诊断学理论与实践 ›› 2019, Vol. 18 ›› Issue (04): 394-401.doi: 10.16150/j.1671-2870.2019.04.004
李蕾1,2, 吴希2, 许冠群2, 梁茜2, 戴菁2, 武文漫2, 丁秋兰2, 王鸿利1, 王学锋2,3( )
)
收稿日期:2019-05-01
出版日期:2019-08-25
发布日期:2019-08-25
通讯作者:
王学锋
E-mail:wangxuefeng6336@hotmail.com
基金资助:
LI Lei1,2, WU Xi2, XU Guanqun2, LIANG Qian2, DAI Jing2, WU Wenman2, DING Qiulan2, WANG Hongli1, WANG Xuefeng2,3()
Received:2019-05-01
Online:2019-08-25
Published:2019-08-25
Contact:
WANG Xuefeng
E-mail:wangxuefeng6336@hotmail.com
摘要:
目的: 研发髙效、准确、简单、实用的易栓症遗传性危险因素的基因检测方法,用于我国易栓症患者的病因诊断和治疗指导。方法: 收集上海交通大学医学院附属瑞金医院血栓与止血门诊246例静脉血栓患者的临床及家系资料,并对其进行遗传性及获得性易栓症表型检测;通过文献研究和人类孟德尔遗传学数据库检索,遴选出18种与血栓发生相关的基因,组成易栓症基因检测Panel,采用二代测序及CNVplex® 高通量拷贝数检测技术对该Panel进行点突变、小缺失/插入及拷贝数变异检测。结果: 246例静脉血栓患者中有159例携带基因突变,突变检出率为64.6%。其中,69.2%的患者携带单一基因突变,13.2%携带单基因的复合杂合突变,另有17.6%携带2种及以上的基因突变。在159例携带基因突变的患者中,有144例患者携带抗凝蛋白基因(SERPINC1、PROS1和PROC)的突变,有31例患者携带其他10种基因(F2、F5、F9、F12、PROCR、THBD、SERPIND1、PLG、ADAMTS13和TFPI)的突变,其中部分突变(F2基因R596Q和F9基因R384Q突变等)被证实与静脉血栓发生相关。拷贝数检测发现,有19例患者存在拷贝数变异,以PROCR及PROS1基因为主。另外,在61例存在获得性血栓危险因素(抗磷脂综合征、手术或妊娠等)的患者中,有40例患者携带遗传性血栓危险因素。56例患者实验室表型检测结果均为正常,而易栓症基因检测Panel结果显示,其中20例患者携带致病性基因突变。72例患者因处于血栓急性期或口服抗凝药物期间,无法进行表型检测,经易栓症基因检测Panel分析发现,其中32例患者携带致病性基因突变。结论: 本研究建立的易栓症基因检测Panel可以快速、有效、准确地对遗传性静脉血栓危险因素进行筛查。对存在获得性血栓危险因素的患者仍有必要进行遗传分析。根据基因检测结果,可评估患者及其家系成员血栓发生风险的大小,制定相应的预防治疗方案,预防血栓的发生或复发,减少血栓后综合征的发生,值得在临床上广泛推广应用。
中图分类号:
李蕾, 吴希, 许冠群, 梁茜, 戴菁, 武文漫, 丁秋兰, 王鸿利, 王学锋. 基于新一代测序技术的易栓症基因检测Panel的建立及其在中国静脉血栓患者遗传背景研究中的临床应用[J]. 诊断学理论与实践, 2019, 18(04): 394-401.
LI Lei, WU Xi, XU Guanqun, LIANG Qian, DAI Jing, WU Wenman, DING Qiulan, WANG Hongli, WANG Xuefeng. Establishment and application of thrombophilia gene detection panel based on next generation sequencing in identification of genetic background of Chinese patients with venous thromboembolism[J]. Journal of Diagnostics Concepts & Practice, 2019, 18(04): 394-401.
