外科理论与实践 ›› 2023, Vol. 28 ›› Issue (04): 371-377.doi: 10.16139/j.1007-9610.2023.04.014
朱巧俐1, 苗伊鸣2*, 陈小松2( )
)
收稿日期:2022-08-24
出版日期:2023-07-25
发布日期:2023-10-24
通讯作者:
陈小松,E-mail: 作者简介:*共同第一作者
ZHU Qiaoli1, MIAO Yiming2*, CHEN Xiaosong2()
Received:2022-08-24
Online:2023-07-25
Published:2023-10-24
摘要:
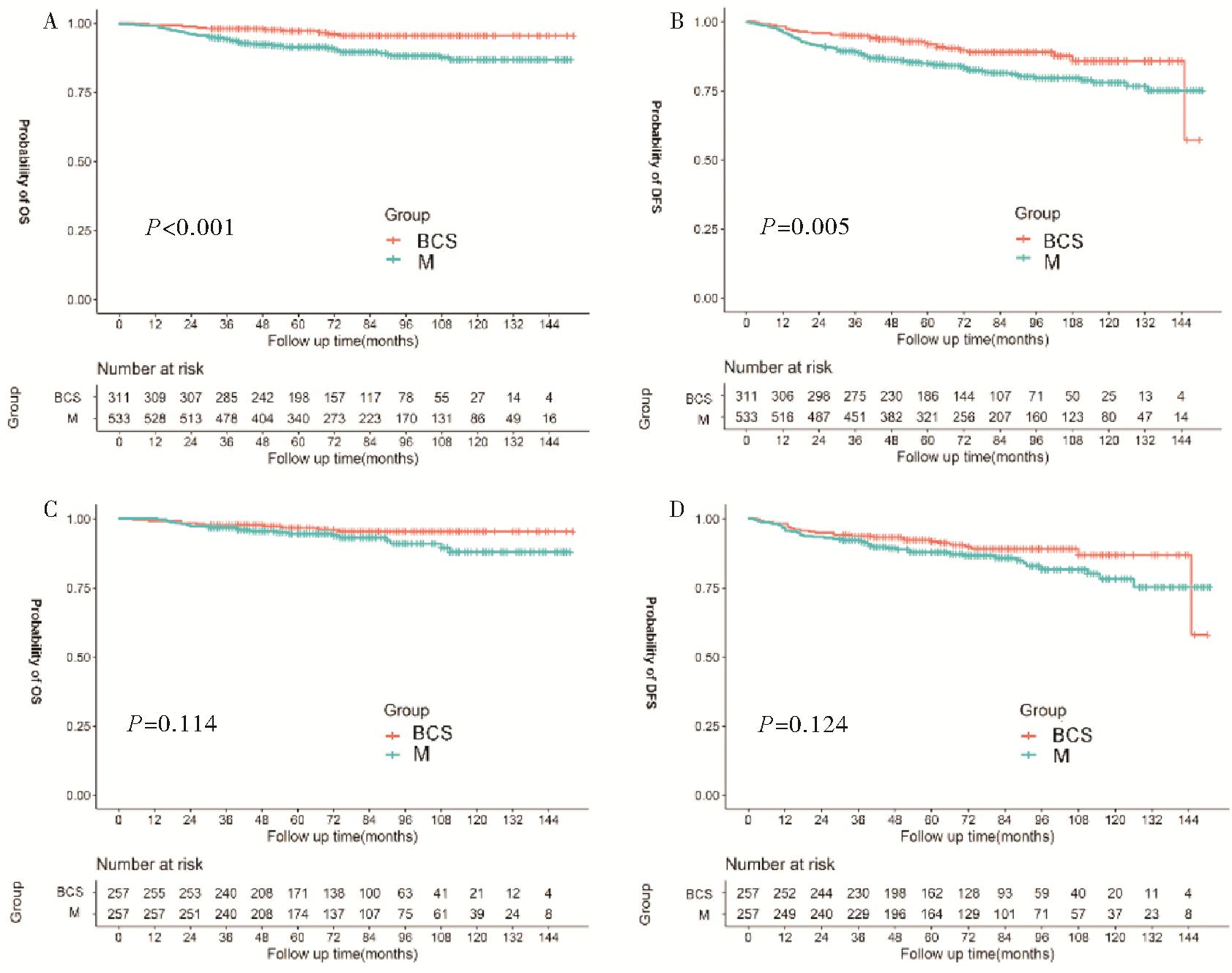
目的:探讨Ⅰ~Ⅲ期三阴性乳腺癌(triple-negative breast cancer, TNBC)病人接受保乳手术(breast-conserving surgery, BCS)或乳房切除术(mastectomy, M)对病人无病生存(disease free survival, DFS)和总生存(overall survival, OS)的影响。方法:收集2009年1月至2018年12月上海交通大学医学院附属瑞金医院乳腺疾病诊治中心收治的844例可手术Ⅰ~Ⅲ期TNBC病人,根据手术方式分为BCS组和M组。采用COX回归分析评估病人的临床特征和手术方式对病人DFS和OS的影响。进一步应用倾向性评分匹配平衡两组病人间存在的基线特征差异,评估两组手术的预后差异。结果:533例(63.15%)接受M,311例(36.85%)接受BCS。与M组相比,年轻、肿瘤小、淋巴结阴性、HER2表达缺失(HER2-0)的病人更多接受BCS。中位随访时间72个月。多因素分析表明,M组病人的OS率低于BCS组病人(HR=2.02,95% CI: 1.04~3.91,P=0.038),但两组DFS差异无统计学意义(HR=1.42,95% CI: 0.94~2.15, P=0.100)。将病人T分期、N分期(pN)和年龄等因素进行倾向性评分匹配平衡后,BCS组和M组病人OS率(P=0.114)和DFS率(P=0.124)差异无统计学意义。结论:在Ⅰ~Ⅲ期TNBC病人中,年轻、肿瘤小、淋巴结阴性和HER2-0病人更多选择BCS。匹配相关临床病理指标后,TNBC病人接受BCS或M手术方式的预后差异无统计学意义。
中图分类号:
朱巧俐, 苗伊鸣, 陈小松. I~III期三阴性乳腺癌病人接受保乳手术或乳房切除术的预后分析[J]. 外科理论与实践, 2023, 28(04): 371-377.
ZHU Qiaoli, MIAO Yiming, CHEN Xiaosong. Prognostic analysis of breast-conserving surgery or mastectomy in patients with stage Ⅰ-Ⅲ triple-negative breast cancer[J]. Journal of Surgery Concepts & Practice, 2023, 28(04): 371-377.
表1
Ⅰ~Ⅲ期TNBC病人临床病理特征分析[$\bar{x}±s$/n(%)]
| Factors | BCS(n=311) | M(n=533) | F/x2 value | P value |
|---|---|---|---|---|
| Age(years) | 53.68±13.05 | 57.23±11.85 | 16.3 | <0.001 |
| BMI(kg/m2) | 23.10±3.01 | 23.01±2.79 | 0.2 | 0.671 |
| Menopause status[n(%)] | ||||
| Pre-menopause | 128 (41.16) | 167 (31.33) | 8.3 | 0.004 |
| Post-menopause | 183 (58.84) | 366 (68.67) | ||
| pT[n(%)] | ||||
| T1 | 192 (61.74) | 226 (42.40) | 29.4 | <0.001 |
| T2-3 | 119 (38.26) | 307 (57.60) | ||
| pN[n(%)] | ||||
| Negative | 250 (80.39) | 358 (67.17) | 17.0 | <0.001 |
