外科理论与实践 ›› 2021, Vol. 26 ›› Issue (02): 138-143.doi: 10.16139/j.1007-9610.2021.02.010
司安锋1a, 雷正清2, 杨平华3, 江涛1b, 王轩1b, 程张军2( )
)
收稿日期:2021-01-21
出版日期:2021-03-25
发布日期:2022-07-27
通讯作者:
程张军
E-mail:chengzhangjun@seu.edu.cn
SI Anfeng1a, LEI Zhengqing2, YANG Pinghua3, JIANG Tao1b, WANG Xuan1b, CHENG Zhangjun2()
Received:2021-01-21
Online:2021-03-25
Published:2022-07-27
Contact:
CHENG Zhangjun
E-mail:chengzhangjun@seu.edu.cn
摘要:
目的:探讨巨块型肝内胆管癌术后经肝动脉化疗栓塞(transarterial chemoembolization,TACE)治疗的有效性。方法:回顾性分析2009年1月至2013年12月手术治疗125例巨块型肝内胆管癌(最大径≥10 cm)病人的临床病理资料。35例术后TACE,90例无术后TACE,分别为TACE组和非TACE组。采用Kaplan-Meier法估计病人术后复发率和生存率。采用Log-Rank检验比较组间差异。应用Cox回归探索影响病人术后复发和生存的独立危险因素。采用倾向评分匹配减少组间差异。根据肝内胆管癌第8版TNM分期进行亚组分析,探索术后TACE治疗的获益病人。结果:TACE组和非TACE组具有相似的复发率和生存率(5年复发率:85.7%比84.4%,P=0.487;5年生存率:22.9%比20.0%,P=0.426)。1∶1倾向评分配对后,两组各33例病人,术后复发率(P=0.114)和生存率(P=0.197)差异无统计学意义。TNM分期亚组分析,61例TNM Ⅰ期,64例TNM Ⅱ期。分期分析显示Ⅰ期病人TACE组和非TACE组的复发率和生存率差异无统计学意义。Ⅱ期病人TACE组5年复发率较低(91.7%比97.5%,P=0.022),5年生存率较高(12.5%比2.5%,P=0.002)。在矫正肿瘤多发、血管侵犯和癌胚抗原≥5 μg/L后,TACE仍是显著影响Ⅱ期病人肿瘤复发(风险比:0.564,95% CI:0.327~0.974)和生存(风险比:0.449,95% CI:0.259~0.777)的危险因素。结论:术后TACE有可能改善巨块型肝内胆管癌TNM Ⅱ期病人的预后。
中图分类号:
司安锋, 雷正清, 杨平华, 江涛, 王轩, 程张军. 巨块型肝内胆管癌术后经肝动脉化疗栓塞的有效性[J]. 外科理论与实践, 2021, 26(02): 138-143.
SI Anfeng, LEI Zhengqing, YANG Pinghua, JIANG Tao, WANG Xuan, CHENG Zhangjun. Effectiveness of postoperative transarterial chemoembolization for huge intrahepatic cholangiocarcinoma[J]. Journal of Surgery Concepts & Practice, 2021, 26(02): 138-143.