表1
易栓症基因检测Panel包含的18种基因
| 基因(蛋白) | OMIM# | 基因(蛋白) | OMIM# |
|---|---|---|---|
| F2(凝血因子Ⅱ) | 188050 | SERPINC1(抗凝血酶) | 613118 |
| F5(凝血因子Ⅴ) | 188055 | PROC(PC) | 176860/612304 |
| F7(凝血因子Ⅶ) | 608446 | PROS1(PS) | 612336/614514 |
| F8(凝血因子Ⅷ) | 300841 | PROCR(内皮细胞PC受体) | 600646 |
| F9(凝血因子Ⅸ) | 300807 | THBD(血栓调节蛋白) | 614486 |
| F10(凝血因子Ⅹ) | 613872 | SERPIND1(肝素辅因子Ⅱ) | 612356 |
| F11(凝血因子Ⅺ) | 264900 | TFPI(组织因子途径抑制物) | 152310 |
| F12(凝血因子Ⅻ) | 610609 | PLG(纤溶酶原) | 217090 |
| ADAMTS13(ADAMTS13) | 274105 | HRG(富组氨酸糖蛋白) | 613116 |
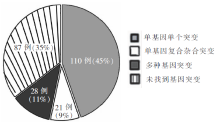
图1
246例静脉血栓栓塞患者的易栓症基因检测Panel结果
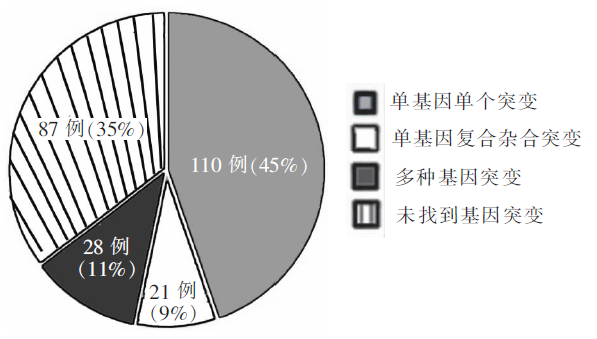
表2
携带单基因单个突变患者的表型及基因检测结果(n)
| 基因名称(蛋白名称) | 受累患者数 | 携带已报道突变的患者数 | 携带新突变的患者数 | 合并获得性血栓危险因素的患者数 | |
|---|---|---|---|---|---|
| 与表型结果一致 | 无表型结果 | ||||
| PROC(PC) | 36 | 31 | 3 | 2 | 9 |
| PROS1(PS) | 43 | 26 | 16 | 1 | 7 |
| SERPINC1(AT) | 17 | 8 | 9 | 0 | 7 |
| F2 (凝血因子Ⅱ) | 1 | 1 | 0 | 0 | 0 |
| F5 (凝血因子Ⅴ) | 2 | 0 | 2 | 0 | 0 |
| F9 (凝血因子Ⅸ) | 1 | 0 | 0 | 1 | 0 |
| F12 (凝血因子Ⅻ) | 1 | 0 | 0 | 1 | 0 |
| PROCR (EPCR) | 4 | 1 | 0 | 3 | 2 |
| THBD (TM) | 2 | 0 | 0 | 2 | 2 |
| SERPIND1(HCⅡ) | 2 | 0 | 0 | 2 | 2 |
| PLG(纤溶酶原) | 1 | 0 | 1 | 0 | 1 |
表3
携带单基因复合杂合突变患者的表型及基因检测结果
| 编号 | 年龄(岁)/ 性别 | VTE次数 (发病年龄) | 获得性血栓 危险因素 | 基因名称 | 突变位点 | 表型结果 |
|---|---|---|---|---|---|---|
| 1 | 50/男 | 1 (49) | 无 | PROC | c.565C>T, p.R189WMI;c.247T>C, p.W83RFI | PC活性 42% |
| 2 | 47/男 | 1 (47) | 无 | PROC | c.565C>T, p.R189WFI;c.325G>C, p.G109RMI | PC活性 38% |
| 3 | 51/男 | 2 (35) | 无 | PROC | c.565C>T, p.R189WMI;c.658C>T, p.R220WFI | PC活性 43% |
| 4 | 22/男 | 2 (21) | 无 | PROC | c.565C>T, p.R189WMI;c.659G>A, p.R220QFI | PC活性 41% |
| 5 | 31/女 | 1 (31) | 避孕药 | PROC | c.565C>T, p.R189WFI;c.1081A>G, p.N361DMI,* | PC活性 36% |
| 6 | 30/男 | 1 (30) | 无 | PROC | c.565C>T, p.R189WFI;c.1130T>C, p.M377TMI | PC活性 35% |
| 7 | 56/男 | 2 (42) | 无 | PROC | c.565C>T, p.R189WMI;c.1157T>C, p.L386PFI | PC活性 32% |
| 8 | 67/男 | 3 (51) | 手术2nd | PROC | c.565C>T, p.R189WFI;c.1140delG, p.V381CfsX39MI,* | PC活性 31% |
| 9 | 14/男 | 1 (14) | 无 | PROC | c.574_576delAAG, p.K192delMI;c.303C>G, p.C101WFI,* | PC活性 48% |
| 10 | 28/男 | 1 (21) | 无 | PROC | c.574_576delAAG, p.K192delMI;c.896_899delACAT, p.D299AfsX15FI,* | PC活性 54% |
| 11 | 32/男 | 1 (32) | 无 | PROC | c.574_576delAAG, p.K192delFI;c.1353delC, p.D451EfsX54MI,* | PC活性 56% |
| 12 | 23/男 | 2 (21) | 无 | PROC | c.574_576delAAG, p.K192delFI;c.1099G>A, p.V367MMI | PC活性 56% |
