Journal of Diagnostics Concepts & Practice ›› 2023, Vol. 22 ›› Issue (06): 520-526.doi: 10.16150/j.1671-2870.2023.06.002
• Expert forum • Previous Articles Next Articles
ZHOU Yan, ZHANG Min( )
)
Received:2023-10-08
Online:2023-12-25
Published:2024-03-18
Contact:
ZHANG Min
E-mail:maggie_zhangmin@163.com
CLC Number:
ZHOU Yan, ZHANG Min. Current status and countermeasures of diagnosis and treatment of mild bronchial asthma in China[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(06): 520-526.
Table 1
Classification of initial and follow-up patients
| 分级 | 根据症状及肺功能评估 |
|---|---|
| 初诊* | (1)哮喘发作<1次/d; |
| (2)可能影响活动和(或)睡眠; | |
| (3)夜间哮喘发作<1次/周; | |
| (4)FEV1占预计值%≥80%,或PEF≥80% 个人最佳值且PEF 变异率<30% | |
| 复诊 | 经过第1级和第2级治疗药物能达到完全控制 |
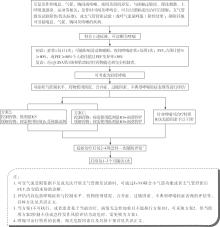
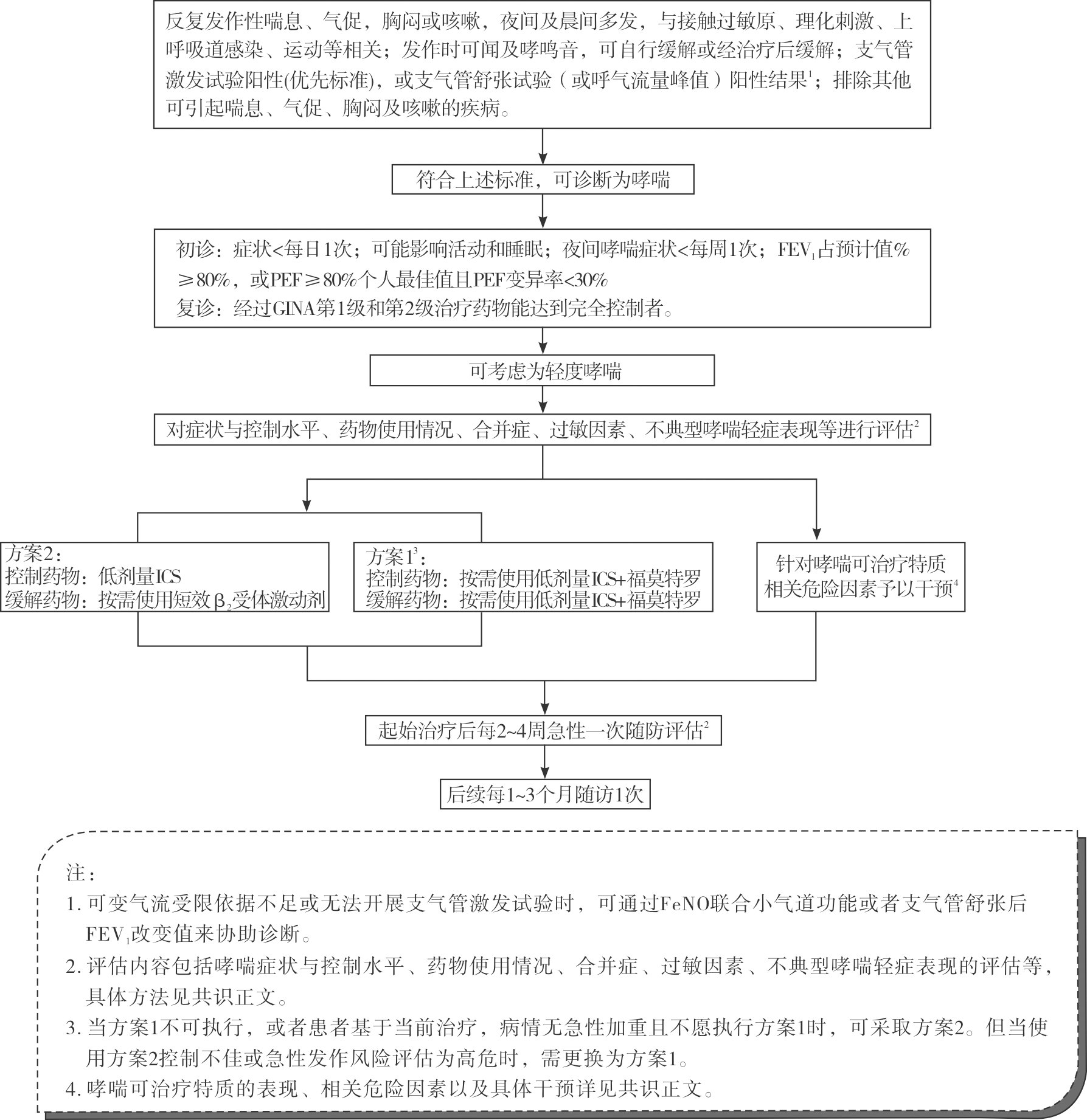
Table 2
Treatment regime
| 路径 | 方案 |
|---|---|
| 优选路径 | 按需低剂量ICS+快速起效的长效β2受体激动剂(如福莫特罗) |
| 备选路径 | (1)维持治疗的低剂量ICS+按需给予短效β2受体激动剂(SABA) |
| (2)维持治疗的其他药物+按需给予SABA | |
| (3)按需ICS-SABA |
| [1] | 中华医学会呼吸病学分会哮喘学组. 支气管哮喘防治指南(2020年版)[J]. 中华结核和呼吸杂志, 2020, 43(12):1023-1048. |
| Asthma Group, Respiratory Society of Chinese Medical Association. Guidelines for bronchial asthma prevent and management(2020 edition) Asthma group of Chinese Throacic Society[J]. Zhonghua Jie He He Hu Xi Za Zhi, 2020, 43(12):1023-1048. | |
| [2] |
HUANG K, YANG T, XU J, et al. Prevalence, risk factors, and management of asthma in China: a national cross-sectional study[J]. Lancet, 2019, 394(10196):407-418.
doi: S0140-6736(19)31147-X pmid: 31230828 |
| [3] | 中国医药教育协会儿科专业委员会, 中华医学会儿科学分会呼吸学组哮喘协作组, 中国医师协会呼吸医师分会儿科呼吸工作委员会, 等. 中国儿童支气管哮喘诊治现状及发展策略(2022)[J]. 中华实用儿科临床杂志, 2023, 38(9):647-680. |
