诊断学理论与实践 ›› 2019, Vol. 18 ›› Issue (06): 649-654.doi: 10.16150/j.1671-2870.2019.06.009
许海敏1, 陈晓炎1( ), 张静2, 王朝夫1
), 张静2, 王朝夫1
收稿日期:2019-08-01
出版日期:2019-12-25
发布日期:2019-12-25
通讯作者:
陈晓炎
E-mail:cxy11832@rjh.com.cn
XU Haimin1, CHEN Xiaoyan1(), ZHANG Jing2, WANG Chaofu1
Received:2019-08-01
Online:2019-12-25
Published:2019-12-25
Contact:
CHEN Xiaoyan
E-mail:cxy11832@rjh.com.cn
摘要:
目的:探讨肺胶样腺癌(colloid adenocarcinoma, CA)的临床病理学特征、免疫表型、分子特征及鉴别诊断。方法:回顾性分析4例肺CA患者的临床病理资料,并结合相关文献进行探讨。结果:4例均为老年男性,年龄为61~67岁,中位年龄为64岁,其中3例有吸烟史,临床表现为乏力、咳嗽等非特异性症状,或因体检发现。肿瘤位于右肺上叶3例,右肺下叶1例。胸部CT检查提示病灶呈实性结节状或团块状。大体检查,3例为外周型,1例几乎占据整个肺叶,最大径为1.6~12.0 cm,切面呈灰白色,黏冻样,有光泽。光镜检查可见,肿瘤组织富含黏液,形成黏液池,肺泡间隔断裂。肿瘤细胞呈单个、簇状、条索状或微乳头状,漂浮于黏液池中,少量肿瘤细胞贴壁生长,4例肿瘤中3例可见微乳头成分。细胞呈杯状细胞或印戒细胞形态,中度异型,核分裂相少见。2例黏液池中可见少量砂砾体。免疫组织化学(免疫组化)检查结果显示,4例均表达CK7及MUC-1,1例表达CK20;3例表达TTF-1与NapsinA,其中1例两者均弥漫表达,2例两者均局灶表达;2例表达CDX-2、MUC-2及Villin;3例表达MUC5AC。4例中2例行分子检测,1例行EGFR、ALK及ROS1基因检测,未检测到基因改变;另1例行数字PCR检测,检测到KRAS外显子2基因突变。随访结果显示,3例伴微乳头结构的病例中,2例出现转移,其中1例病灶伴有少量实性成分者出现远处转移;另1例虽无微乳头结构,但肿瘤巨大,术后半年患者因肺部感染、呼吸衰竭死亡。结论:肺CA是一种少见的原发性肺腺癌,明确诊断依赖病理组织学检查及免疫组化检查,TTF-1及NapsinA阳性有助于原发性肺CA的诊断,当两者均阴性时要综合形态学、免疫表型及临床病史排除转移的可能性;大部分肺CA患者预后较好,但出现微乳头结构提示预后不佳。
中图分类号:
许海敏, 陈晓炎, 张静, 王朝夫. 肺胶样腺癌4例临床病理分析及文献复习[J]. 诊断学理论与实践, 2019, 18(06): 649-654.
XU Haimin, CHEN Xiaoyan, ZHANG Jing, WANG Chaofu. Pulmonary colloid adenocarcinoma: Clinical pathological analysis of 4 cases and review of literature[J]. Journal of Diagnostics Concepts & Practice, 2019, 18(06): 649-654.
