外科理论与实践 ›› 2021, Vol. 26 ›› Issue (05): 420-424.doi: 10.16139/j.1007-9610.2021.05.012
周静瑜, 任峰, 周建平( )
)
收稿日期:2021-08-03
出版日期:2021-09-25
发布日期:2022-07-22
通讯作者:
周建平
E-mail:392991429@qq.com
ZHOU Jingyu, REN Feng, ZHOU Jianping()
Received:2021-08-03
Online:2021-09-25
Published:2022-07-22
Contact:
ZHOU Jianping
E-mail:392991429@qq.com
摘要: 目的:探讨开放人工材料桥接修复手术治疗腹壁巨大缺损的应用。方法:回顾性分析2007年6月至2020年6月我科收治的58例腹壁巨大缺损病人临床资料,其中19例腹壁占位性病变切除后缺损,35例巨大切口疝,3例腹壁外伤、感染后肌层毁损,1例先天性膈疝修补后腹腔容积不足延迟关腹,随访观察疗效。结果:本研究所有病人均达到预期重建效果。术后发生血清肿5例,通过重置双套管负压抽吸治愈。皮肤坏死、切口裂开、补片外露1例,用负压封闭引流(vacuum sealing drainage,VSD)技术引流愈合。血肿1例,加压包扎保守治疗。补片感染1例,取出上层补片,应用VSD技术引流愈合。1例腹腔容积不足采用腹腔内修补(intraperitoneal onlay mesh,IPOM)+Inlay桥接、补片外露的临时性关腹,通过3次VSD分期拉拢、关闭皮肤伤口。1例补片膨出,持续随访,未行特殊处理。随访12~156个月,3例失访,随访率为94.8%,未见疝或缺损复发。结论:对于肌筋膜层无法关闭的腹壁巨大缺损,开放人工材料桥接修补手术是腹壁外科不可或缺的一项技术,并发症可以防控。
中图分类号:
周静瑜, 任峰, 周建平. 开放人工材料桥接修复腹壁巨大缺损(附58例报告)[J]. 外科理论与实践, 2021, 26(05): 420-424.
ZHOU Jingyu, REN Feng, ZHOU Jianping. Open bridging repair with artificial material in treating large abdominal wall defect: a report of 58 cases[J]. Journal of Surgery Concepts & Practice, 2021, 26(05): 420-424.
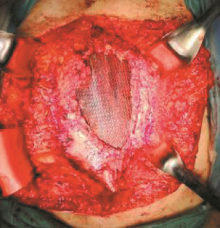
图1
IPOM桥接


图2
Sublay桥接
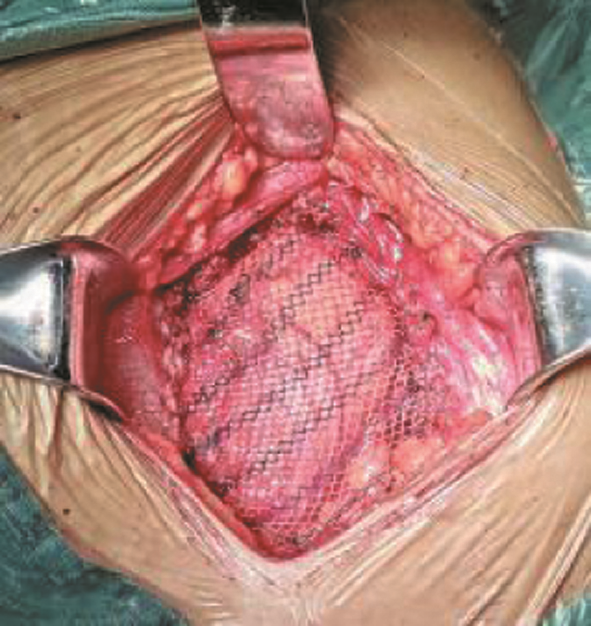
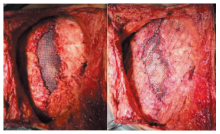
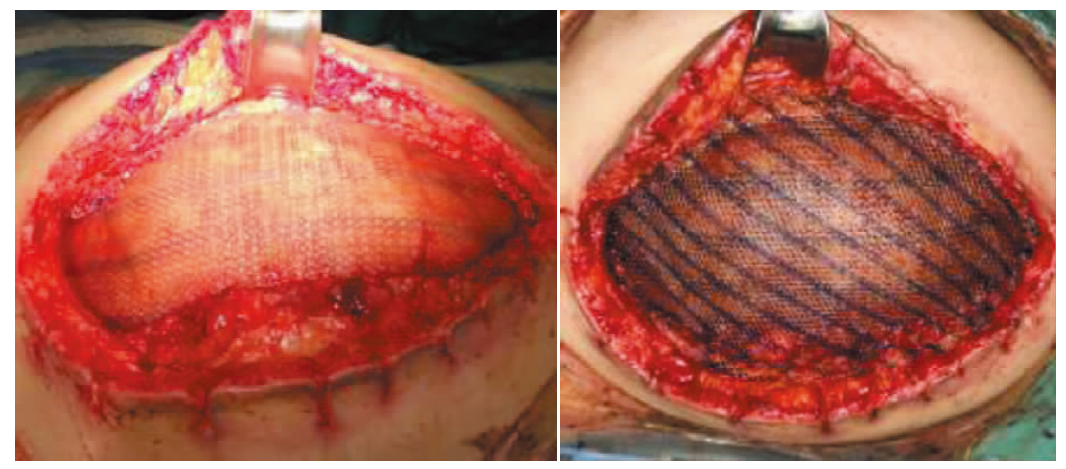
图3
IPOM+Onlay桥接
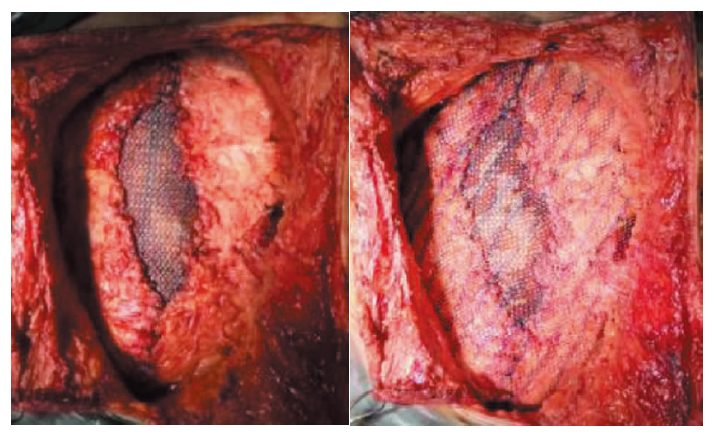