| Positive | 61 (19.61) | 175 (32.83) | ||
| HER2[n(%)] | ||||
| HER2-0 | 135 (43.41) | 182 (34.15) | 7.2 | 0.007 |
| HER2 low | 176 (56.59) | 351 (65.85) | ||
| Ki-67[n(%)] | ||||
| ≤14% | 42 (13.50) | 90 (16.89) | 1.7 | 0.192 |
| >14% | 269 (86.50) | 443 (83.11) | ||
| Pathologic typing[n(%)] | ||||
| DCIS | 5 (1.61) | 11 (2.07) | ||
| IDC | 290 (93.25) | 490 (91.93) | 0.5 | 0.776 |
| Others[n(%)] | 16 (5.14) | 32 (6.00) | ||
| Grading | ||||
| Ⅰ-Ⅱ | 59 (18.97) | 129 (24.20) | ||
| Ⅲ | 200 (64.31) | 322 (60.41) | 3.1 | 0.211 |
| Unknown | 52 (16.72) | 82 (15.39) | ||
| Chemotherapy[n(%)] | ||||
| No | 41 (13.18) | 63 (11.82) | 0.3 | 0.561 |
| Yes | 270 (86.82) | 470 (88.18) |
表2
Ⅰ~Ⅲ期TNBC病人M组相关临床病理因素的多因素Logistic回归分析
| Factors | OR | 95%CI | P value |
|---|---|---|---|
| Age(years) ≥60 vs. <60 | 1.02 | 1.01-1.04 | 0.013 |
| Menopause status post-menopause vs. pre-menopause | 0.99 | 0.63-1.57 | 0.967 |
| pT T2-3 vs. T1 | 2.17 | 1.61-2.91 | <0.001 |
| pN N positive vs. N negative | 1.84 | 1.30-2.59 | <0.001 |
| HER2 HER2 low vs. HER2-0 | 1.42 | 1.05-1.92 | 0.023 |
表3
Ⅰ~Ⅲ期TNBC病人OS及DFS的单因素COX回归分析
| Factors | OS | DFS |
|---|---|---|
| P value | P value | |
| Age(years) ≥60 vs. <60 | 0.07 | 0.158 |
| Menopause status post-menopause vs. pre-menopause | 0.09 | 0.061 |
| BMI(kg/m2) | 0.773 | 0.605 |
| ≥24 vs. ≥18.5,<24 | 0.473 | 0.698 |
| <18.5 vs. ≥18.5,<24 | 0.967 | 0.375 |
| Pathologic typing | 0.589 | 0.507 |
| IDC vs. DCIS | 0.78 | 0.725 |
| Others vs. DCIS | 0.723 | 0.333 |
| pT T2-3 vs. T1 | 0.001 | <0.001 |
| pN N positive vs. N negative | <0.001 | <0.001 |
| Grading | 0.291 | 0.733 |
| Ⅲ vs. Ⅰ-Ⅱ | 0.981 | 0.566 |
| Unknown vs. Ⅰ-Ⅱ | 0.156 | 0.897 |
| HER2 HER2 low vs. HER2-0 | 0.362 | 0.749 |
| Ki-67 >14% vs. ≤14% | 0.119 | 0.045 |
| Chemotherapy Yes vs. No | 0.112 | 0.049 |
| Surgical approach M vs. BCS | 0.002 | 0.005 |
表4
Ⅰ~Ⅲ期TNBC病人OS及DFS的多因素COX回归分析