| 13 | 45/男 | 2 (39) | 无 | PROC | c.574_576delAAG, p.K192delFI;c.678+9C>TMI | PC活性 67% |
| 14 | 35/男 | 1 (34) | 手术 | PROC | c.565C>T, p.R189WFI;c.574_576delAAG, p.K192delMI | PC活性 89% |
| 15 | 25/男 | 2 (18) | 无 | PROC | c.76G>A, p.V26MFI;c.191G>A, p.C64YMI,* | PC活性 15% |
| 16 | 54/男 | 2 (22) | 无 | PROC | c.749C>T, p.T250IFI, *;c.889G>C, p.D297HMI | PC活性 19% |
| 17 | 34/男 | 1 (34) | 无 | PROC | c.889G>C, p.D297HFI;c.1161T>G, p.C387WMI,* | PC活性 21% |
| 18 | 49/女 | 2 (46) | 无 | PROS1 | c.1334G>A, p.R445HFI;c.1155+5G>CMI,* | PS活性 38% |
| 19 | 38/男 | 2 (37) | 无 | PROS1 | c.200A>C, p.E67AFI;c.802G>T, p.D268YMI,* | PS活性 25% |
| 20 | 20/男 | 2 (15) | 无 | PROS1 | c.200A>C, p.E67AFI;c.1681C>T, p.R561WMI | PS活性 23% |
| 21 | 28/男 | 2 (21) | 手术2nd | PROS1 | c.1681C>T, p.R561WFI;c.1551_52delCAinsG, p.T518RfsX41MI,* | PS活性 18% |
表4
携带多种基因突变患者的表型及基因检测结果
| 编号 | 年龄(岁)/ 性别 | VTE次数 (发病年龄) | 获得性血栓 危险因素 | 基因名称 | 突变位点(生物学意义) | 表型结果 |
|---|---|---|---|---|---|---|
| 1 | 29/男 | 2 (27) | 无 | PROC | c.262+2T>C*(T) | PC活性45% |
| PROS1 | c.1680T>A, p.Y560X(T) | PS活性40% | ||||
| 2 | 14/男 | 1 (14) | 无 | PROC | c.889G>C, p.D297H(T) | PC活性52% |
| PROS1 | c.1680T>A, p.Y560X(T) | PS活性53% | ||||
| 3 | 35/男 | 1 (35) | 无 | PROC | c.170G>A, p.R57Q(T) | PC活性104% |
| PROS1 | c.200A>C, p.E67A(T) | PS活性37% | ||||
| 4 | 18/男 | 1 (16) | 无 | PROC | c.574_576delAAG, p.K192del(T) | PC活性103% |
| PROS1 | c.200A>C, p.E67A(T) | PS活性45% | ||||
| 5 | 31/男 | 1 (31) | 无 | PROC | c.574_576delAAG, p.K192del(T) | PC活性101% |
| PROS1 | c.134T>A, p.L45X*(T) | PS活性51% | ||||
| 6 | 48/女 | 2 (47) | 手术2nd | PROC | c.574_576delAAG, p.K192del(T) | PC活性96% |
| PROS1 | exon1-4 deletion*(T) | PS活性62% | ||||
| 7 | 36/男 | 1 (36) | 无 | PROC | c.565C>T, p.R189W(T) | PC活性75% |
| PROS1 | c.1681C>T, p.R561W(T) | PS活性38% | ||||
| 8 | 17/男 | 3 (11) | 无 | PROC | c.574_576delAAG, p.K192del(T) | PC活性93% |
| SERPINC1 | c.1033_1035del, p.E345del(T) | AT活性55% | ||||
| 9 | 38/男 | 2 (25) | 无 | PROC | c.1207dupG, p. P405AfsX19*(T) | PC活性43% |
| SERPINC1 | c.1274G>A, p.R425H(T) | AT活性65% | ||||
| 10 | 40/男 | 1 (39) | 无 | PROC | c.574_576delAAG, p.K192del(T) | PC活性99% |
| SERPINC1 | c.938T>C, p.M313T*(UN) | AT活性96% | ||||
| 11 | 54/男 | 3 (26) | 无 | PROS1 | c.200A>C, p.E67A(T) | PS活性35% |
| SERPINC1 | c.1033_1035del, p.E345del(T) | AT活性57% | ||||
| 12 | 54/男 | 3 (51) | 手术1st, | PROC | c.574_576delAAG, p.K192delH(T) | PC活性113% |
| 卧床3rd | PROCR | c.434C>T, p.P145L(UN) | 未检测 | |||
| 13 | 56/男 | 2 (54) | 无 | PROC | c.703A>C, p.K235Q(T) | PC活性56% |
| PROCR | exon1-3 duplication*(UN) | 未检测 | ||||
| 14 | 31/男 | 2 (29) | 无 | PROC | c.262+2T>C*(T) | PC活性63% |
| PROCR | c.434C>T, p.P145L(UN) | 未检测 | ||||
| 15 | 14/男 | 1 (14) | 无 | PROC | c.574_576delAAG, p.K192del(T) | PC活性 105% |
| PROCR | exon1-3 duplication*(UN) | 未检测 | ||||
| 16 | 22/男 | 1 (19) | 无 | PROS1 | c.1680T>A, p.Y560X(T) | PS活性 52% |
| PROCR | exon1-3 duplication*(UN) | 未检测 | ||||
| 17 | 38/男 | 1 (38) | 手术 | PROS1 | c.1553delC,p.T518RfsX40*(T) | PS活性 37% |
| PROCR | exon1-3 duplication*(UN) | 未检测 | ||||
| 18 | 48/男 | 1 (48) | 无 | PROS1 | c.268C>T, p.R90C(T) | PS活性 47% |
| PROCR | exon1-3 duplication*(UN) | 未检测 | ||||
| 19 | 28/男 | 2 (23) | 无 | SERPINC1 | c.486_487delCT, p.Y163SfsX24(T) | AT活性 57% |
| PROCR | c.434C>T, p.P145L(UN) | 未检测 | ||||
| 20 | 39/男 | 2 (37) | 无 | SERPINC1 | c.1315C>A, p.P439T(T) | AT活性 70% |
| PROCR | c.434C>T, p.P145L(UN) | 未检测 | ||||
| 21 | 41/男 | 2 (39) | 无 | PROC | c.565C>, p.R189W(T) | PC活性 85% |
| PLG | exon1-2 deletion*(UN) | PLG活性 52% | ||||
| 22 | 38/男 | 2 (32) | 无 | PROC | c.574_576delAAG, p.K192del(T) | PC活性 101% |
| THBD | c.840C>A, p.C280X*(UN) | 未检测 | ||||
| 23 | 60/男 | 2 (59) | 无 | PROC | c.574_576delAAG, p.K192del(T) | PC活性 111% |
| F5 | c.1114G>C, p.D372H*(UN) | FⅤ活性 94% | ||||
| 24 | 34/男 | 2 (24) | 外伤1st, 2nd | PROS1 | c.200A>C, p.E67A(T) | PS活性 40% |
| TFPI | c.757A>G, p.N253D*(UN) | 未检测 | ||||
| 25 | 33/男 | 1 (33) | 无 | PROS1 | exon7-15 deletion*(T) | PS 活性 37% |
| ADAMTS13 | c.923C>G, p.T308R*(UN) | VWF:Ag 166% | ||||
| 26 | 53/女 | 1 (52) | 手术 | F5 | c.1663A>C, p.K555Q*(UN) | FⅤ活性 107% |
| PROCR | exon1-3 duplication*(UN) | 未检测 | ||||
| 27 | 32/男 | 3 (16) | 抗磷脂综合征 | PROC | c.574_576delAAG, p.K192del(T) | PC活性 111% |
| PROS1 | c.751_752delAT,p.M251VfsX16*(T) | PS活性 39% | ||||
| PROCR | exon1-3 duplication*(UN) | 未检测 | ||||
| 28 | 23/男 | 2 (21) | 无 | PROC | c.-148T>C H*(T) | PC活性 14% |
| F2 | c.1436A>G, p.H479R*(UN) | FⅡ活性 75% | ||||
| F12 | c.1417G>C, p.G473RH*(UN) | FⅫ活性 15% |
| [1] | 丁秋兰, 王学锋. 遗传性易栓症的表型和基因诊断流程[J]. 诊断学理论与实践, 2019, 18(2):127-132. |
| [2] |
Ding Q, Wang M, Xu G, et al. Molecular basis and thrombotic manifestations of antithrombin deficiency in 15 unrelated Chinese patients[J]. Thromb Res, 2013, 132(3):367-373.
