诊断学理论与实践 ›› 2020, Vol. 19 ›› Issue (03): 297-302.doi: 10.16150/j.1671-2870.2020.03.017
刘圣均1, 刘莉莉1, 朱政斌1, 孙宜2, 朱天奇1, 冯硕1, 陈馨1, 权薇薇1( ), 张瑞岩1()
), 张瑞岩1()
收稿日期:2020-04-25
出版日期:2020-06-25
发布日期:2020-06-25
通讯作者:
权薇薇,张瑞岩
E-mail:qww10826@rjh.com.cn;zhangruiyan@263.net
基金资助:
LIU Shengjun1, LIU Lili1, ZHU Zhengbin1, SUN Yi2, ZHU Tianqi1, FENG Shuo1, CHEN Xin1, QUAN Weiwei1(), ZHANG Ruiyan1()
Received:2020-04-25
Online:2020-06-25
Published:2020-06-25
Contact:
QUAN Weiwei,ZHANG Ruiyan
E-mail:qww10826@rjh.com.cn;zhangruiyan@263.net
摘要:
目的: 探索冠状动脉(冠脉)药物洗脱支架植入(以下简称支架植入)术后随访期估算肾小球滤过率(estimated glomerular filtration rate, eGFR)与支架植入术后再狭窄(in-stent restenosis, ISR)间的关系。方法: 以中国冠状动脉斑块进展多因素回顾分析研究中的患者为对象,病例均于2010年1月至2016年7月间在各中心进行冠脉造影检查,并在之后12~24个月(平均为13个月)内进行冠脉造影复查,采用二元Logistics回归分析评估随访期eGFR与ISR间的关系,初步探索导致ISR发生的危险因素。结果: 本研究共纳入符合标准的冠心病患者1 790例,随访期全体患者eGFR平均值为89.97 mL/(min·1.73m2),按照随访期复查冠脉造影有无ISR,分为ISR组(n=200)和无ISR组(n=1590)。其中,ISR组患者在随访期间的eGFR低于无ISR组[(86.50±25.69) mL/(min·1.73 m2)比(90.64±26.59) mL/(min·1.73 m2),P=0.038]。二元Logistics回归分析提示,导致ISR的危险因素包括植入支架的个数(OR=1.478, 95% CI 1.177~1.855, P=0.001)、基线期C反应蛋白升高(OR=1.006, 95%CI 1.002~1.011, P=0.007),而随访期间相对较高的eGFR是ISR的保护性因素(OR=0.990,95%CI 0.982~0.999, P=0.022)。结论: 在eGFR基本正常的冠心病患者中,较低的随访期eGFR水平与其接受冠脉药物洗脱支架植入术后的ISR发生率密切相关。
中图分类号:
刘圣均, 刘莉莉, 朱政斌, 孙宜, 朱天奇, 冯硕, 陈馨, 权薇薇, 张瑞岩. 肾小球滤过率与冠状动脉支架内再狭窄的相关性分析[J]. 诊断学理论与实践, 2020, 19(03): 297-302.
LIU Shengjun, LIU Lili, ZHU Zhengbin, SUN Yi, ZHU Tianqi, FENG Shuo, CHEN Xin, QUAN Weiwei, ZHANG Ruiyan. Correlation of estimated glomerular filtration rate with incidence of in-stent restenosis in patients with drug-elu-ting stent[J]. Journal of Diagnostics Concepts & Practice, 2020, 19(03): 297-302.