| Factors | OS | DFS | |||||
|---|---|---|---|---|---|---|---|
| HR | 95% CI | P value | HR | 95%CI | P value | ||
| Age(years) ≥60 vs. <60 | 1.37 | 0.64-2.91 | 0.419 | / | / | / | |
| Menopause status Post-menopause vs. pre-menopause | 1.23 | 0.53-2.84 | 0.626 | 1.33 | 0.9-1.97 | 0.155 | |
| Surgical approach M vs. BCS | 2.02 | 1.04-3.91 | 0.038 | 1.42 | 0.94-2.15 | 0.100 | |
| pT T2-3 vs. T1 | 2.02 | 1.17-3.48 | 0.011 | 1.82 | 1.25-2.65 | 0.002 | |
| Chemotherapy Yes vs. No | / | / | / | 0.58 | 0.35-0.94 | 0.026 | |
| pN N Positive vs. N Negative | 3.22 | 1.96-5.30 | <0.001 | 2.12 | 1.48-3.05 | 0.001 | |
| Ki-67 >14% vs. ≤14% | / | / | / | 0.67 | 0.44-1.04 | 0.076 | |
表5
PSM后行BCS及M的Ⅰ~Ⅲ期TNBC病人临床病理特征比较[$\bar{x}±s$/n(%)]
| Factors | BCS (n=257) | M (n=257) | F/x2 value | P value |
|---|---|---|---|---|
| Age(years) | 54.79±12.76) | 56.02±11.67) | 1.3 | 0.253 |
| BMI(kg/m2) | 23.11±3.00) | 23.14±2.82) | 0.0 | 0.912 |
| Menopause status[n(%)] | ||||
| Pre-menopause | 100 (38.91) | 87 (33.85) | 1.4 | 0.233 |
| Post-menopause | 157 (61.09) | 170 (66.15) | ||
| pT[n(%)] | ||||
| T1 | 148 (57.59) | 145 (56.42) | 0.7 | 0.789 |
| T2-3 | 109 (42.41) | 112 (43.58) | ||
| pN[n(%)] | ||||
| Negative | 202 (78.60) | 208 (80.93) | 0.4 | 0.51 |
| Positive | 55 (21.40) | 49 (19.07) | ||
| HER2[n(%)] | ||||
| HER2 0 | 103 (40.08) | 107 (41.63) | 0.1 | 0.72 |
| HER2 low | 154 (59.92) | 150 (58.37) | ||
| Ki-67[n(%)] | ||||
| ≤14% | 34 (13.23) | 42 (16.34) | 1.0 | 0.32 |
| >14% | 223 (86.77) | 215 (83.66) | ||
| Pathologic typing[n(%)] | ||||
| DCIS | 5 (1.95) | 6 (2.34) | 0.3 | 0.854 |
| IDC | 242 (94.16) | 243 (94.55) | ||
| Others | 10 (3.89) | 8 (3.11) | ||
| Grading[n(%)] | ||||
| Ⅰ-Ⅱ | 52 (20.23) | 47 (18.29) | 1.3 | 0.528 |
| Ⅲ | 168 (65.37) | 164 (63.81) | ||
| Unknown | 37 (14.40) | 46 (17.90) | ||
| Chemotherapy[n(%)] | ||||
| No | 30 (11.67) | 39 (15.18) | 1.4 | 0.244 |