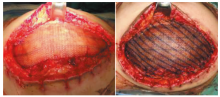
图4
IPOM+Inlay桥接
| [1] | 中华医学会外科学分会疝与腹壁外科学组, 中国医疗保健国际交流促进会临床实用技术分会腹壁修复与重建外科学组.组织结构分离技术规范化操作中国专家共识(2020版)[J]. 中国实用外科杂志, 2020, 40(5):488-493. |
| [2] | 中华医学会外科学分会疝与腹壁外科学组, 中国医疗保健国际交流促进会临床实用技术分会腹壁修复与重建外科学组. 腹壁缺损修复与重建中国专家共识(2019 版)[J]. 中国实用外科杂志, 2019, 39(2):101-109. |
| [3] |
Bernardi K, Olavarria OA, Holihan JL, et al. Primary fascial closure during laparoscopic ventral hernia repair improves patient quality of life: a multicenter, blinded randomized controlled trial[J]. Ann Surg, 2020, 271(3):434-439.
doi: 10.1097/SLA.0000000000003505 pmid: 31365365 |
| [4] |
Sharma A, Sinha C, Baijal M, et al. Hybrid approach for ventral incisional hernias of the abdominal wall: a systematic review of the literature[J]. J Minim Access Surg, 2021, 17(1):7-13.
doi: 10.4103/jmas.JMAS_146_19 URL |
| [5] |
Bittner R, Bain K, Bansal VK, et al. Update of Guidelines for laparoscopic treatment of ventral and incisional abdominal wall hernias (International Endohernia Society (IEHS))—Part A[J]. Surg Endosc, 2019, 33(10):3069-3139.
doi: 10.1007/s00464-019-06907-7 pmid: 31250243 |
| [6] | 周建平, 任峰, 周静瑜. 腹壁外科桥接手术常见并发症的预防和处理[J]. 中国实用外科杂志, 2020, 40(7):24-26. |
| [7] |
Massey LH, Pathak S, Bhargava A, et al. The use of adjuncts to reduce seroma in open incisional hernia repair: a systematic review[J]. Hernia, 2018, 22(2):273-283.
doi: 10.1007/s10029-017-1690-z pmid: 29071497 |
| [8] |
Petersson P, Montgomery A, Petersson U, et al. Vacuum-assisted wound closure and permanent onlay mesh-me-diated fascial traction: a novel technique for the prevention of incisional hernia after open abdomen therapy inclu-ding results from a retrospective case series[J]. Scand J Surg, 2019, 108(3):216-226.
doi: 10.1177/1457496918818979 pmid: 30574843 |
| [9] |
Garcia-Ruano A, Deleyto E, Garcia-Fernandez S. VAC-instillation therapy in abdominal mesh exposure: a novel indication[J]. J Surg Res, 2016, 206(2):292-297.
doi: S0022-4804(16)30298-0 pmid: 27884322 |
| [10] |
Kokotovic D, Bisgaard T, Helgstrand F. Long-term recurrence and complications associated with elective incisional hernia repair[J]. JAMA, 2016, 316(15):1575-1582.
doi: 10.1001/jama.2016.15217 pmid: 27750295 |
| [1] | 徐康倪 袁斯明.
婴幼儿血管瘤的局部医源性并发症
[J]. 组织工程与重建外科杂志, 2023, 19(2): 146-. |
| [2] | 叶枫, 龚笑勇, 任家俊, 蔡强, 陈胜. ERCP在原发性肝癌围术期胆道并发症诊治中的应用[J]. 外科理论与实践, 2023, 28(04): 355-360. |
| [3] | 华晴, 周建桥. 甲状腺良性结节超声引导下热消融并发症研究进展[J]. 诊断学理论与实践, 2023, 22(02): 184-189. |
| [4] | 于岚, 张永怡, 黄雷, 万歆, 姜胜耀, 唐思静, 张俊, 胡伟国. 老年病人胰十二指肠切除术后严重并发症发生的危险因素[J]. 外科理论与实践, 2023, 28(02): 139-146. |
| [5] | 何凯, 唐颖, 周秀玲, 朱俞岚, 傅晓键, 朱炎逢, 丁红, 姚琪远, 陈浩. 腔镜腹白线折叠缝合术治疗产伤性腹直肌分离的临床疗效评估[J]. 外科理论与实践, 2023, 28(01): 67-71. |
| [6] | 李建锋 李强 黄欢 张希峰 严建锋 蔡莉丹. 高龄患者髋关节置换的ERAS路径与传统路径的临床疗效对比[J]. 组织工程与重建外科杂志, 2022, 18(2): 154-. |
| [7] | 庄奥博, 童汉兴, 张勇, 陆维祺, 周宇红, 闾晨涛. 老年原发性腹膜后软组织肉瘤病人手术治疗安全性分析的回顾性队列研究[J]. 外科理论与实践, 2022, 27(06): 534-539. |
| [8] | 黄蔚, 李恒宇, 丁晓毅. 晚期乳腺癌介入诊疗的价值及应用[J]. 外科理论与实践, 2022, 27(05): 411-415. |
| [9] | 王瑞华, 仇鹏, 刘俊超, 吴小雨, 秦金保, 叶开创, 李维敏, 刘晓兵, 殷敏毅, 黄新天, 陆信武. 激光原位开窗胸主动脉腔内重建治疗累及弓部分支的主动脉夹层:近期结果及并发症[J]. 外科理论与实践, 2022, 27(04): 324-329. |
| [10] | 杜燕然, 焦景, 任芸芸, 周建桥. 超声影像组学技术在评估胎肺成熟度中的应用[J]. 诊断学理论与实践, 2022, 21(03): 326-330. |
| [11] | 王巍, 华杰. 胰十二指肠切除术中常见血管变异及应对策略[J]. 外科理论与实践, 2022, 27(01): 34-38. |
| [12] | 林喜风 卢艺朴 王涛. 微创钥匙孔负压抽吸术治疗腋臭疗效观察及术后并发症影响因素分析[J]. 组织工程与重建外科杂志, 2021, 17(4): 335-. |
| [13] | 李艳 李萍 殷宗宝 陈晓峰 薛小云 张烨. 急性髋关节骨折患者手术时机的选择[J]. 组织工程与重建外科杂志, 2021, 17(4): 345-. |
| [14] | 张少杰 韩森东. 伊利扎罗夫技术治疗 Pilon 骨折的临床效果观察 [J]. 组织工程与重建外科杂志, 2021, 17(2): 142-. |
| [15] | 孙寒星, 沈晓卉, 高浩基, 刘卓然, 陈曦, 邱伟华, 严佶祺. Graves病的手术前评估与准备(附126例报告)[J]. 外科理论与实践, 2021, 26(06): 517-521. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||