doi: 10.1016/j.thromres.2013.07.013 URL |
| [3] |
Ding Q, Shen W, Ye X, et al. Clinical and genetic features of protein C deficiency in 23 unrelated Chinese patients[J]. Blood Cells Mol Dis, 2013, 50(1):53-58.
doi: 10.1016/j.bcmd.2012.08.004 URL |
| [4] |
Li L, Wu X, Wu W, et al. Clinical Manifestation and Mutation Spectrum of 53 Unrelated Pedigrees with Protein S Deficiency in China[J]. Thromb Haemost, 2019, 119(3):449-460.
doi: 10.1055/s-0038-1677031 URL |
| [5] |
Simioni P, Tormene D, Tognin G, et al. X-linked thrombophilia with a mutant factor IX (factor IX Padua)[J]. N Engl J Med, 2009, 361(17):1671-1675.
doi: 10.1056/NEJMoa0904377 URL |
| [6] |
Ichinose A, Espling ES, Takamatsu J, et al. Two types of abnormal genes for plasminogen in families with a predisposition for thrombosis[J]. Proc Natl Acad Sci U S A, 1991, 88(1):115-119.
pmid: 1986355 |
| [7] |
Shigekiyo T, Yoshida H, Matsumoto K, et al. HRG Tokushima: molecular and cellular characterization of histidine-rich glycoprotein (HRG) deficiency[J]. Blood, 1998, 91(1):128-133.
pmid: 9414276 |
| [8] |
Moatti D, Haidar B, Fumeron F, et al. A new T-287C polymorphism in the 5' regulatory region of the tissue factor pathway inhibitor gene. Association study of the T-287C and C-399T polymorphisms with coronary artery disease and plasma TFPI levels[J]. Thromb Haemost, 2000, 84(2):244-249.
doi: 10.1055/s-0037-1614003 URL |
| [9] |
Hu B, Wang QY, Tang L, et al. Association of thrombomodulin c.1418C>T polymorphism and venous thromboembolism[J]. Gene, 2017, 628:56-62.
doi: 10.1016/j.gene.2017.07.024 URL |
| [10] |
Wu C, Dwivedi DJ, Pepler L, et al. Targeted gene sequencing identifies variants in the protein C and endothelial protein C receptor genes in patients with unprovoked venous thromboembolism[J]. Arterioscler Thromb Vasc Biol, 2013, 33(11):2674-2681.
doi: 10.1161/ATVBAHA.113.302137 URL |
| [11] |
Villa P, Aznar J, Vaya A, et al. Hereditary homozygous heparin cofactor II deficiency and the risk of developing venous thrombosis[J]. Thromb Haemost, 1999, 82(3):1011-1014.
doi: 10.1055/s-0037-1614320 URL |
| [12] |
Lee EJ, Dykas DJ, Leavitt AD, et al. Whole-exome sequencing in evaluation of patients with venous thromboembolism[J]. Blood Adv, 2017, 1(16):1224-1237.
doi: 10.1182/bloodadvances.2017005249 URL |
| [13] |
Yin T, Takeshita S, Sato Y, et al. Alarge deletion of the PROS1 gene in a deep vein thrombosis patient with protein S deficiency[J]. Thromb Haemost, 2007, 98(4):783-789.
doi: 10.1160/TH07-03-0211 URL |
| [14] |
Choung HS, Kim HJ, Gwak GY, et al. Inherited protein S deficiency as a result of a large duplication mutation of the PROS1 gene detected by multiplex ligation-dependent probe amplification[J]. J Thromb Haemost, 2008, 6(8):1430-1432.
doi: 10.1111/j.1538-7836.2008.03026.x pmid: 18489710 |
| [15] |
Reitsma PH. Genetics in thrombophilia. An update[J]. Hamostaseologie, 2015, 35(1):47-51.
doi: 10.5482/HAMO-14-11-0062 pmid: 25465384 |
| [16] |
Zhang Z, Li C, Wu F, et al. Genomic variations of the mevalonate pathway in porokeratosis[J]. ELife, 2015, 4:e06322.