表1
两组临床病理特征[n(%)]
| 变量 | TACE组 (n=35) | 非TACE组 (n=90) | P值 |
|---|---|---|---|
| 年龄(岁) | 54 (47~64) | 55 (46~62) | 0.835 |
| 男性 | 21 (60.0) | 52 (57.8) | 0.821 |
| 有结石 | 5 (14.3) | 18 (20.0) | 0.459 |
| 乙肝表面抗原阳性 | 17 (48.6) | 38 (42.2) | 0.521 |
| 甲胎蛋白≥20 μg/L | 11 (31.4) | 18 (20.0) | 0.174 |
| 糖类抗原19-9≥39 U/L | 15 (42.9) | 45 (50.0) | 0.473 |
| 癌胚抗原≥5 μg/L | 5 (14.3) | 25 (27.8) | 0.113 |
| 总胆红素≥17.1 μmol/L | 3 (8.6) | 17 (18.9) | 0.254 |
| 丙氨酸转氨酶≥44 U/L | 6 (17.1) | 13 (14.4) | 0.706 |
| 碱性磷酸酶≥129 U/L | 10 (28.6) | 34 (37.8) | 0.333 |
| 肿瘤直径(cm) | 11.1 (10.4~13.3) | 11.7 (10.4~13.0) | 0.839 |
| 肿瘤数目 | |||
| 多发 | 17 (48.6) | 34 (37.8) | 0.270 |
| 单发 | 18 (51.4) | 56 (62.2) | |
| 肝硬化 | 9 (25.7) | 20 (22.2) | 0.678 |
| 术中输血 | 14 (40.0) | 26 (28.9) | 0.232 |
| 分化差 | 2 (5.7) | 5 (5.6) | 1.000 |
| 血管侵犯 | 11 (31.4) | 14 (15.6) | 0.046 |
| TNM分期 | |||
| Ⅰ: T1bN0M0 | 11 (31.4) | 50 (55.6) | 0.015 |
| Ⅱ: T2N0M0 | 24 (68.6) | 40 (44.4) |
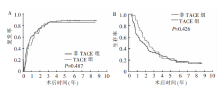
图1
两组预后比较 A:复发曲线;B:生存曲线
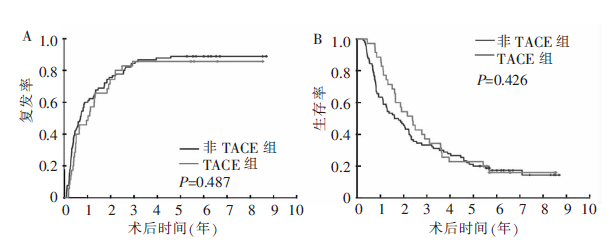
表2
术后生存的单因素、多因素Cox回归分析
| 变量 | 单因素 | 多因素 | |||
|---|---|---|---|---|---|
| 风险比(95% CI) | P值 | 风险比(95% CI) | P值 | ||
| 年龄(岁)55>比≤55 | 0.950 (0.646~1.397) | 0.794 | |||
| 男比女 | 0.973 (0.659~1.439) | 0.893 | |||
| 结石 | 1.023 (0.628~1.667) | 0.927 | |||
| 乙肝表面抗原阳性 | 1.053 (0.714~1.552) | 0.795 | |||
| 甲胎蛋白(μg/L)>20比≤20 | 1.297 (0.835~2.013) | 0.247 | |||
| 糖类抗原19-9(U/L)>39比≤39 | 1.372 (0.931~2.022) | 0.110 | |||
| 癌胚抗原(μg/L)>5比≤5 | 2.346 (1.518~3.627) | <0.001 | 1.804 (1.142~2.850) | 0.011 | |
| 总胆红素(μmol/L)>17.1比≤17.1 | 1.101 (0.654~1.852) | 0.718 | |||
| 丙氨酸转氨酶(U/L)>44比≤44 | 0.977 (0.573~1.666) | 0.931 | |||
| 碱性磷酸酶(U/L)>129比≤129 | 1.187 (0.794~1.774) | 0.404 | |||
| 肿瘤多发 | 2.212 (1.490~3.284) | <0.001 | 1.857 (1.229~2.807) | 0.003 | |
| 肝硬化 | 1.001 (0.634~1.580) | 0.998 | |||
| 术中输血 | 1.299 (0.861~1.959) | 0.212 | |||
| 分化差 | 1.451 (0.635~3.317) | 0.377 | |||
| 血管侵犯 | 1.871 (1.181~2.964) | 0.008 | 1.871 (1.164~3.007) | 0.010 | |
| TACE | 0.840 (0.547~1.291) | 0.427 | |||
表3
术后复发的单因素、多因素Cox回归分析
| 变量 | 单因素 | 多因素 | |||
|---|---|---|---|---|---|
| 风险比(95%CI) | P值 | 风险比(95%CI) | P值 | ||
| 年龄(岁)55>比≤55 | 0.893 (0.612~1.301) | 0.555 | |||
| 男比女 | 1.082 (0.738~1.585) | 0.687 | |||
| 结石 | 0.804 (0.495~1.307) | 0.380 | |||