表1
4例CA患者的临床资料
| 病例 | 性别 | 年龄 (岁) | 吸烟 史 | 症状 | 体积(cm) | PET/CT | 部位 | 手术方式 | 病理分期 | 随访 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 男 | 61 | 无 | 体检发现,无症状 | 1.6×1.6 ×1.5 | 代谢轻度增高 | 右肺上叶 | 肺段切除+纵隔 淋巴结清除 | ⅢA (T1bN2M0) | 术后34个月无复发及远处转移 |
| 2 | 男 | 67 | 有 | 咳嗽、咳痰,胸闷、气促 | 2.9×1.7 ×1.5 | 未查 | 右肺下叶 | 肺叶切除+纵隔 淋巴结清除 | ⅠA3 (T1cN0M0) | 术后半年发生骨转移及脑转移 |
| 3 | 男 | 66 | 有 | 体检发现,无症状 | 1.6×1.0 ×1.0 | 未查 | 右肺上叶 | 肺叶切除+纵隔 淋巴结清除 | ⅠA2 (T1bN0M0) | 术后31个月无 复发转移 |
| 4 | 男 | 62 | 有 | 全身乏力半年余 | 12.0×11.0 ×8.0 | 代谢轻度增高 | 右肺上叶 | 肺叶切除+纵隔 淋巴结清除 | ⅢA (T4N0M0) | 术后半年因肺部感染、呼吸衰竭死亡 |

图1
肿瘤组织内黏液池形成及肺泡间隔断裂(HE,×100)
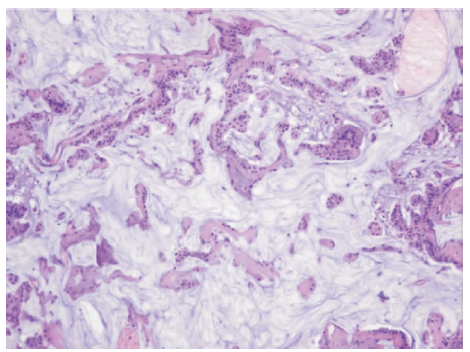
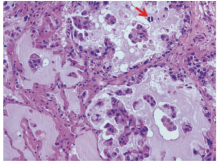
图2
肿瘤细胞表现(HE,×200) 肿瘤细胞呈单个、簇状、小条索状、微乳头状,漂浮于黏液池中,少量贴壁生长,红色箭头所指处可见砂砾体
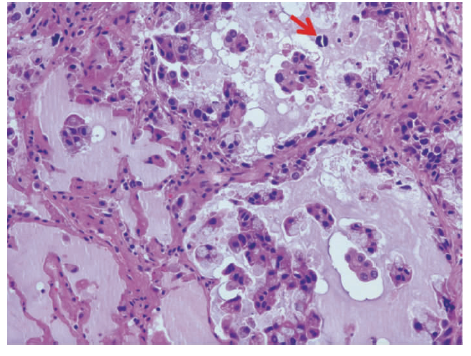
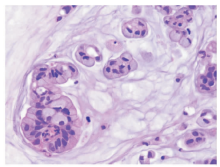
图3
肿瘤细胞呈杯状细胞形态或印戒细胞形态(HE,×400) 肿瘤细胞中度异型且核分裂相少见

表2
4例CA的免疫组化标志物检测结果
| 病例 | TTF-1 | NapsinA | SP-A | CK7 | CK20 | CDX-2 | Villin | MUC-1 | MUC-2 | MUC5AC |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | - | - | - | + | - | - | - | F+ | - | F+ |
| 2 | F+ | F+ | - | + | - | + | F+ | + | F+ | + |
| 3 | + | + | - | + | - | - | - | + | - | + |
| 4 | F+ | F+ | F+ | + | + | + | F+ | F+ | + | - |

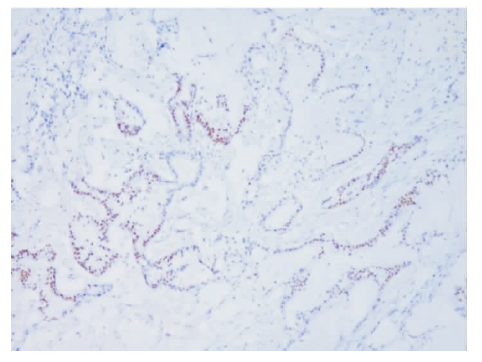
图4
TTF-1免疫组化染色(×100)
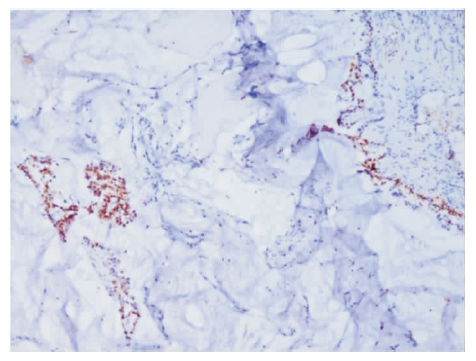
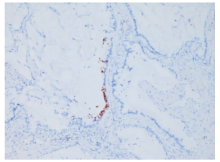
图5
NapsinA免疫组化染色(×100)
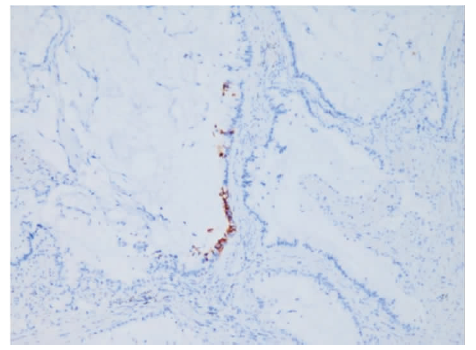
图6
CDX-2免疫组化染色(×100)
| [1] | Travis WD, Brambilla E, Burke AP, et al. WHO Classification oftumours of the lung, pleura, thymus and heart[M]. Lyon: IARC Press, 2015:40-41. |
| [2] |
Zenali MJ, Weissferdt A, Solis LM, et al. An update on clinicopathological, immunohistochemical, and molecular profiles of colloid carcinoma of the lung[J]. Hum Pathol, 2015, 46(6): 836-842.
doi: 10.1016/j.humpath.2014.10.032 URL |
| [3] |
Sonzogni A, Bianchi F, Fabbri A, et al. Pulmonary adenocarcinoma with mucin production modulates phenotype according to common genetic traits: a reappraisal of mucinous adenocarcinoma and colloid adenocarcinoma[J]. J Pathol Clin Res, 2017, 3(2):139-152.
doi: 10.1002/cjp2.67 URL |
| [4] |
Cha YJ, Shim HS, Han J, et al. Clinicopathologic ana-lysis of 10 cases of pulmonary colloid adenocarcinoma and prognostic implication of invasive micropapillary component[J]. Pathol Res Pract, 2018, 214(12):2093-2098.
doi: 10.1016/j.prp.2018.10.014 URL |
| [5] | Masai K, Sakurai H, Suzuki S, et al. Clinicopathological features of colloid adenocarcinoma of the lung: A report of six cases[J]. JSurg Oncol, 2016, 114(2):211-215. |
| [6] |
Rossi G, Murer B, Cavazza A, et al. Primary mucinous (so-called colloid) carcinomas of the lung: a clinicopathologic and immunohistochemical study with special refe-rence to CDX-2 homeobox gene and MUC2 expression[J]. Am J Surg Pathol, 2004, 28(4):442-452.
doi: 10.1097/00000478-200404000-00003 URL |
| [7] |
Graeme-Cook F, Mark EJ. Pulmonary mucinous cystic tumors of borderline malignancy[J]. Hum Pathol, 1991, 22(2):185-190.
pmid: 2001880 |
| [8] | Moran CA, Hochholzer L, Fishback N, et al. Mucinous (so-called colloid) carcinomas of lung[J]. Mod Pathol, 1992, 5(6): 634-638. |
| [9] |
Gao ZH, Urbanski S J. The spectrum of pulmonary mu-cinous cystic neoplasia : a clinicopathologic and immunohistochemical study of ten cases and review of litera-ture[J]. Am J Clin Pathol, 2005, 124(1):62-70.
doi: 10.1309/52XXR6E6U0J2JX0F URL |
| [10] |
Berger K L, Nicholson S A, Dehdashti F, et al. FDG PET evaluation of mucinous neoplasms: correlation of FDG uptake with histopathologic features[J]. Am J Roentgenol, 2000, 174(4):1005-1008.
pmid: 10749239 |
| [11] |
Shim S S, Han J. FDG-PET/CT imaging in assessing mucin-producing non-small cell lung cancer with pathologic correlation[J]. Ann Nucl Med, 2010, 24(5):357-362.
doi: 10.1007/s12149-010-0358-x URL |
| [12] | Miyake A, Okudela K, Matsumura M, et al. Update on the potential significance of psammoma bodies in lung adenocarcinoma from a modern perspective[J]. Histopatho-logy, 2018, 72(4):609-618. |
| [13] |
Chang JC, Montecalvo J, Borsu L, et al. Bronchiolar adenoma: expansion of the concept of ciliated mucono-dular papillary tumors with proposal for revised terminology based on morphologic, immunophenotypic, and genomic analysis of 25 cases[J]. Am J Surg Pathol, 2018, 42(8):1010-1026.
doi: 10.1097/PAS.0000000000001086 URL |
| [14] |
Chuang H W, Liao J B, Chang H C, et al. Ciliated muconodular papillary tumor of the lung: a newly defined peripheral pulmonary tumor with conspicuous mucin pool mimicking colloid adenocarcinoma: a case report and review of literature[J]. Pathol Int, 2014, 64(7):352-357.
doi: 10.1111/pin.12179 URL |
| [15] | 陈晓炎, 杨晓群, 袁菲, 等. 肺纤毛黏液结节性乳头状肿瘤2例临床病理分析及文献复习[J]. 诊断学理论与实践, 2018, 17(5):575-580. |
| [16] |
Ye J, Findeis-Hosey JJ, Yang Q, et al. Combination of napsin A and TTF-1 immunohistochemistry helps in differentiating primary lung adenocarcinoma from metastatic carcinoma in the lung[J]. Appl Immunohistochem Mol Morphol, 2011, 19(4):313-317.