| Pediatric Professional Committee of Chinese Medical Education Association, Asthma Collaborative Group of Respiratory Group of Pediatrics Branch of Chinese Medical Association, Pediatric Respiratory Working Committee of Respiratory Physician Branch of Chinese Medical Doctor Association, et al. Current situation and development strategies of diagnosis and treatment of bronchial asthma in children in China (2022)[J]. Chin J Appl Clin Pediatr, 2023, 38(9):647-680. | |
| [4] | 中华医学会呼吸病学分会. 轻度支气管哮喘诊断与治疗中国专家共识(2023)[J]. 中华结核和呼吸杂志, 2023, 46(9):880-896. |
| Respiratory Society of Chinese Medical Association. Expert consensus on the diagnosis, treatment and management of mild bronchial asthma in China (2023 edition)[J]. Zhonghua Jie He He Hu Xi Za Zhi, 2023, 46(9):880-896. | |
| [5] |
VAN SCHAYCK C P, VAN DER HEIJDEN F M, VAN DEN BOOM G, et al. Underdiagnosis of asthma: is the doctor or the patient to blame? The DIMCA project[J]. Thorax, 2000, 55(7):562-565.
doi: 10.1136/thorax.55.7.562 pmid: 10856315 |
| [6] |
ADAMS R J, WILSON D H, APPLETON S, et al. Underdiagnosed asthma in South Australia[J]. Thorax, 2003, 58(10):846-850.
pmid: 14514934 |
| [7] |
BACKER V, HARMSEN L, LUND T, et al. A 3-year longitudinal study of asthma quality of life in undiagnosed and diagnosed asthma patients[J]. Int J Tuberc Lung Dis, 2007, 11(4):463-469.
pmid: 17394695 |
| [8] |
DE MARCO R, CERVERI I, BUGIANI M, et al. An undetected burden of asthma in Italy: the relationship between clinical and epidemiological diagnosis of asthma[J]. Eur Respir J, 1998, 11(3):599-605.
pmid: 9596109 |
| [9] |
SCHOETTLER N, OBER C. Genetic architecture of mode-rate-to-severe asthma mirrors that of mild asthma[J]. J Allergy Clin Immunol, 2019, 144(6):1521-1523.