| 乙肝表面抗原阳性 | 1.158 (0.794~1.687) | 0.446 | |||
| 甲胎蛋白(μg/L)>20比≤20 | 1.762 (1.138~2.729) | 0.011 | |||
| 糖类抗原19-9(U/L)>39比≤39 | 1.210 (0.832~1.759) | 0.319 | |||
| 癌胚抗原(μg/L)>5比≤5 | 1.555 (1.015~2.382) | 0.042 | |||
| 总胆红素(μmol/L)>17.1比≤17.1 | 0.866 (0.509~1.473) | 0.596 | |||
| 丙氨酸转氨酶(U/L)>44比≤44 | 1.131 (0.682~1.877) | 0.633 | |||
| 碱性磷酸酶(U/L)>129比≤129 | 1.268 (0.585~1.876) | 0.234 | |||
| 肿瘤多发 | 1.927 (1.315~2.826) | 0.001 | 1.885 (1.285~2.765) | 0.001 | |
| 肝硬化 | 0.943 (0.594~1.498) | 0.805 | |||
| 术中输血 | 1.297 (0.872~1.930) | 0.199 | |||
| 分化差 | 1.330 (0.583~3.034) | 0.498 | |||
| 血管侵犯 | 2.536 (1.600~4.020) | <0.001 | 2.748 (1.711~4.412) | <0.001 | |
| TACE | 0.862 (0.566~1.312) | 0.488 | |||
表 4
倾向性评分配对后两组的临床病理特征比较[n(%)]
| 变量 | TACE组 (n=33) | 非TACE组 (n=33) | P值 |
|---|---|---|---|
| 年龄(岁) | 54.0 (46.5~64.5) | 56.0 (46.5~62.5) | 0.768 |
| 男性 | 19 (57.6) | 19 (57.6) | 1.000 |
| 有结石 | 5 (15.2) | 4 (12.1) | 1.000 |
| 乙肝表面抗原阳性 | 15 (45.5) | 17 (51.5) | 0.622 |
| 甲胎蛋白≥20 μg/L | 9 (27.3) | 8 (24.2) | 0.778 |
| 糖类抗原19-9≥39 U/L | 13 (39.4) | 16 (48.5) | 0.457 |
| 癌胚抗原≥5 μg/L | 5 (15.2) | 3 (9.1) | 0.706 |
| 总胆红素≥17.1 μmol/L | 3 (9.1) | 2 (6.1) | / |
| 丙氨酸转氨酶≥44 U/L | 5 (15.2) | 6 (18.2) | 0.741 |
| 碱性磷酸酶≥129 U/L | 9 (27.3) | 11 (33.3) | 0.592 |
| 肿瘤直径(cm) | 11.1 (10.5~13.5) | 11.5 (10.3~12.3) | 0.620 |
| 肿瘤数目 | |||
| 多发 | 16 (48.5) | 14 (42.4) | 0.621 |
| 单发 | 17 (51.5) | 19 (57.6) | |
| 肝硬化 | 7 (21.2) | 6 (18.2) | 0.757 |
| 术中输血 | 13 (39.4) | 7 (21.2) | 0.108 |
| 分化差 | 2 (6.1) | 2 (6.1) | / |
| 血管侵犯 | 9 (27.3) | 7 (21.2) | 0.566 |
| TNM分期 | |||
| Ⅰ: T1bN0M0 | 11 (33.3) | 14 (42.2) | 0.447 |
| Ⅱ: T2N0M0 | 22 (66.7) | 19 (57.6) |
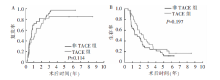
图2
两组倾向性评分匹配后预后比较 A:复发曲线;B:生存曲线
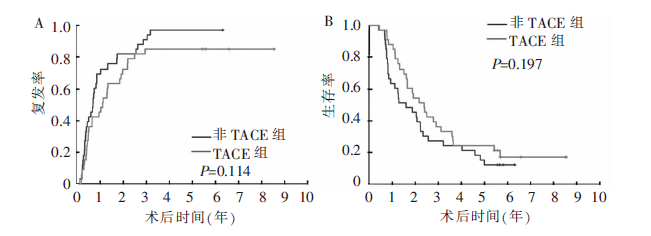
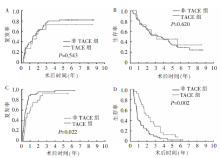
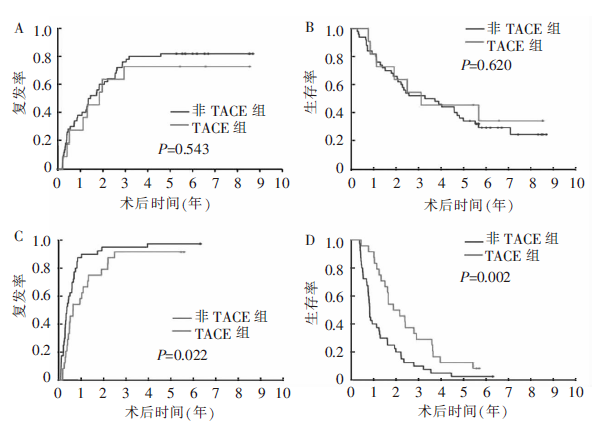
图3
两组TNM分期预后比较 A:TNMⅠ期复发曲线;B:TNMⅠ期生存曲线;C:TNM Ⅱ期复发曲线;D:TNMⅡ期生存曲线
| [1] | Aljiffry M, Abdulelah A, Walsh M, et al. Evidence-based approach to cholangiocarcinoma: a systematic review of the current literature[J]. J Am Coll Surg, 2009, 208(1):134-147. |
| [2] | Wang Y, Li J, Xia Y, et al. Prognostic nomogram for intrahepatic cholangiocarcinoma after partial hepatectomy[J]. J Clin Oncol, 2013, 31(9):1188-1195. |
| [3] |
Bridgewater J, Galle PR, Khan SA, et al. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma[J]. J Hepatol, 2014, 60(6):1268-1289.
doi: 10.1016/j.jhep.2014.01.021 pmid: 24681130 |
| [4] |
Shen WF, Zhong W, Liu Q, et al. Adjuvant transcatheter arterial chemoembolization for intrahepatic cholangiocarcinoma after curative surgery: retrospective control study[J]. World J Surg, 2011, 35(9):2083-2091.
doi: 10.1007/s00268-011-1171-y pmid: 21698503 |
| [5] |
Wu ZF, Zhang HB, Yang N, et al. Postoperative adjuvant transcatheter arterial chemoembolisation improves survival of intrahepatic cholangiocarcinoma patients with poor prognostic factors: results of a large monocentric series[J]. Eur J Surg Oncol, 2012, 38(7):602-610.
doi: 10.1016/j.ejso.2012.02.185 pmid: 22417704 |
| [6] | Li T, Qin LX, Zhou J, et al. Staging, prognostic factors and adjuvant therapy of intrahepatic cholangiocarcinoma after curative resection[J]. Liver Int, 2014, 34(6):953-960. |
| [7] | Jeong S, Zheng B, Wang J, et al. Transarterial chemoembolization: a favorable postoperative management to improve prognosis of hepatitis B virus-associated intrahe-patic cholangiocarcinoma after surgical resection[J]. Int J Biol Sci, 2017, 13(10):1234-1241. |
| [8] | Lu Z, Liu S, Yi Y, et al. Serum gamma-glutamyl transferase levels affect the prognosis of patients with intrahepatic cholangiocarcinoma who receive postoperative adjuvant transcatheter arterial chemoembolization: a propensity score matching study[J]. Int J Surg, 2017, 37:24-28. |
| [9] | Li J, Wang Q, Lei Z, et al. Adjuvant transarterial chemoembolization following liver resection for intrahe-patic cholangiocarcinoma based on survival risk stratifica-tion[J]. Oncologist, 2015, 20(6):640-647. |
| [10] | Wang L, Deng M, Ke Q, et al. Postoperative adjuvant therapy following radical resection for intrahepatic cholangiocarcinoma: a multicenter retrospective study[J]. Cancer Med, 2020, 9(8):2674-2685. |
| [11] |
Austin PC. Some methods of propensity-score matching had superior performance to others: results of an empirical investigation and Monte Carlo simulations[J]. Biom J, 2009, 51(1):171-184.
doi: 10.1002/bimj.200810488 pmid: 19197955 |
| [12] |
Mazzaferro V, Gorgen A, Roayaie S, et al. Liver resection and transplantation for intrahepatic cholangiocarcinoma[J]. J Hepatol, 2020, 72(2):364-377.
