Journal of Internal Medicine Concepts & Practice ›› 2025, Vol. 20 ›› Issue (03): 191-197.doi: 10.16138/j.1673-6087.2025.03.02
• Original article • Previous Articles Next Articles
TIAN Xiaofang1,2, LIU Liping2, YUAN Liying1,2, REN Hong1, WANG Zhaohui1( ), SHI Hao1()
), SHI Hao1()
Received:2025-03-24
Online:2025-06-28
Published:2025-09-01
Contact:
WANG Zhaohui, SHI Hao
E-mail:wzhaohui2001@163.com;shihaohp@163.com
CLC Number:
TIAN Xiaofang, LIU Liping, YUAN Liying, REN Hong, WANG Zhaohui, SHI Hao. Heavy and light chain renal amyloidosis with biclonal paraproteinemia: a case study and literature review[J]. Journal of Internal Medicine Concepts & Practice, 2025, 20(03): 191-197.

Figure 1
Renal biopsy pathological atlas
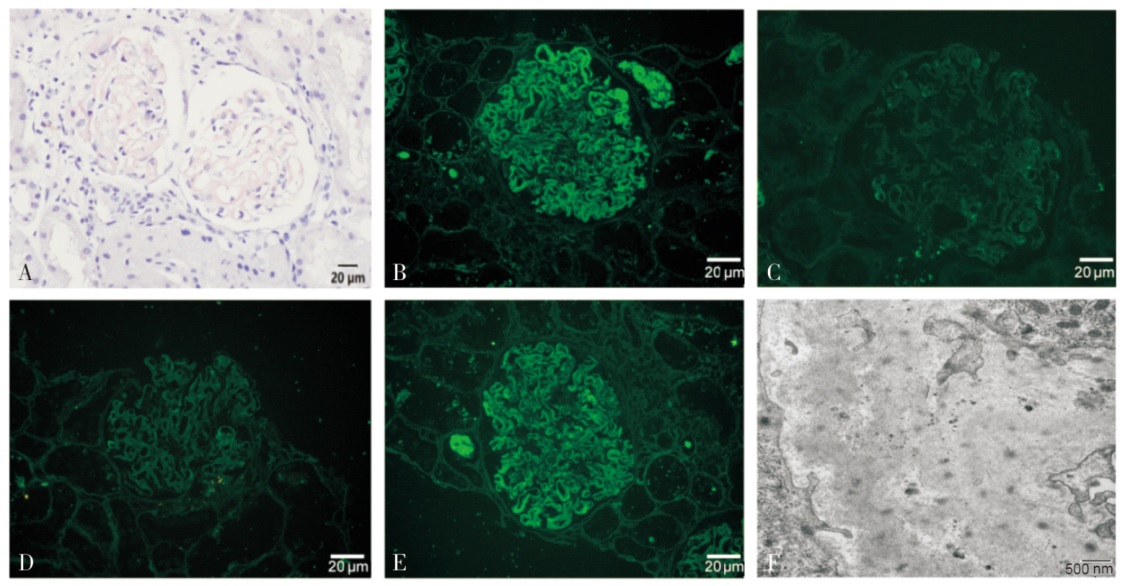
Figure 2
Changes in serum free λ light chain, κ/λ ratio and dFLC during treatment