doi: 10.1016/j.jaci.2019.09.003 URL |
| [10] |
CHETTA A, FORESI A, DEL DONNO M, et al. Airways remodeling is a distinctive feature of asthma and is related to severity of disease[J]. Chest, 1997, 111(4):852-857.
pmid: 9106559 |
| [11] |
HALWANI R, AL-MUHSEN S, HAMID Q. Airway remodeling in asthma[J]. Curr Opin Pharmacol, 2010, 10(3):236-245.
doi: 10.1016/j.coph.2010.06.004 pmid: 20591736 |
| [12] | HUANG H, HUA W, CHEN R, et al. Perspectives and Management of Atypical Asthma in Chinese Specialists and Primary Care Practitioners-A Nationwide Questionnaire Survey[J]. Front Med (Lausanne), 2021, 8:727381. |
| [13] |
CAMINATI M, BETTONCELLI G, MAGNONI M S, et al. The level of control of mild asthma in general practice: an observational community based study[J]. J Asthma, 2014, 51(1):91-96.
doi: 10.3109/02770903.2013.843098 URL |
| [14] |
DING B, SMALL M. Disease burden of mild asthma in China[J]. Respirology, 2018, 23(4):369-377.
doi: 10.1111/resp.13189 pmid: 29052915 |
| [15] | FITZGERALD J M, BARNES P J, CHIPPS B E, et al. The burden of exacerbations in mild asthma: a systematic review[J]. ERJ Open Res, 2020, 6(3):00359-2019. |
| [16] |
RABE K F, ADACHI M, LAI C K, et al. Worldwide severity and control of asthma in children and adults: the global asthma insights and reality surveys[J]. J Allergy Clin Immunol, 2004, 114(1):40-47.
doi: 10.1016/j.jaci.2004.04.042 URL |
| [17] | 林江涛. 轻度哮喘的流行病学、临床特点及治疗策略[J]. 中华结核和呼吸杂志, 2015, 38(3):236-238. |
| LIN J T. Epidemiology, clinical characteristics, and treatment strategies for mild asthma[J]. Zhonghua Jie He He Hu Xi Za Zhi, 2015 ;38(3):236-238. | |
| [18] |
SADATSAFAVI M, LYND L, MARRA C, et al. Direct health care costs associated with asthma in British Columbia[J]. Can Respir J, 2010, 17(2):74-80.
doi: 10.1155/2010/361071 pmid: 20422063 |
| [19] | Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention,2023. Updated May 2023[EB/OL]. [2023 03 01]. http://www.ginasthma.org. |
| [20] | 中华医学会呼吸病学分会哮喘学组. 胸闷变异性哮喘诊治中国专家共识[J]. 中华医学杂志, 2023, 103(34):2662-2673. |
| Asthma Group, Respiratory Society of Chinese Medical Association. Expert consensus on the diagnosis and treatment of chest tightness variant asthma in China[J]. Chin Med J, 2023, 103(34):2662-2673. | |
| [21] |
BAO W, ZHANG X, YIN J, et al. Small-airway function variables in spirometry, fractional exhaled nitric oxide, and circulating eosinophils predicted airway hyperresponsiveness in patients with mild asthma[J]. J Asthma Allergy, 2021, 14:415-426.
doi: 10.2147/JAA.S295345 pmid: 33907426 |
| [22] |
HAO H, BAO W, XUE Y, et al. Spirometric changes in bronchodilation tests as predictors of asthma diagnosis and treatment response in patients with FEV(1) ≥ 80% predicted[J]. J Allergy Clin Immunol Pract, 2021, 9(8):3098-3108.e4.
doi: 10.1016/j.jaip.2021.03.015 URL |
| [23] |
BAO W, ZHANG X, LV C, et al. The value of fractional exhaled nitric oxide and forced mid-expiratory flow as predictive markers of bronchial hyperresponsiveness in adults with chronic cough[J]. J Allergy Clin Immunol Pract, 2018, 6(4):1313-1320.
doi: S2213-2198(17)30786-9 pmid: 29128336 |
| [24] |
HOU L, HAO H, HUANG G, et al. The value of small airway function parameters and fractional exhaled nitric oxide for predicting positive methacholine challenge test in asthmatics of different ages with FEV(1) ≥ 80% predicted[J]. Clin Transl Allergy, 2021, 11(1):e12007.