图1
支架植入前、后及随访期间冠脉造影图像 A:基线期,右冠状动脉近段75%狭窄伴开口瘤样扩张(虑线),右冠状动脉中远段85%狭窄(实线);B:基线期,右冠状动脉近段及中远段支架植入;C:随访期,右冠状动脉近段40%狭窄,右冠状动脉中远段95%狭窄
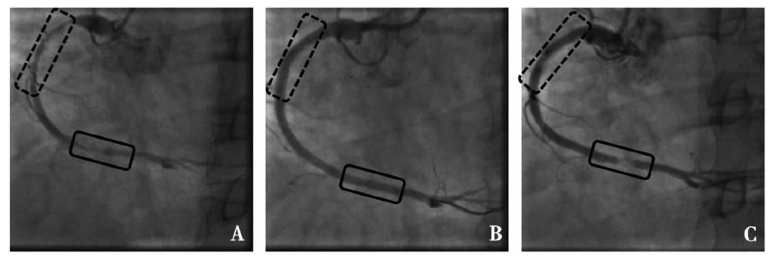
表1
ISR组与无ISR组的一般情况比较
| 项目 | 无ISR组(n=1 590) | ISR组(n=200) | P值 |
|---|---|---|---|
| 临床特征 | |||
| 年龄(岁) | 63.45±10.79 | 63.09±10.15 | 0.658 |
| 男性 [n(%)] | 1 169(73.5%) | 147(73.5%) | 0.995 |
| 体质量指数(kg/m2) | 25.46±3.22 | 25.49±3.4 | 0.919 |
| 基线期收缩压(mmHg) | 131.48±17.46 | 130.82±16.61 | 0.613 |
| 基线期舒张压(mmHg) | 78.15±10.62 | 77.5±10.81 | 0.415 |
| 随访期收缩压(mmHg) | 130.11±15.24 | 131.27±16.82 | 0.316 |
| 随访期舒张压(mmHg) | 77.29±9.60 | 77.51±10.42 | 0.758 |
| 基线期射血分数(%) | 61.59±8.36 | 62.17±7.72 | 0.366 |
| 随访期射血分数(%) | 61.94±8.02 | 61.27±8.75 | 0.287 |
| 冠脉造影信息 | |||
| 2次造影间隔时间(d) | 446.75±102.06 | 456.87±100.70 | 0.186 |
| 植入支架数*(个) | 1 (1~2) | 1 (1~2) | 0.006 |
| 平均支架长度(mm) | 26.0 (19.8~33.4) | 28.0 (20.9~34.9) | 0.171 |
| 合并症 | |||
| 高血压[n(%)] | 1 017(64.0%) | 135(64.0%) | 0.325 |
| 糖尿病[n(%)] | 908(57.1%) | 112(57.1%) | 0.766 |
| 高脂血症[n(%)] | 241(15.2%) | 35(15.2%) | 0.387 |
| 慢性肾病病史[n(%)] | 31(1.9%) | 3(1.9%) | 0.661 |
| 急性冠脉综合征病史[n(%)] | 267(16.8%) | 41(16.8%) | 0.190 |
| 外周血管病史[n(%)] | 128(8.1%) | 15(8.1%) | 0.787 |
| 卒中病史[n(%)] | 87(5.5%) | 16(5.5%) | 0.148 |
| 吸烟史[n(%)] | 674(42.4%) | 89(42.4%) | 0.570 |
| 药物治疗 | |||
| P2Y12受体拮抗剂使用 [n(%)] | 1 526(96.0%) | 190(96.0%) | 0.514 |
| 降脂药使用[n(%)] | 1 538(96.7%) | 193(96.7%) | 0.864 |
| ACEI和(或)ARB使用[n(%)] | 911(57.3%) | 114(57.3%) | 0.937 |
| β受体阻滞剂使用[n(%)] | 1 162(73.1%) | 144(73.1%) | 0.745 |
表2
ISR组与无ISR组的实验室检查指标比较
| 项目 | 基线期 | 随访期 | |||||
|---|---|---|---|---|---|---|---|
| 无ISR组 | ISR组 | P值 | 无ISR组 | ISR组 | P值 | ||
| 肾功能相关指标 | |||||||
| 尿酸(μmol/L) | 335.97±96.20 | 334.12±97.49 | P>0.05 | 334.12±97.49 | 337.95±91.21 | P>0.05 | |
| eGFR[mL/(min·1.73 m2)] | 91.53±27.53 | 88.10±26.27 | P<0.05 | 88.10±26.27 | 86.50±25.69 | P<0.05 | |
| 其他实验室指标 | |||||||
| C反应蛋白(mg/L) | 1.6(0.7~5.1) | 2.6(0.8~8.5) | P>0.05 | 2.6(0.8~8.5) | 0.9(0.5~2.5) | P>0.05 | |
| 空腹血糖(mmol/L) | 6.19±2.36 | 6.53±3.16 | P>0.05 | 6.53±3.16 | 6.19±2.26 | P>0.05 | |
| 总胆固醇(mmol/L) | 4.25±1.20 | 4.19±1.14 | P>0.05 | 4.19±1.14 | 3.64±0.87 | P>0.05 | |
| 甘油三酯(mmol/L) | 1.84±1.30 | 1.72±1.14 | P>0.05 | 1.72±1.14 | 1.59±1.24 | P>0.05 | |
| 高密度脂蛋白胆固醇(mmol/L) | 1.05±0.29 | 1.07±0.28 | P>0.05 | 1.07±0.28 | 1.08±0.31 | P>0.05 | |
| 低密度脂蛋白胆固醇(mmol/L) | 2.50±0.93 | 2.44±0.86 | P>0.05 | 2.44±0.86 | 2.01±0.68 | P>0.05 | |
表3
ISR相关危险因素分析
| 项目 | 单因素分析 | 多因素分析 | |||
|---|---|---|---|---|---|
| P值 | β值 | P值 | OR(95% CI) | ||
| 性别(男性) [n(%)] | 0.995 | -0.163 | 0.379 | 0.850(0.592~1.221) | |
| 年龄(岁) | 0.658 | -0.024 | <0.001 | 0.976(0.968~0.984) | |
| 糖尿病 [n(%)] | 0.766 | -0.162 | 0.324 | 0.851(0.617~1.173) | |
| 吸烟史 [n(%)] | 0.570 | 0.070 | 0.673 | 1.073(0.773~1.489) | |