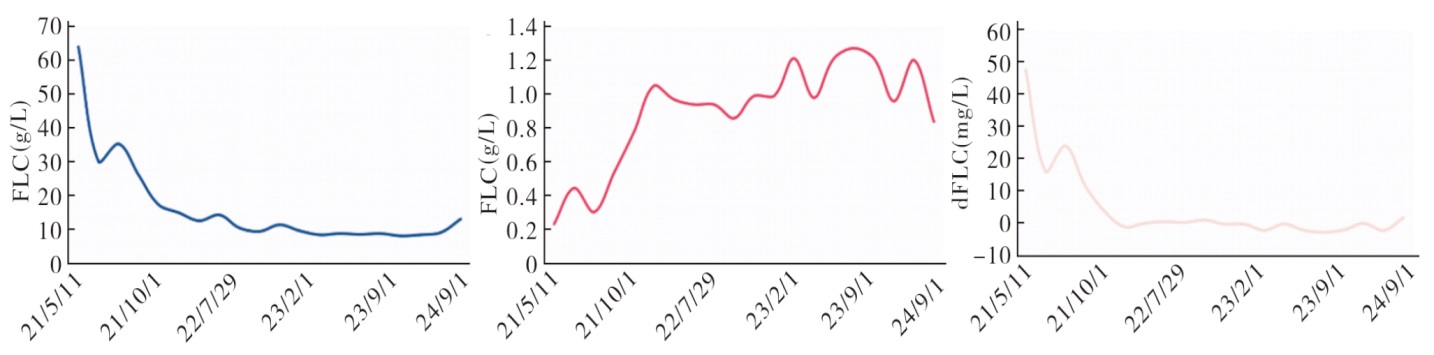

Figure 3
Changes in 24 h urine protein, serum albumin and serum creatinine during treatment
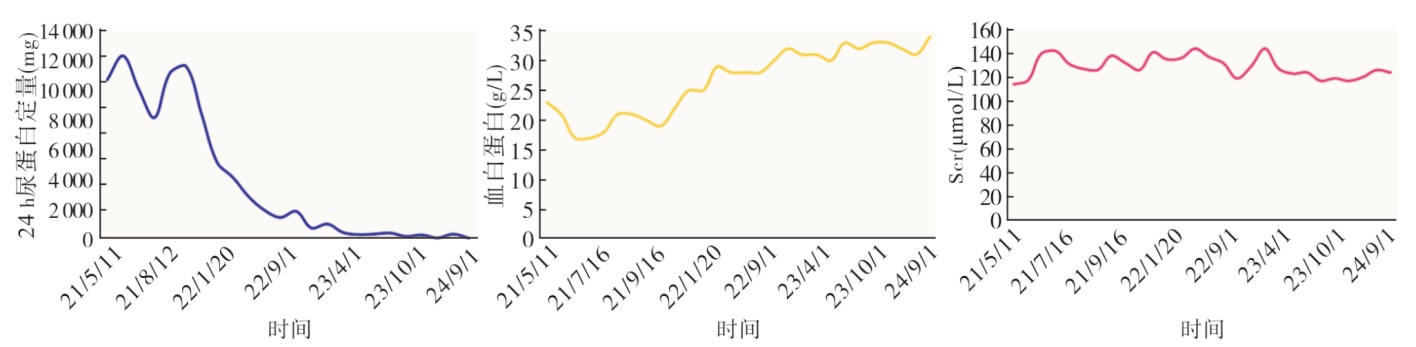
Table 1
Clinical characteristics and treatments of AL amyloidosis patients with biclonal paraproteinemia (without MM)
| 项目 | Julien等[ | Bouvet等[ | Pace等[ | Yan等[ | Dhaliwal等[ |
|---|---|---|---|---|---|
| 年龄(岁) | 59 | 51 | 80 | 46 | 68 |
| 性别 | 男性 | 男性 | 男性 | 男性 | 男性 |
| 血M蛋白类型 | IgM κ/IgG λ | IgG κ/IgA λ | IgG κ/IgA λ | IgA κ/IgG κ | IgM κ/IgM λ |
| 骨髓涂片或流式细胞检测 | 未报道 | 浆细胞3.60% | 浆细胞4.80% | 流式:克隆浆细胞0.86% | 流式:克隆B细胞13.00% |
| 累及器官 | 肾脏、周围神经 | 肾、肠道 | 心脏、肾脏、周围神经、肠道 | 支气管黏膜 | 肾脏、心脏 |
| 治疗 | 未报道 | MP方案 | MP方案 | CyBorD方案 | BDR方案后调整为Dara |
| [1] |
Wechalekar AD, Gillmore JD, Hawkins PN. Systemic amyloidosis[J]. Lancet, 2016, 387(10038):2641-2654.