doi: 10.1097/PAI.0b013e318205b059 URL |
| [17] |
Rossi G, Cavazza A, Righi L, et al. Napsin-A, TTF-1, EGFR, and ALK status determination in lung primary and metastatic mucin-producing adenocarcinomas[J]. Int J Surg Pathol, 2014, 22(5):401-407.
doi: 10.1177/1066896914527609 URL |
| [18] |
Kalhor N. Colloid carcinoma of the lung: Current views[J]. Semin Diagn Pathol, 2014, 31(4):265-270.
doi: 10.1053/j.semdp.2014.06.003 pmid: 25239272 |
| [19] | Morita K, Nagashima A, Takemoto N, et al. Primary pulmonary mucinous (colloid) adenocarcinoma with postope-rative bone metastasis[J]. Ann Thorac Cardiovas Surg, 2014, 20(Suppl):677-681. |
| [1] | 石峰, 郭竹英, 郭海艳. 新型冠状病毒肺炎患者外周血淋巴细胞亚群变化的临床意义[J]. 诊断学理论与实践, 2022, 21(05): 619-624. |
| [2] | 孙艳艳, 兰信堂. 肺癌颅脑转移患者接受放射治疗后前庭功能受损1例[J]. 诊断学理论与实践, 2022, 21(05): 632-634. |
| [3] | 张祥钦, 江勇. 宏基因组第二代测序技术诊断鹦鹉热衣原体肺炎1例[J]. 诊断学理论与实践, 2022, 21(05): 635-637. |
| [4] | 车稳, 柳蒋书, 陈晓炎, 王朝夫, 袁菲, 王璇. 肺混合性鳞状细胞和腺性乳头状瘤2例临床病理特征及冷冻切片病理诊断误诊分析[J]. 诊断学理论与实践, 2022, 21(04): 476-481. |
| [5] | 包志瑶, 孟文凯, 沈继敏, 李庆云. 成人继发于化脓性扁桃体炎的血行播散性肺炎1例报道并文献复习[J]. 诊断学理论与实践, 2022, 21(04): 520-523. |
| [6] | 杜燕然, 焦景, 任芸芸, 周建桥. 超声影像组学技术在评估胎肺成熟度中的应用[J]. 诊断学理论与实践, 2022, 21(03): 326-330. |
| [7] | 陈沁, 徐雯莉, 丰青, 陈瑜, 邓雪芹, 陈芸, 庞碧芸. 新型冠状病毒肺炎收治定点医院护理人力资源的调配与实践[J]. 诊断学理论与实践, 2022, 21(02): 273-276. |
| [8] | 张红, 朱梦梦. 新型冠状病毒肺炎疫情期间老年人进食安全护理[J]. 诊断学理论与实践, 2022, 21(02): 277-280. |
| [9] | 梁婧, 黄晨, 蒋琰, 许敬华, 梁晓虹, 杨之涛, 景峰. 新冠疫情下急诊输液室的护理防控管理策略[J]. 诊断学理论与实践, 2022, 21(02): 281-285. |
| [10] | 黄晨, 景峰, 杨之涛, 陈影, 谢之辉, 张祎博, 尚寒冰, 林靖生, 吴文娟, 顾志冬, 毕宇芳, 陈尔真. 方舱医院护理管理体系建设的探索与实践[J]. 诊断学理论与实践, 2022, 21(02): 286-290. |
| [11] | 新冠病毒定点医院公共学科工作模式撰写组. 上海交通大学医学院附属瑞金医院抗击新型冠状病毒定点医院公共学科工作模式[J]. 诊断学理论与实践, 2022, 21(02): 118-127. |
| [12] | 中华医学会内分泌学分会. 新型冠状病毒肺炎疫情下骨质疏松症管理专家建议[J]. 诊断学理论与实践, 2022, 21(02): 133-135. |
| [13] | 中华医学会内分泌学分会. 新型冠状病毒肺炎疫情下肾上腺疾病管理专家建议[J]. 诊断学理论与实践, 2022, 21(02): 139-142. |
| [14] | 陈长强, 孟俊, 金佩佩, 戴菁. 定点医院新型冠状病毒肺炎患者核酸检测工作的实践和探索[J]. 诊断学理论与实践, 2022, 21(02): 143-149. |
| [15] | 施莺莺, 钟旭, 刘嘉琳, 何乐, 熊少洁, 翁懿, 丁成唯, 杨溢, 陈伟红, 邱力萍, 辛海光. 新型冠状病毒疫情相关防疫工作人员感染防控实践调查分析及对策[J]. 诊断学理论与实践, 2022, 21(02): 178-183. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||