| 植入支架数(个) | 0.006 | 0.391 | 0.001 | 1.478(1.177~1.855) | |
| 基线空腹血糖(mmol/L) | 0.080 | 0.042 | 0.174 | 1.043(0.982~1.108) | |
| 基线期C反应蛋白(mg/L) | 0.064 | 0.006 | 0.007 | 1.006(1.002~1.011) | |
| 基线期eGFR[mL/(min·1.73 m2)] | 0.097 | -0.004 | 0.363 | 0.996(0.988~1.004) | |
| 随访期eGFR(mL/(min·1.73 m2)) | 0.038 | -0.010 | 0.022 | 0.990(0.982~0.999) | |
| [1] |
Ene-Iordache B, Perico N, Bikbov B, et al. Chronic kidney disease and cardiovascular risk in six regions of the world (ISN-KDDC): A cross-sectional study[J]. Lancet Glob Health, 2016, 4(5):e307-e319.
doi: 10.1016/S2214-109X(16)00071-1 URL |
| [2] |
Mathew RO, Bangalore S, Lavelle MP, et al. Diagnosis and management of atherosclerotic cardiovascular di-sease in chronic kidney disease: A review[J]. Kidney int, 2017, 91(4):797-807.
doi: S0085-2538(16)30625-1 pmid: 28040264 |
| [3] |
Keith DS, Nichols GA, Gullion CM, et al. Longitudinal follow-up and outcomes among a population with chronic kidney disease in a large managed care organization[J]. Arch Intern Med, 2004, 164(6):659-663.
doi: 10.1001/archinte.164.6.659 URL |
| [4] | Zhang L, Zhao MH, Zuo L, et al. China Kidney Disease Network (CK-NET) 2015 Annual Data Report[J]. Kidney Int Suppl, 2019, 9(1):e1-e81. |
| [5] | 国家心血管病中心. 中国心血管病报告2018[M]. 北京: 中国大百科全书出版社, 2018. |
| [6] |
Zhang L, Wang F, Wang L, et al. Prevalence of chronic kidney disease in China: A cross-sectional survey[J]. Lancet, 2012, 379(9818):815-822.
doi: 10.1016/S0140-6736(12)60033-6 URL |
| [7] | Zhang L, Wang H, Long J, et al. China Kidney Disease Network (CK-NET) 2014 Annual Data Report[J]. Am J kidney Dis, 2017, 69(6S2):A4. |
| [8] |
Ishimoto Y, Tanaka T, Yoshida Y, et al. Physiological and pathophysiological role of reactive oxygen species and reactive nitrogen species in the kidney[J]. Clin Exp Pharmacol Physiol, 2018, 45(11)1097-1105.
doi: 10.1111/1440-1681.13018 URL |
| [9] |
Spoto B, Pisano A, Zoccali C, et al. Insulin resistance in chronic kidney disease: a systematic review[J]. Am J Physiol Renal Physiol, 2016, 311(6):F1087-F1108.
doi: 10.1152/ajprenal.00340.2016 URL |
| [10] |
Horowitz B, Miskulin D, Zager P, et al. Epidemiology of hypertension in CKD[J]. Adv Chronic Kidney Dis, 2015, 22(2):88-95.
doi: 10.1053/j.ackd.2014.09.004 URL |
| [11] | 王芳, 章安迪. 伴有多种危险因素的冠心病患者支架内再狭窄的影响因素[J]. 诊断学理论与实践, 2016, 15(3):280-282. |
| [12] |
Welt FG, Rogers C. Inflammation and restenosis in the stent era[J]. Arterioscler Thromb Vasc Biol, 2002, 22(11):1769-1776.
doi: 10.1161/01.ATV.0000037100.44766.5B URL |
| [13] |
Gross ML, Meyer HP, Ziebart H, et al. Calcification of coronary intima and media: Immunohistochemistry, backscatter imaging, and X-ray analysis in renal and nonrenal patients[J]. Clin J Am Soc Nephrol, 2007, 2(1):121-134.