doi: S0140-6736(15)01274-X pmid: 26719234 |
| [2] | Fotiou D, Dimopoulos MA, Kastritis E. Systemic AL amyloidosis: current approaches to diagnosis and management[J]. Hemasphere, 2020, 4(4):e454. |
| [3] |
Palladini G, Dispenzieri A, Gertz MA, et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes[J]. J Clin Oncol, 2012, 30(36):4541-4549.
doi: 10.1200/JCO.2011.37.7614 pmid: 23091105 |
| [4] | 中国系统性轻链型淀粉样变性协作组, 国家肾脏疾病临床医学研究中心, 国家血液系统疾病临床医学研究中心. 系统性轻链型淀粉样变性诊断和治疗指南(2021年修订)[J]. 中华医学杂志, 2021, 101(22):1646-1656. |
| [5] |
Palladini G, Hegenbart U, Milani P, et al. A staging system for renal outcome and early markers of renal response to chemotherapy in AL amyloidosis[J]. Blood, 2014, 124(15):2325-2332.
doi: 10.1182/blood-2014-04-570010 pmid: 25115890 |
| [6] |
Lolin YI, Chow J, Wickham NW. Monoclonal gammopathy of unknown significance and malignant paraproteinemia in Hong Kong[J]. Am J Clin Pathol, 1996, 106(4):449-456.
pmid: 8853031 |
| [7] |
Mullikin TC, Rajkumar SV, Dispenzieri A, et al. Clinical characteristics and outcomes in biclonal gammopathies[J]. Am J Hematol, 2016, 91(5):473-475.
doi: 10.1002/ajh.24319 pmid: 26840395 |
| [8] |
Spicka I, Merta M, Cieslar P, et al. [Renal impairment in monoclonal gammapathies. clinical study][J]. Cas Lek Cesk, 1995, 134(15):478-481.
pmid: 7585865 |
| [9] | Yan W, Li P, Wu C, et al. Case Report: Management of primary tracheobronchial light chain amyloidosis in a patient with biclonal cammopathy using a systemic bortezomib-based regimen[J]. Front Med (Lausanne), 2021, 8:728561. |
| [10] |
Coen M, Bornand A, Samii K, et al. Gastrointestinal amyloidosis in biclonal gammopathy[J]. Clin Lymphoma Myeloma Leuk, 2021, 21(7):e606-e610.
doi: 10.1016/j.clml.2021.02.015 pmid: 33785295 |
| [11] | Stammler F. Haemorrhagic diathesis as an early symptom of systemic amyloidosis[J]. Dtsch Med Wochenschr, 2006, 131(1-2):17-21. |
| [12] |
Julien J, Vital C, Vallat JM, et al. IgM demyelinative neuropathy with amyloidosis and biclonal gammopathy[J]. Ann Neurol, 1984, 15(4):395-399.
pmid: 6430211 |
| [13] |
Bouvet JP, Delrieu F. Polyarteritis nodosa associated with biclonal gammopathy of two-cell line origin and amyloidosis[J]. J Rheumatol, 1985, 12(1):168-170.
pmid: 2858589 |
| [14] |
Silver MM, Hearn SA, Walton JC et al. Immunogold quantitation of immunoglobulin light chains in renal amyloidosis and kappa light chain nephropathy[J]. Am J Pathol, 1990, 136(5):997-1007.
pmid: 1693473 |
| [15] |
Pace F, Gubitosi G, Giorgi A, et al. Idiopathic AL amyloidosis and biclonal paraproteinemia: a case report and review of the literature[J]. Amyloid, 2001, 8(3):215-219.