doi: 10.7554/eLife.06322 URL |
| [17] |
Richards S, Aziz N, Bale S, et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology[J]. Genet Med, 2015, 17(5):405-424.
doi: 10.1038/gim.2015.30 pmid: 25741868 |
| [18] |
Sivasundar S, Oommen AT, Prakash O, et al. Molecular defect of 'Prothrombin Amrita': substitution of arginine by glutamine (Arg553 to Gln) near the Na(+) binding loop of prothrombin[J]. Blood Cells Mol Dis, 2013, 50(3):182-183.
doi: 10.1016/j.bcmd.2012.11.008 URL |
| [19] |
Djordjevic V, Kovac M, Miljic P, et al. A novel prothrombin mutation in two families with prominent thrombophi-lia--the first cases of antithrombin resistance in a Caucasian population[J]. J Thromb Haemost, 2013, 11(10):1936-1939.
doi: 10.1111/jth.12367 pmid: 23927452 |
| [20] |
Baglin T, Gray E, Greaves M, et al. Clinical guidelines for testing for heritable thrombophilia[J]. Br J Haematol, 2010, 149(2):209-220.
doi: 10.1111/j.1365-2141.2009.08022.x URL |
| [21] |
Connors JM. Thrombophilia Testing and Venous Thrombosis[J]. N Engl J Med, 2017, 377(12):1177-1187.
doi: 10.1056/NEJMra1700365 URL |
| [1] | 张伯玮, 任静, 马睿, 门剑龙. D-二聚体在静脉血栓栓塞症诊疗中的应用临床实践[J]. 诊断学理论与实践, 2020, 19(05): 469-473. |
| [2] | 丁秋兰, 王学锋. 遗传性易栓症的表型和基因诊断流程[J]. 诊断学理论与实践, 2019, 18(2): 127-132. |
| [3] | 门剑龙, 任静. 静脉血栓栓塞症的危险因素和危险分层诊断[J]. 诊断学理论与实践, 2019, 18(1): 10-15. |
| [4] | 毛毅敏, 黄伸伸, 和雪改. 围手术期静脉血栓栓塞症形成风险评估及抗凝药物管理[J]. 诊断学理论与实践, 2019, 18(1): 16-20. |
| [5] | 杜云志, 冯菁华, 常春康. 二代测序技术在骨髓增生异常综合征临床诊断和治疗决策中的应用进展[J]. 诊断学理论与实践, 2019, 18(06): 685-671. |
| [6] | 宋元林, 侯东妮. 支气管扩张症患者气道、肠道微生态的研究及临床价值[J]. 诊断学理论与实践, 2019, 18(05): 503-508. |
| [7] | 冯国栋, 贺旻, 汪昕. 二代测序技术在诊断神经系统感染性疾病中的应用[J]. 诊断学理论与实践, 2018, 17(04): 391-395. |
| [8] | 陈冰, 眭竫旎. 急性髓系白血病微小残留病监测方式的展望[J]. 诊断学理论与实践, 2017, 16(01): 17-26. |
| [9] | 宋陆茜, 常春康. 二代测序技术在骨髓增生异常综合征诊治中的临床应用[J]. 诊断学理论与实践, 2016, 15(06): 556-560. |
| [10] | 蒋米尔, 殷敏毅,. 静脉血栓栓塞症的诊断现状[J]. 诊断学理论与实践, 2011, 10(02): 93-96. |
| [11] | 区满春, 曾敏怡, 石任任, 陈靖, 方劭桦, 谢玮, 冯莹,. 静脉血栓栓塞症高危因素和临床表现的荟萃分析[J]. 诊断学理论与实践, 2011, 10(02): 113-116. |
| [12] | 冯莹,. 静脉血栓形成的危险因素[J]. 诊断学理论与实践, 2011, 10(02): 101-104. |
| [13] | 陈华云, 胡晓波,. D-二聚体定量检测在排除静脉血栓性疾病中的作用——推荐性指南(CLSI H59-P)解读[J]. 诊断学理论与实践, 2011, 10(02): 168-171. |
| [14] | 包承鑫,. 遗传性易栓症实验诊断中的若干问题[J]. 诊断学理论与实践, 2011, 10(02): 109-112. |
| [15] | 周荣富, 王鸿利,. 易栓症的实验诊断[J]. 诊断学理论与实践, 2008, 7(05): 574-578. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||