doi: 10.1002/clt2.v11.1 URL |
| [25] | 殷凯生. 支气管哮喘治疗中的几个新概念和新方法[J]. 中华结核和呼吸杂志, 2005, 28(11):746-748. |
| YIN K S. Several new concepts and new approaches in the treatment of bronchial asthma[J]. Zhonghua Jie He He Hu Xi Za Zhi, 2005, 28(11):746-748. | |
| [26] | 谢燕清, 郑劲平. 支气管激发试验的技术规范和质量控制[J]. 中华结核和呼吸杂志, 2012, 35(11):870-872. |
| XIE Y Q, ZHENG J P. Technical specification and qua-lity control of the bronchial provocation test[J]. Chin J Tuberc Respir Dis, 2012, 35(11):870-872. | |
| [27] | 郭娥, 高怡, 关伟杰, 等. 中国支气管激发试验开展现状调查[J]. 中国实用内科杂志, 2014(S1):48. |
| GUO E, GAO Y, GUAN W J, et al. Investigation of bronchial excitation test in China[J]. Chin J Pract Intern Med, 2014(S1):48. | |
| [28] |
BERGSTRÖM S E, BOMAN G, ERIKSSON L, et al. Asthma mortality among Swedish children and young adults, a 10 year study[J]. Respir Med, 2008, 102(9):1335-1341.
doi: 10.1016/j.rmed.2008.03.020 URL |
| [29] |
USMANI O S, HAN M K, KAMINSKY D A, et al. Seven pillars of small airways disease in asthma and copd: supporting opportunities for novel therapies[J]. Chest, 2021, 160(1):114-134.
doi: 10.1016/j.chest.2021.03.047 URL |
| [30] |
BAO W, TIAN X, HAO H, et al. Is small airway dysfunction an abnormal phenomenon for patients with normal forced expiratory volume in 1 second and the ratio of forced expiratory volume in 1 second to forced vital capacity?[J]. Ann Allergy Asthma Immunol, 2022, 128(1):68-77.e1.
doi: 10.1016/j.anai.2021.09.011 URL |
| [31] |
XUE Y, BAO W, ZHOU Y, et al. Small-airway dysfunction is involved in the pathogenesis of asthma: evidence from two mouse models[J]. J Asthma Allergy, 2021, 14:883-896.
doi: 10.2147/JAA.S312361 pmid: 34285515 |
| [32] | XUE Y, ZHOU Y, BAO W, et al. STAT3 and IL-6 Contribute to Corticosteroid Resistance in an OVA and Ozone-induced Asthma Model with Neutrophil Infiltration[J]. Front Mol Biosci, 2021, 8:717962. |
| [33] |
POSTMA D S, BRIGHTLING C, BALDI S, et al. Explo-ring the relevance and extent of small airways dysfunction in asthma (ATLANTIS): baseline data from a prospective cohort study[J]. Lancet Respir Med, 2019, 7(5):402-416.
doi: 10.1016/S2213-2600(19)30049-9 URL |
| [34] | 中华医学会呼吸病学分会肺功能专业组. 肺功能检查指南(第三部分)——组织胺和乙酰甲胆碱支气管激发试验[J]. 中华结核和呼吸杂志, 2014, 37(8):566-5671. |
| Pulmonary function Professional Group of Respiratory Diseases Branch of Chinese Medical Association. Guidelines for pulmonary function tests (Part Ⅲ) --- Hiistamine and acetylmethcholine bronchial challenge test[J]. Zhonghua Jie He He Hu Xi Za Zhi, 2014, 37(8):566-5671. | |
| [35] |
ZHANG X, XU Z, LIN J, et al. Sex differences of small airway function and fractional exhaled nitric oxide in patients with mild asthma[J]. Ann Allergy Asthma Immunol, 2023, 130(2):187-198.e3.
doi: 10.1016/j.anai.2022.11.010 URL |
| [36] |
LIU X, WANG X, YAO X, et al. Value of exhaled nitric oxide and FEF25-75 in identifying factors associated with chronic cough in allergic rhinitis[J]. Allergy Asthma Immunol Res, 2019, 11(6):830-845.
doi: 10.4168/aair.2019.11.6.830 URL |
| [37] | HAO H, PAN Y, XU Z, et al. Prediction of bronchodilation test in adults with chronic cough suspected of cough variant asthma[J]. Front Med (Lausanne), 2022, 9:987887. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||