| Yes | 227 (88.33%) | 218 (84.82%) |
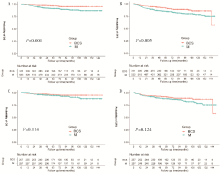
图1
倾向性评分匹配前后接受BCS或M的生存分析
| [1] |
SUNG H, FERLAY J, SIEGEL R L, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3):209-249.
doi: 10.3322/caac.v71.3 URL |
| [2] | DASS S A, TAN K L, SELVA RAJAN R, et al. Triple negative breast cancer: a review of present and future diagnostic modalities[J]. Medicina(kaunas), 2021, 57(1):62. |
| [3] | LI Y, MU L, RUAN Y X, et al. The influence of molecular classification of breast cancer on the safety of breast-conserving surgery[J]. Zhonghua Zhong Liu Za Zhi, 2018, 40(5):341-346. |
| [4] | 陈春明, 孔灵芝. 中国成人超重和肥胖症预防控制指南[M]. 北京: 人民卫生出版社, 2006:3. |
| CHEN C M, KONG L Z. Guidelines for the prevention and control of overweihgt and obesity in Chinese adults[M]. Beijing: People’s Medical Publishing House, 2006:3. | |
| [5] | AMIN M B, EDGE S B, GREENE F L, et al. AJCC cancer staging manual. 8th ed[M]. NewYork: Springer, 2016:589-628. |
| [6] |
GU J, GROOT G, BODEN C, et al. Review of factors influencing women's choice of mastectomy versus breast conserving therapy in early stage breast cancer: a syste-matic review[J]. Clin Breast Cancer, 2018, 18(4):e539-e554.
doi: 10.1016/j.clbc.2017.12.013 URL |
| [7] |
BOERO I J, PARAVATI A J, HOU J, et al. The impact of surgeons on the likelihood of mastectomy in breast cancer[J]. Ann Surg, 2019, 269:951-958.
doi: 10.1097/SLA.0000000000002698 pmid: 29465454 |
| [8] |
CHEN Q X, WANG X X, LIN P Y, et al. The different outcomes between breast-conserving surgery and mastectomy in triple-negative breast cancer: a population-based study from the SEER 18 database[J]. Oncotarget, 2017, 8(3):4773-4780.
doi: 10.18632/oncotarget.v8i3 URL |
| [9] |
LI P, LI L, XIU B, et al. The prognoses of young women with breast cancer (≤35 years) with different surgical options: a propensity score matching retrospective cohort study[J]. Front Oncol, 2022, 12:795023.
doi: 10.3389/fonc.2022.795023 URL |
| [10] |
FISHER B, ANDERSON S, BRYANT J, et al. Twenty-year follow-up of a randomized trial comparing total mastectomy, lumpectomy, and lumpectomy plus irradiation for the treatment of invasive breast cancer[J]. N Engl J Med, 2002, 347(16):1233-1241.
doi: 10.1056/NEJMoa022152 URL |
| [11] |
SINNADURAI S, KWONG A, HARTMAN M, et al. Breast-conserving surgery versus mastectomy in young women with breast cancer in Asian settings[J]. BJS Open, 2018, 3(1):48-55.
doi: 10.1002/bjs5.2019.3.issue-1 URL |
| [12] |
AGARWAL S, PAPPAS L, NEUMAYER L, et al. Effect of breast conservation therapy vs. mastectomy on disease-specific survival for early-stage breast cancer[J]. JAMA Surg, 2014, 149(3):267-274.
doi: 10.1001/jamasurg.2013.3049 URL |
| [13] |
HARTMANN-JOHNSEN O J, KÅRESEN R, SCHLICHTING E, et al. Survival is better after breast conserving therapy than mastectomy for early stage breast cancer: a registry-based follow-up study of Norwegian women primary ope-rated between 1998 and 2008[J]. Ann Surg Oncol, 2015, 22(12):3836-3845.
doi: 10.1245/s10434-015-4441-3 URL |
| [14] |
WANG J, YANG S P, ZHOU P, et al. Additional radiotherapy to breast-conserving surgery is an optional treatment for de novo stage Ⅳ breast cancer: a population-based analysis[J]. Cancer Med, 2021, 10(5):1634-1643.
doi: 10.1002/cam4.v10.5 URL |
| [15] |
WANG J, WANG S, TANG Y, et al. Comparison of treatment outcomes with breast-conserving surgery plus radiotherapy versus mastectomy for patients with stage Ⅰ breast cancer: a propensity score-matched analysis[J]. Clin Breast Cancer, 2018, 18(5):e975-e984.
doi: 10.1016/j.clbc.2018.06.002 URL |
| [16] |
DE LA CRUZ KU G, KARAMCHANDANI M, CHAMBERGO-MICHILOT D, et al. Does breast-conserving surgery with radiotherapy have a better survival than mastectomy? A meta-analysis of more than 1,500,000 patients[J]. Ann Surg Oncol, 2022, 29(10):6163-6188.
doi: 10.1245/s10434-022-12133-8 |
| [17] |
VAN MAAREN M C, DE MUNCK L, DE BOCK G H, et al. 10 year survival after breast-conserving surgery plus radiotherapy compared with mastectomy in early breast cancer in the Netherlands: a population-based study[J]. Lancet Oncol, 2016, 17(8):1158-1170.
doi: S1470-2045(16)30067-5 pmid: 27344114 |
| [18] | 刘晓静, 杨柳春, 进淑娟, 等. 乳腺癌患者生存与复发的随访报告:一项单中心回顾性研究[J]. 中华乳腺病杂志(电子版), 2019, 13(5):270-276. |
| LIU X J, YANG L C, JIN S J, et al. Survival and recurrence of breast cancer patients:a single-center retrospective study[J]. Chin J Breast Dis(Electronic Edition), 2019, 13(5):270-276. | |
| [19] | 刘晓静, 朱明华, 左思, 等. 不同治疗方式对三阴性乳腺癌预后的影响[J]. 国际肿瘤学杂志, 2022, 49(1):33-38. |
|
LIU X J, ZHU M H, ZUO S, et al. Effects of different treatments on prognosis of triple-negative breast cancer[J]. J Int Oncol, 2022, 49(1):33-38.
doi: 10.3892/ijo.2016.3516 URL |
|
| [20] | 吕文芝, 丁波泥, 钱立元, 等. 保留乳房手术对比乳房根治术治疗三阴性乳腺癌疗效的Meta分析[J]. 中华乳腺病杂志(电子版), 2018, 12(5):276-281. |
| LYU W Z, DING B N, QIAN L Y, et al. Efficacy comparison of breast conserving surgery versus radical mastectomy in triple negative breast cancer patients:a meta-analysis[J]. Chin J Breast Dis(Electronic Edition), 2018, 12(5):276-281. | |
| [21] | DOMINICI L S, HU J, KING T A, et al. Abstract GS6-06: local therapy and quality of life outcomes in young women with breast cancer[J]. Cancer Research, 2019, 79(4 Supplement):GS6-06-GS6-06. |
| [1] | 李慧, 尹昱, 李春晓, 等. 呼吸训练对乳腺癌相关淋巴水肿康复疗效的研究进展#br#[J]. 组织工程与重建外科杂志, 2023, 19(4): 430-. |
| [2] | 张莹莹, 李华, 管佳琴, 等.