pmid: 11676298 |
| [16] | Dhaliwal A, Tripathi A, Ravi S. A case of μ heavy and λ light chain amyloidosis in a patient with bi-clonal (IgM κ and λ) gammopathy treated with daratumumab[J]. Cureus, 2024, 16(3):e56994. |
| [17] | Ravichandran S, Lachmann HJ, Wechalekar AD. Epidemiologic and survival trends in amyloidosis, 1987-2019[J]. N Engl J Med, 2020, 382(16):1567-1568. |
| [18] |
Leung N, Bridoux F, Hutchison CA, et al. Monoclonal gammopathy of renal significance: when MGUS is no longer undetermined or insignificant[J]. Blood, 2012, 120(22):4292-4295.
doi: 10.1182/blood-2012-07-445304 pmid: 23047823 |
| [19] |
Kyle RA, Robinson RA, Katzmann JA. The clinical aspects of biclonal gammopathies[J]. Am J Med, 1981, 71(6):999-1008.
pmid: 6797297 |
| [20] |
Palladini G, Russo P, Bosoni T, et al. Identification of amyloidogenic light chains requires the combination of serum-free light chain assay with immunofixation of serum and urine[J]. Clin Chem, 2009, 55(3):499-504.
doi: 10.1373/clinchem.2008.117143 pmid: 19131635 |
| [21] |
Clausen J, Christensen HE. Paraproteins and acid mucopolysaccharides in primary amyloidosis. biochemical and histologic studies of four human cases of primary amyloidosis[J]. Acta Pathol Microbiol Scand, 1964, 60:493-511.
pmid: 14154712 |
| [22] | Wechalekar AD, Cibeira MT, Gibbs SD, et al. Guidelines for non-transplant chemotherapy for treatment of systemic AL amyloidosis: EHA-ISA Working Group[J]. Amyloid, 2023, 30(1):3-17. |
| [23] |
Sachchithanantham S, Roussel M, Palladini G, et al. European collaborative study defining clinical profile outcomes and novel prognostic criteria in monoclonal immunoglobulin M-related light chain amyloidosis[J]. J Clin Oncol, 2016, 34(17):2037-2045.
doi: 10.1200/JCO.2015.63.3123 pmid: 27114592 |
| [24] | Paulus A, Manna A, Akhtar S, et al. Targeting CD38 with daratumumab is lethal to Waldenström macroglobulinaemia cells[J]. Br J Haematol, 2018, 183(2):196-211. |
| [25] |
Castillo JJ, Libby EN, Ansell SM, et al. Multicenter phase 2 study of daratumumab monotherapy in patients with previously treated Waldenström macroglobulinemia[J]. Blood Adv, 2020, 4(20):5089-5092.
doi: 10.1182/bloodadvances.2020003087 pmid: 33085756 |
| [26] | Kumar SK, Callander NS, Adekola K, et al. Systemic Light Chain Amyloidosis, Version 2.2023, NCCN Clinical Practice Guidelines in Oncology[J]. J Natl Compr Canc Netw, 2023, 21(1):67-81. |
| [1] | XU Lili, HU Xiaofan, LI Hao, WANG Weiming. Study on predictors for treatment efficacy of rituximab in patients with PLA2R-negative primary membranous nephropathy [J]. Journal of Diagnostics Concepts & Practice, 2025, 24(03): 279-285. |
| [2] | RUAN Yilin, XU Tian, FENG Xiaobei, XU Jing, SHI Hao, REN Hong. Invasive pulmonary aspergillosis secondary to immunosuppressive therapy in nephrotic syndrome: a case report [J]. Journal of Internal Medicine Concepts & Practice, 2024, 19(05): 318-321. |
| [3] | PAN Meng, WANG Jingying. Current status and considerations on the diagnosis and treatment of pemphigus in China [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(03): 209-214. |
| [4] | WANG Yan, TAO Yi, JIN Shiwei, MI Jianqing, LIU Yuanfang. Dose-adjusted daratumumab combined with DCEP in treatment of multiple myeloma dual-refractory to bortezomib and lenalidomide [J]. Journal of Internal Medicine Concepts & Practice, 2023, 18(03): 165-170. |
| [5] | . [J]. Journal of Diagnostics Concepts & Practice, 2012, 11(02): 130-135. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||