arterial hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA)[J]. J Hypertens, 2023, 41(12):1874-2071.
doi: 10.1097/HJH.0000000000003480 URL |
| [101] |
CHEN X, BARYWANI S B, HANSSON P O, et al. High-normal blood pressure conferred higher risk of cardiovascular disease in a random population sample of 50-year-old men: A 21-year follow-up[J]. Medicine (Baltimore), 2020, 99(17):e19895.
doi: 10.1097/MD.0000000000019895 URL |
| [102] |
MUSCAT D M, MORRIS G M, BELL K, et al. Benefits and Harms of Hypertension and High-Normal Labels: A Randomized Experiment[J]. Circ Cardiovasc Qual Outcomes, 2021, 14(4):e007160.
doi: 10.1161/CIRCOUTCOMES.120.007160 URL |
| [103] |
HAMER M, BATTY G D, STAMATAKIS E, et al. Hypertension awareness and psychological distress[J]. Hypertension, 2010, 56(3):547-550.
doi: 10.1161/HYPERTENSIONAHA.110.153775 pmid: 20625078 |
| [104] |
RANTANEN A T, KORKEILA J J A, LÖYTTYNIEMI E S, et al. Awareness of hypertension and depressive symptoms: a cross-sectional study in a primary care population[J]. Scand J Prim Health Care, 2018, 36(3):323-328.
doi: 10.1080/02813432.2018.1499588 URL |
| [105] | 王继光. 必须高度重视降压药物治疗的安全性[J]. 中华心血管病杂志, 2022, 50(7):625-626. |
| WANG J G. [Taking the safety of antihypertensive drug treatment seriously][J]. Zhonghua Xin Xue Guan Bing Za Zhi, 2022, 50(7):625-626. | |
| [106] | 潘锋. CHINOM研究填补国内外心血管疾病同类研究空白——正常高值血压人群如无其他严重疾病无需服用降压药[J]. 中国医药科学, 2022, 12(11):1-4. |
| PAN F. CHINOM research fills the gap in similar research on cardiovascular diseases both domestically and internationally - people with normal high blood pressure do not need to take antihypertensive drugs if there are no other serious diseases[J]. China Med Pharm, 2022, 12(11):1-4. | |
| [107] | 医师报循环频道. 该怎么看待CHINOM研究?张新华教授等独家解读[EB/OL]. 医师报循环频道.(2022-5-17) [2023-7-17]. https://mp.pdnews.cn/Pc/ArtInfoApi/article?id=28689628. |
| [108] |
KREUTZ R, BRUNSTRÖM M, THOMOPOULOS C, et al. Do recent meta-analyses truly prove that treatment with blood pressure-lowering drugs is beneficial at any blood pressure value, no matter how low? A critical review[J]. J Hypertens, 2022, 40(5):839-846.
doi: 10.1097/HJH.0000000000003056 URL |
| [109] |
BASSLER D, MONTORI V M, BRIEL M, et al. Early stopping of randomized clinical trials for overt efficacy is problematic[J]. J Clin Epidemiol, 2008, 61(3):241-246.
doi: 10.1016/j.jclinepi.2007.07.016 pmid: 18226746 |
| [110] |
NOLDE J M, BEANEY T, CARNAGARIN R, et al. Global Impact of Different Blood Pressure Thresholds in 4 021 690 Participants of the May Measurement Month Initiative[J]. Hypertension, 2022, 79(7):1497-1505.
doi: 10.1161/HYPERTENSIONAHA.122.19144 URL |
| [1] | QIAN Ying, MA Xiaobo, GAO Chenni, ZHANG Chunli, MA Jun, ZHANG Wen, CHEN Xiaonong. Association between hyperuricemia and hypertension in chronic kidney disease [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 160-165. |
| [2] | YANG Yang, WU Qinmi, FENG Yulan, ZHANG Bei, FU Yi. Factors related to enlarged perivascular spaces and lacunes in patients with hypertension [J]. Journal of Diagnostics Concepts & Practice, 2021, 20(04): 372-377. |
| [3] | LI Zhoutong, ZHANG Wei, WANG Jiguang. Accuracy of home versus ambulatory blood pressure monitoring in the diagnosis of white-coat and masked hypertension [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(05): 487-493. |
| [4] | WANG Lijuan, PAN Zilai, SU Wenting, XU Jingci, RAO Min, LIU Xiao. Feasibility study on the portal vein imaging using non-contrast-enhanced magnetic resonance angiography with flow inversion recovery sequence in the cirrhotic portal hypertension [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(05): 494-498. |
| [5] | HUANG Yongyan, YANG Lina, CAO Jiumei, WANG Wei. Cloud-based solution assisted blood pressure management in outpatient setting [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(03): 319-324. |
| [6] | CHEN Chen, ZHANG Yue, HU Xiaobo. The clinical evaluation and optimization of alarm Threshold setting for Sysmex UF5000 UTI [J]. Journal of Diagnostics Concepts & Practice, 2020, 19(02): 168-171. |
| [7] | WEI Xiaomin, ZHANG Yuanyuan, DONG Liang, XIA Jingwen, GONG Yi, YU Yongping, LI Shengqing. A prospective study on incidence of chronic thromboembolic pulmonary hypertension after pulmonary thromboembolism [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(1): 37-43. |
| [8] | WANG Yajuan, GUO Qianhui, ZHANG Dongyan, CHENG Yibang, CHEN Ling, ZHU Dingliang, LI Yan. Prevalence of overweight and obesity and analysis of blood pressure related factors among children and adolescents in Xinzhuang community, Shanghai [J]. Journal of Diagnostics Concepts & Practice, 2019, 18(05): 575-580. |
| [9] | DONG Fang, ZHANG Yihui, GUO Jian, LIU Jinming. Correlation between nutritional risk and exercise tolerance in patients with idiopathic pulmonary arterial hypertension [J]. Journal of Diagnostics Concepts & Practice, 2018, 17(06): 664-669. |
| [10] | CHEN Hui, GUO Qianhui, XU Jie, CHENG Yibang, ZHANG Dongyan, WANG Ying, HUANG Qifang, SHENG Changsheng, LI Yan. Prevalence and determinants of asymptomatic intracranial artery stenosis assessed by transcranial Doppler ultrosonography [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(06): 592-595. |
| [11] | ZHU Bingliang, SHA Jie. Analysis of causes of upper gastrointestinal bleeding in portal hypertension patients with varicosity at different positions of esophageal and gastric fundus vein [J]. Journal of Diagnostics Concepts & Practice, 2017, 16(01): 114-117. |
| [12] | . [J]. Journal of Diagnostics Concepts & Practice, 2016, 15(04): 371-375. |
| [13] | . [J]. Journal of Diagnostics Concepts & Practice, 2016, 15(04): 405-409. |
| [14] | . [J]. Journal of Diagnostics Concepts & Practice, 2015, 14(04): 318-323. |
| [15] | . [J]. Journal of Diagnostics Concepts & Practice, 2015, 14(03): 262-266. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||