乳腺癌患者术后早期上肢淋巴水肿的发生率及影响因素分析
[J]. 组织工程与重建外科杂志, 2023, 19(3): 242-. |
| [3] | 朱丹丽 鲍婉婷 魏昊 郭善禹.
乳腺癌术后乳房缺损修复的研究进展
[J]. 组织工程与重建外科杂志, 2023, 19(2): 201-. |
| [4] | 杨奕, 杨兴霞, 金思励, 张旭, 朱娟英, 陈小松. 术前MRI检查在乳腺导管原位癌保乳手术的临床应用研究[J]. 外科理论与实践, 2023, 28(04): 378-382. |
| [5] | 董军, 崔凤鸣, 刘军. 沉默Ki-67基因对乳腺癌MCF-7/DOX细胞多柔比星耐药性的影响[J]. 外科理论与实践, 2023, 28(03): 254-259. |
| [6] | 高卫奇, 张旭, 王铮, 朱一霏, 黄佳慧, 洪进, 朱思吉, 陈小松, 黄欧, 何建蓉, 陈伟国, 李亚芬, 沈坤炜, 徐华, 吴佳毅. 新辅助治疗后腹壁下深血管穿支皮瓣即刻乳房重建手术的安全性研究[J]. 外科理论与实践, 2023, 28(02): 147-151. |
| [7] | 张小丽 李赞 宋达疆 王业成 海涛. 带蒂胸外侧动脉穿支皮瓣在保乳术后即刻乳房重建中的临床应用[J]. 组织工程与重建外科杂志, 2022, 18(5): 382-. |
| [8] | 宋达疆 李赞 章一新. 带蒂腹直肌皮瓣联合游离腹壁下动脉穿支皮瓣移植重建胸壁巨大缺损的手术策略[J]. 组织工程与重建外科杂志, 2022, 18(5): 386-. |
| [9] | 姚成才 陈明 刘长春 黄传蔷 冼家仪 严国标 陈庞洲. 硅凝胶乳房假体联合钛网补片在早期乳腺癌即刻乳房重建中的应用[J]. 组织工程与重建外科杂志, 2022, 18(3): 247-. |
| [10] | 廖晓明 蒋奕 唐玮 杨华伟 姬逸男 韦莉颖. 薄层血管化腹股沟淋巴结皮瓣移植联合反向淋巴显影在继发性上肢淋巴水肿手术中的应用[J]. 组织工程与重建外科杂志, 2022, 18(1): 8-. |
| [11] | 宋景涌 汤鹏 钟晓捷 刘侠 孙洋 亢玉 王遥佳 陈安玥 陈怡安 吉训通 周艳虹 蒋曼妃 修骋 穆籣. 吻合口通畅性量化分析应用于乳腺癌腋窝淋巴结清扫术同期预防性淋巴管静脉吻合1例[J]. 组织工程与重建外科杂志, 2022, 18(1): 34-. |
| [12] | 陈小松, 沈坤炜, 李宏为. 早期可手术乳腺癌的诊治现状与展望[J]. 外科理论与实践, 2022, 27(05): 385-386. |
| [13] | 吴佳毅, 陆裕杰, 何金光, 沈坤炜, 徐华. 乳腺癌术后植入物乳房重建技术[J]. 外科理论与实践, 2022, 27(05): 387-391. |
| [14] | 陈益定, 吴世杰. 遗传性乳腺癌外科治疗[J]. 外科理论与实践, 2022, 27(05): 392-395. |
| [15] | 谢妍妍, 吕青, 杜正贵. 乳腺腔镜和机器人手术的现状及未来之路——华西医院经验分享[J]. 外科理论与实践, 2022, 27(05): 396-402. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||