doi: S0168-8278(19)30711-1 pmid: 31954498 |
| [13] |
Spolverato G, Kim Y, Alexandrescu S, et al. Is hepatic resection for large or multifocal intrahepatic cholangiocarcinoma justified? results from a multi-institutional colla-boration[J]. Ann Surg Oncol, 2015, 22(7):2218-2225.
doi: 10.1245/s10434-014-4223-3 pmid: 25354576 |
| [14] |
Hyder O, Marques H, Pulitano C, et al. A nomogram to predict long-term survival after resection for intrahepatic cholangiocarcinoma: an Eastern and Western experience[J]. JAMA Surg, 2014, 149(5):432-438.
pmid: 24599477 |
| [15] |
Sapisochin G, Facciuto M, Rubbia-Brandt L, et al. Liver transplantation for “very early” intrahepatic cholangiocarcinoma: international retrospective study supporting a prospective assessment[J]. Hepatology, 2016, 64(4):1178-1188.
doi: 10.1002/hep.28744 pmid: 27481548 |
| [16] | Bruix J, Gores GJ, Mazzaferro V. Hepatocellular carcinoma: clinical frontiers and perspectives[J]. Gut, 2014, 63(5):844-855. |
| [17] | Wang Z, Ren Z, Chen Y, et al. Adjuvant transarterial chemoembolization for HBV-related hepatocellular carcinoma after resection: a randomized controlled study[J]. Clin Cancer Res, 2018, 24(9):2074-2081. |
| [18] | Wang H, Du PC, Wu MC, et al. Postoperative adjuvant transarterial chemoembolization for multinodular hepatocellular carcinoma within the Barcelona Clinic Liver Cancer early stage and microvascular invasion[J]. Hepatobiliary Surg Nutr, 2018, 7(6):418-428. |
| [19] | Ke Q, Lin N, Deng M, et al. The effect of adjuvant therapy for patients with intrahepatic cholangiocarcinoma after surgical resection: a systematic review and meta-analysis[J]. PLoS One, 2020, 15(2):e0229292. |
| [1] | 严晓伟, 刘坤, 胡皆乐, 姜松耀, 项明. 循环肿瘤细胞与胃癌病理分期相关性的初探[J]. 外科理论与实践, 2020, 25(01): 56-59. |
| [2] | 程石, 赵修浩. 胆囊癌治疗的若干热点问题[J]. 外科理论与实践, 2019, 24(02): 100-104. |
| [3] | 施杰毅, 高强, 周俭, 樊嘉. 第8版AJCC肝内胆管癌TNM分期的解读与验证[J]. 外科理论与实践, 2018, 23(03): 221-226. |
| [4] | 石小举, 孙大伟, 王广义,. 腹腔镜技术在不同分期胆囊癌中的应用[J]. 外科理论与实践, 2017, 22(03): 211-214. |
| [5] | 费维嘉, 陈克敏,. 多排CT在结肠直肠癌术前诊断应用价值的分析[J]. 诊断学理论与实践, 2014, 13(03): 316-320. |
| [6] | 洪德飞, 彭淑牖,. 胆囊癌合理根治术的决策依据和疗效评价[J]. 外科理论与实践, 2011, 16(04): 336-339. |
| [7] | 曹晖, 刘申, 金鑫, 刘骅, 王少华, 庄治国, 冯琦,. 多层螺旋CT在结肠直肠肿瘤诊断中的临床应用研究[J]. 外科理论与实践, 2010, 15(02): 123-128. |
| [8] | 王建承, 陈希, 费健, 张卓, 诸琦,. 胰腺癌不同分期方法的比较研究[J]. 外科理论与实践, 2009, 14(05): 519-522. |
| [9] | 周灵, 李庆云, 时国朝, 万欢英,. 肺鳞状细胞癌合并炎性假瘤1例[J]. 内科理论与实践, 2007, 2(03): 208-209. |
| [10] | 张晓青,杨燕青,刘炳亚,金晓龙,李炜,张庆华,林言箴,朱正纲. 弥漫型胃癌基因表达谱聚类分析[J]. 诊断学理论与实践, 2005, 4(03): 192-196. |
| [11] | 张欢,潘自来,宋琦,杜联军,凌华威,丁蓓,陈克敏. 磁共振检查对胃癌术前TNM分期的价值[J]. 诊断学理论与实践, 2004, 3(06): 59-62. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||