doi: 10.2215/CJN.01760506 URL |
| [14] |
Ishibashi M, Hiasa K, Zhao Q, et al. Critical role of monocyte chemoattractant protein-1 receptor CCR2 on monocytes in hypertension-induced vascular inflammation and remodeling[J]. Circ Res, 2004, 94(9):1203-1210.
pmid: 15059935 |
| [15] | 张瑞岩, 慢性肾病对冠心病发病和预后的影响[J]. 内科理论与实践, 2006, 3(2):94-98. |
| [16] |
Kaul U, Bhagwat A, Pinto B, et al. Paclitaxel-eluting stents versus everolimus-eluting coronary stents in a diabetic population: Two-year follow-up of the TUXEDO-India trial[J]. EuroIntervention, 2017, 13(10):1194-1201.
doi: 10.4244/EIJ-D-17-00333 URL |
| [17] |
Sedlis PS, Jurkovitz CT, Hartigan PM, et al. Optimal medical therapy with or without percutaneous coronary intervention for patients with stable coronary artery disease and chronic kidney disease[J]. Am J Cardiol, 2009, 104(12):1647-1653.
doi: 10.1016/j.amjcard.2009.07.043 URL |
| [18] |
Khalique O, Aronow WS, Ahn C, et al. Relation of moderate or severe reduction in glomerular filtration rate to number of coronary arteries narrowed >50% in patients undergoing coronary angiography for suspected coronary artery disease[J]. Am J Cardiol, 2007, 100(3):415-416.
pmid: 17659920 |
| [19] |
Rostand SG, Gretes JC, Kirk KA, et al. Ischemic heart disease in patients with uremia undergoing maintenance hemodialysis[J]. Kidney Int, 1979, 16(5):600-611.
doi: 10.1038/ki.1979.170 pmid: 548604 |
| [20] |
Schwarz U, Buzello M, Ritzet E, et al. Morphology of coronary atherosclerotic lesions in patients with end-stage renal failure[J]. Nephrol Dial Transplant, 2000, 15(2):218-223.
doi: 10.1093/ndt/15.2.218 URL |
| [21] | 曹立秀, 张欢, 肖华, 等. 中-重度肾功能不全患者冠状动脉病变的CT诊断研究[J]. 诊断学理论与实践, 2011, 10(6):523-526. |
| [22] |
Kato K, Yonetsu T, Jia H, et al. Nonculprit coronary plaque characteristics of chronic kidney disease[J]. Circ Cardiovasc imaging, 2013, 6(3):448-456.
doi: 10.1161/CIRCIMAGING.112.000165 URL |
| [1] | 王芳, 章安迪,. 伴有多种危险因素的冠心病患者支架内再狭窄的影响因素[J]. 诊断学理论与实践, 2016, 15(03): 280-282. |
| [2] | 杨帆, 李丽, 孙爱华, 马蔚芸, 陆怡德,. 基于半胱氨酸蛋白酶抑制素C建立的肾小球滤过率估算公式对于2型糖尿病患者肾功能的评估价值[J]. 诊断学理论与实践, 2012, 11(03): 290-294. |
| [3] | 张祎昀, 刘建民, 张翼飞, 郭永平, 薛冠华,. 2型糖尿病患者大血管病变临床相关因素的探讨[J]. 诊断学理论与实践, 2009, 8(06): 647-649. |
| [4] | 赵雅洁, 沈琳辉, 赵咏桔, 王巍, 林云,. 简化肾脏病膳食改良试验公式在血清肌酐值正常的老年男性群体中的应用[J]. 诊断学理论与实践, 2008, 7(02): 155-160. |
| [5] | 杨松涛, 左力, 王海燕,. 肾小球滤过率计算方程的正确评价[J]. 诊断学理论与实践, 2007, 6(06): 489-493. |
| [6] | 贾支俊, 冯雪凤, 申景涛, 郭万华,. ~(99m)Tc-DTPA肾小球滤过率与血清肌酐在评价狼疮肾炎中的价值[J]. 诊断学理论与实践, 2007, 6(04): 372-373. |
| [7] | 战玉喜, 李建新, 张峰, 王均梅, 郑楠,. 血清半胱氨酸蛋白酶抑制剂C对肾小球滤过功能受损的临床意义[J]. 诊断学理论与实践, 2006, 5(05): 437-438. |
| [8] | 汤兵,梅长林,张玲,章建全,孙田美,张树忠. 多囊肾病患者肾脏体积与临床表现关系的研究[J]. 诊断学理论与实践, 2003, 2(04): 43-45. |
| [9] | 史浩,陈楠,陈晓农,王伟铭,张文,徐耀文,任红,何新英. 检测肾小球滤过率的敏感方法:三碘三酰苯血浆清除率单点测定法[J]. 诊断学理论与实践, 2003, 2(04): 35-38. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||