诊断学理论与实践 ›› 2020, Vol. 19 ›› Issue (05): 516-520.doi: 10.16150/j.1671-2870.2020.05.013
马晓宇, 杨媛艳, 陆文丽( ), 倪继红, 王俊琪, 陈烨, 秦雪艳, 董治亚, 王伟
), 倪继红, 王俊琪, 陈烨, 秦雪艳, 董治亚, 王伟
MA Xiaoyu, YANG Yuanyan, LU Wenli(), NI Jihong, WANG Junqi, CHEN Ye, QIN Xueyan, DONG Zhiya, WANG Wei
摘要:
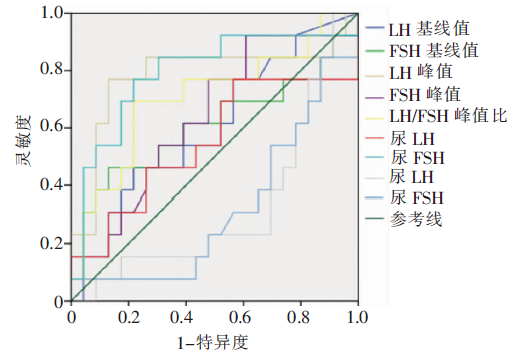
目的: 探寻临床鉴别慢进展型中枢性性早熟(slowly progressive central precocious puberty, SP-CPP)与快进展型中枢性性早熟(rapidly progressive central precocious puberty, RP-CPP)的方法。方法: 收集8岁前出现乳房发育的女童,行促黄体素释放素(lutropin hormone releasing hormone, LHRH)激发试验,定量检测血促黄体素(lutropin hormone, LH)、卵泡刺激素(follicle-stimulating hormone, FSH),同时采用定量试剂盒测定晨尿中LH和FSH。受检测者中53例被诊断为中枢性性早熟(central precocious puberty,CPP)。随访半年后观察其发育进展情况(生长速率、骨龄及第二性征发育等),分为SP-CPP(30例)和RP-CPP(23例)2组,比较分析2组间初诊时血和尿的LH、FSH以及相关参数的差异。结果: 初诊血LH峰值、血LH 峰值/FSH峰值比(以下简称LH/FSH峰值比)及晨尿FSH水平在鉴别SP-CPP与RP-CPP中有一定的临床应用价值,而晨尿LH及晨尿LH/晨尿FSH比值在2组间差异均无统计学意义。与SP-CPP组相比,RP-CPP组具有较高的血LH峰值[(18.06±3.68)IU/L比(7.58±2.50)IU/L,P<0.001]和LH/FSH峰值比[1.67±1.08比0.97±0.43,P=0.014],而其晨尿FSH则低于SP-CPP组[(4.34±1.52)IU/L比(7.60±1.20)IU/L, P=0.007]。根据受试者操作特征曲线(receiver operator characteristic curve,ROC曲线)分析,血LH峰值的临界值为9.68 IU/L时,大于等于该值时鉴别RP-CPP与SP-CPP的灵敏度为76.9%,特异度为87.0%;血LH/FSH峰值比的临界值为1.24,大于等于该值时,其鉴别两者的灵敏度为69.2%,特异度为73.9%;晨尿FSH的临界值为5.91 IU/L,大于等于该值时,其鉴别两者的灵敏度(76.9%)及特异度(78.3%)与血指标检测结果相似。结论: 测定晨尿促性腺激素是一种无创且较可靠的方法,初诊时检测晨尿FSH,对早期CPP分型诊断有一定的辅助意义。
中图分类号: