诊断学理论与实践 ›› 2024, Vol. 23 ›› Issue (05): 542-549.doi: 10.16150/j.1671-2870.2024.05.012
徐鹏宇, 迟骋, 张晓霞( )
)
收稿日期:2024-03-20
接受日期:2024-08-20
出版日期:2024-10-25
发布日期:2025-02-25
通讯作者:
张晓霞 E-mail:jtr2007@sina.com
XU Pengyu, CHI Cheng, ZHANG Xiaoxia()
Received:2024-03-20
Accepted:2024-08-20
Published:2024-10-25
Online:2025-02-25
摘要:
肺部超声(lung ultrasound,LUS)检查因无辐射、低成本、实时成像、床旁可操作且无转运风险,在急诊重症监护病房患者的诊疗中具有重要的应用价值。LUS使用B型和M型模式评估肺部病变,使用LUS评分量化“B线”和评估病变程度,提供了一个系统且客观的病变评价体系。自2008年以来,法国重症医学家Lichtenstein等提出的急诊床旁LUS检查(bedside lung ultrasonography in emergency, BLUE)方案及其后续改良的BLUE(bedside lung ultrasonography in emergency-plus, BLUE-plus)方案在评估急性呼吸衰竭中取得了显著成果。BLUE方案通过不同的超声表现类型区分呼吸困难病因,诊断心源性肺水肿的灵敏度为97%,特异度为95%;诊断肺炎的灵敏度为89%,特异度为94%。BLUE-plus方案增加了后背区域扫描,将诊断肺不张和肺实变的灵敏度提升至95.71%,特异度为87.50%。凭借LUS检查中的“胸膜滑动征”和“B线”等指标,诊断肺水肿的灵敏度可达96%,远超胸部X线(chest X-ray, CXR)检查65%的灵敏度,还可区分心源性与非心源性肺水肿。LUS检查诊断胸腔积液的灵敏度达92%,并能估算积液量。对于肺实变,LUS检查表现出80%~90%的灵敏度和70%~90%的特异度,显著优于CXR的灵敏度(53%)和特异度(78%)。对于气胸,LUS检查的诊断特异度接近100%,且能进行半定量分析。LUS在重症患者的治疗监测中展现出广泛的应用价值。在机械通气患者的肺通气变化评估中,LUS能通过检测“A线”到“B线”再到“组织样征”的转变来评估肺复张情况,且LUS评分与计算机断层扫描(computed tomography, CT)结果高度相关(Rho=0.85,P<0.01)。重症患者的容量管理中,可使用LUS检测“B线”来评估液体超负荷情况,与超声心动图联合使用时,可帮助判断患者是否具有容量反应性。对于呼吸机相关性肺炎(ventilator-associated pneumonia, VAP)和急性呼吸窘迫综合征(acute respiratory distress syndrome, ARDS),LUS不仅有助于诊断,还能评估病情的严重度及疗效。LUS的应用目前仍面临操作者技术的挑战,且存在一定局限性,包括操作者经验的依赖、肺部深度探测的限制、肥胖或胸部术后患者的LUS图像质量较差等问题。未来,结合人工智能技术有望进一步提升LUS的诊断准确率和效率。
中图分类号:
徐鹏宇, 迟骋, 张晓霞. 床旁肺部超声及改良方案在急诊重症监护病房患者肺部病变诊断及监测中的应用进展[J]. 诊断学理论与实践, 2024, 23(05): 542-549.
XU Pengyu, CHI Cheng, ZHANG Xiaoxia. Application progress of BLUE and modified protocols in diagnosing and monitoring pulmonary lesions in EICU patients[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(05): 542-549.
表1
B型模式和M型模式的评价指标
| 模式 | 监测指标 | 临床意义 |
|---|---|---|
| B型 | A线 | 正常肺组织回声; 加重的慢性阻塞性肺疾病或重度急性哮喘 |
| B线 | 肺水肿和间质性肺炎 | |
| 肺搏动征 | 肺实变 | |
| 胸膜滑动征 | 肺通气 | |
| 窗帘征 | 肺下界活动度 | |
| 碎片征 | 肺实变 | |
| 动态支气管充气征 | 实变肺组织内气道通畅性 | |
| 静态支气充气征 | 阻塞性肺不张 | |
| 胸膜搏动征 | 排除气胸 | |
| M型 | 沙滩征 | 正常肺通气 |
| 平流层征 | 胸膜无相对运动 | |
| 肺点征 | 气胸 |

图1
急诊床旁肺部超声检查(BLUE方案)[6] 1. 上蓝点; 2. 下蓝点; 3. 后外侧肺泡和(或)胸膜综合征点 (PLAPS); 4. 膈肌点
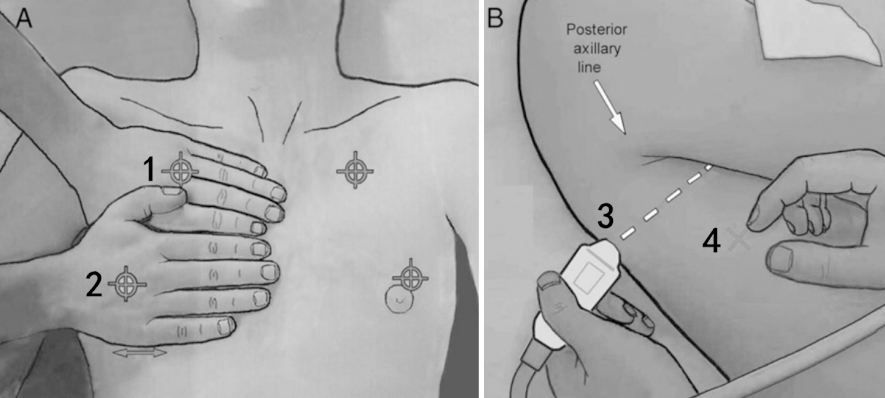
图2
BLUE方案决策树[6] COPD:慢性阻塞性肺病。
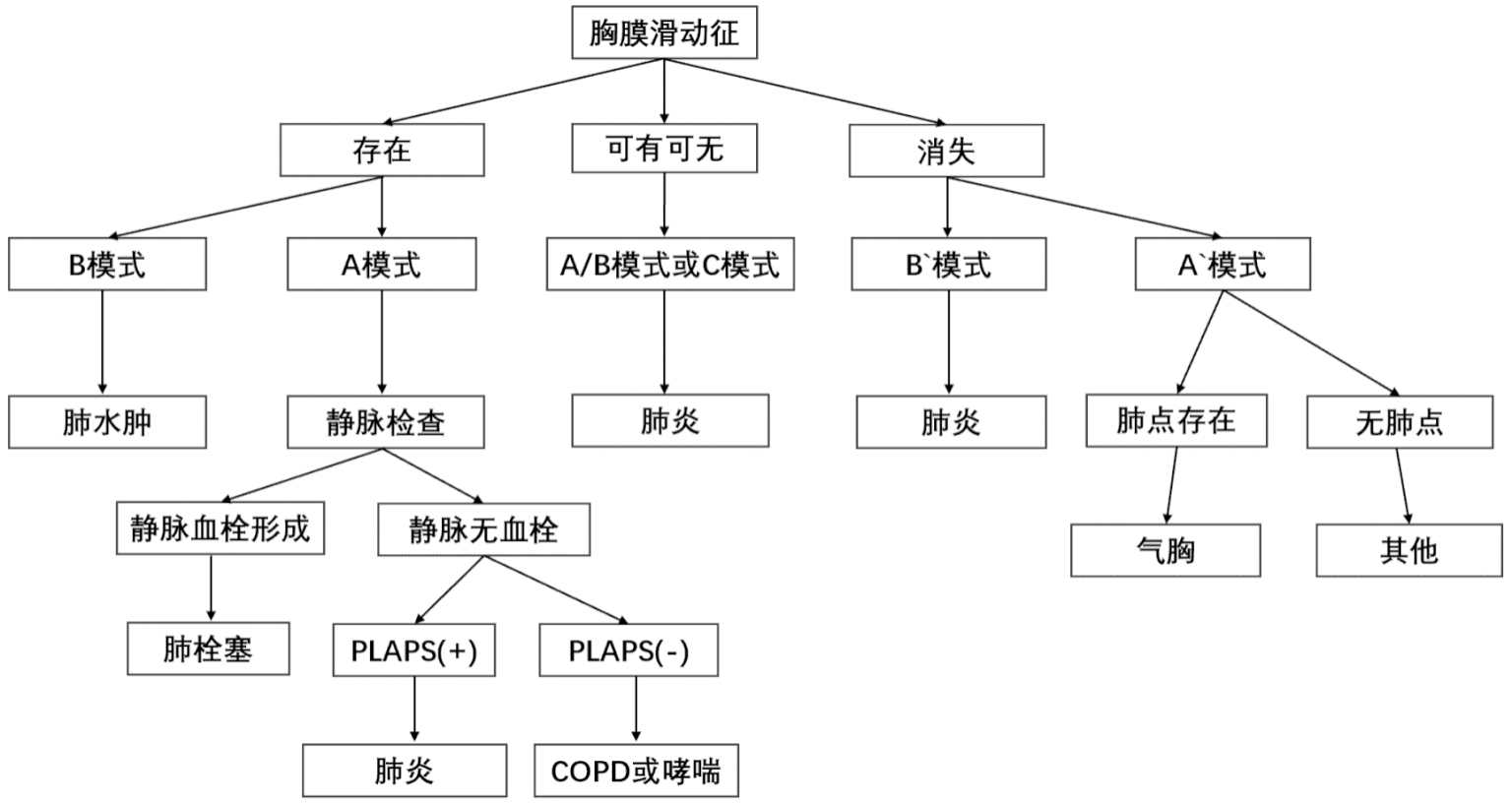
图3
ABCDE-LUS方案[8] COPD:慢性阻塞性肺病。
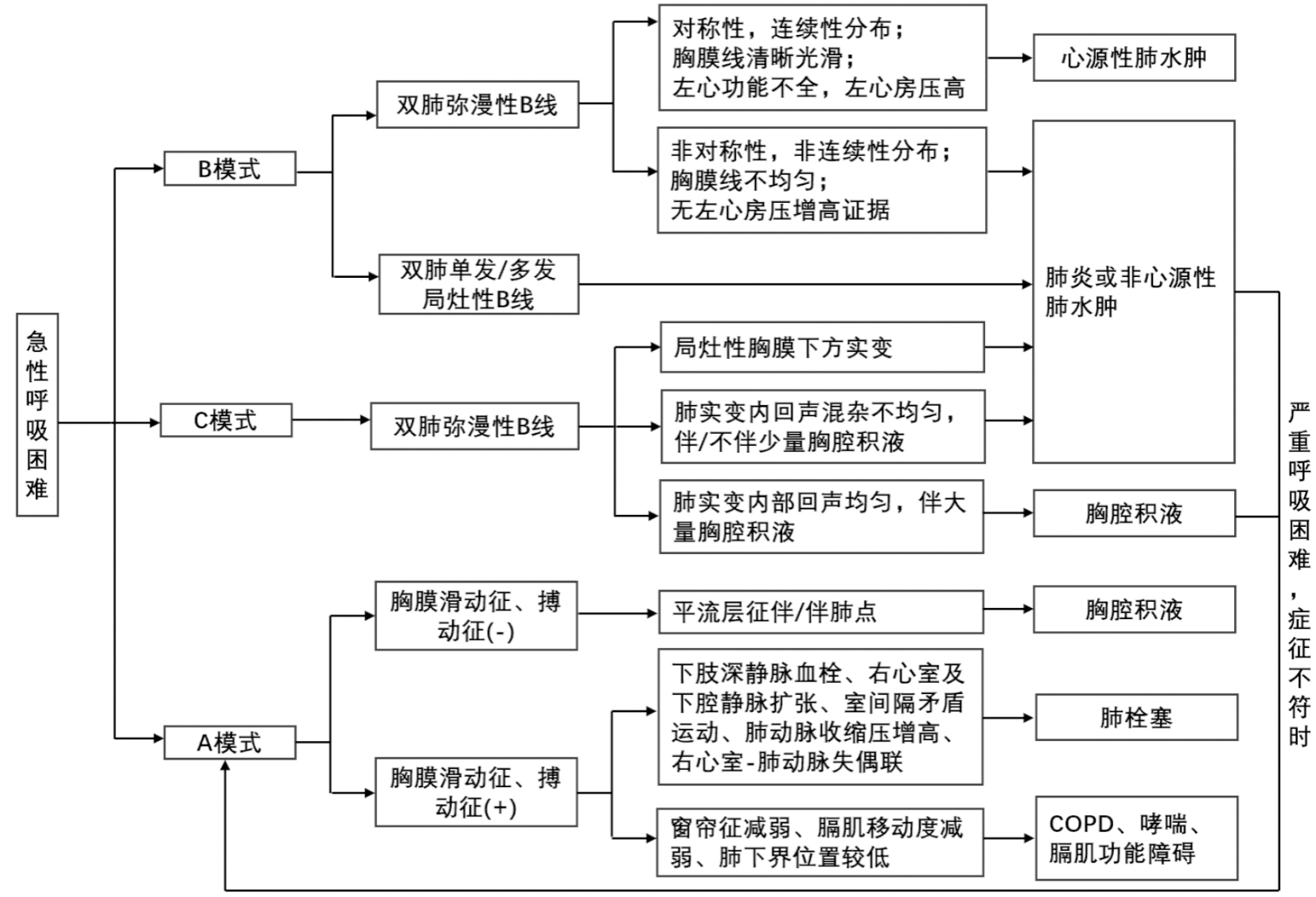
表2
临床肺部感染评分[30]
| 1.体温,℃ |
|---|
| ≥36.5, ≤38.4 = 0分 |
| ≥38.5, ≤38.9 = 1分 |
| ≥39.0或≤36.0 = 2分 |
| 2.白细胞计数,mm-3 |
| ≥4 000, ≤11 000 = 0分 |
| <4 000或>11 000 = 1分 |
| <4 000或>11 000 + 杆状核 ≥500 = 2分 |
| 3.气管分泌物 |
| <14+ 气管分泌物 = 0分 |
| ≥14+ 气管分泌物 = 1分 |
| ≥14+ 气管分泌物 + 脓性分泌物 = 2分 |
| 4.氧合指数:PaO2/FiO2, mmHg |
| >240或ARDS = 0分 |
| ≤ 240且无ARDS证据 = 2分 |
| 5.肺部影像学 |
| 无浸润 = 0分 |
| 弥漫性(或斑片) 浸润 = 1分 |
| 局限性浸润 = 2分 |
| 6.气管抽吸物培养(半定量: 0,1+, 2+ or 3+) |
| 培养致病菌 ≤ 1+ 或未生长 = 0分 |
| 培养致病菌>1+ = 1分 |
| 培养致病菌>1+且革兰染色发现相同致病菌>1+ = 2分 |
| [1] | BREITKOPF R, TREML B, RAJSIC S. Lung Sonography in critical care medicine[J]. Diagnostics (Basel), 2022, 12(6):1405. |
| [2] | GARCÍA-DE-ACILU M, SANTAFÉ M, ROCA O. Use of thoracic ultrasound in acute respiratory distress syndrome[J]. Ann Transl Med, 2023, 11(9):320. |
| [3] | KWACK W G, YUN M, LEE D S, et al. Effectiveness of intrahospital transportation of mechanically ventilated patients in medical intensive care unit by the rapid response team: A cohort study[J]. Medicine (Baltimore), 2018, 97(48):e13490. |
| [4] |
CHRZAN R, POLOK K, ANTCZAK J, et al. The value of lung ultrasound in COVID-19 pneumonia, verified by high resolution computed tomography assessed by artificial intelligence[J]. BMC Infect Dis, 2023, 23(1):195.
doi: 10.1186/s12879-023-08173-4 pmid: 37003997 |
| [5] | MOJOLI F, BOUHEMAD B, MONGODI S, et al. Lung ultrasound for critically ill patients[J]. Am J Respir Crit Care Med, 2019, 199(6):701-714. |
| [6] |
LICHTENSTEIN D A. BLUE-protocol and FALLS-protocol: two applications of lung ultrasound in the critically ill[J]. Chest, 2015, 147(6):1659-1670.
doi: S0012-3692(15)37223-8 pmid: 26033127 |
| [7] |
ROCCA E, ZANZA C, LONGHITANO Y, et al. Lung ultrasound in critical care and emergency medicine: clinical review[J]. Adv Respir Med, 2023, 91(3):203-223.
doi: 10.3390/arm91030017 pmid: 37218800 |
| [8] | 河北省医学会超声分会, 河北省医师协会超声医师分会, 河北省超声医学质量管理与控制中心, 等. 急性呼吸困难床旁肺超声诊断规范专家建议[J]. 疑难病杂志, 2024, 23(3):257-265. |
| Hebei Provincial Medical Association Ultrasound Branch, Hebei Provincial Physicians Association Ultrasonographers Branch, Hebei Provincial Ultrasound Quality Management and Control Center, et al. Expert advice on the standardization of bedside lung ultrasound diagnosis of acute respiratory distress[J]. Chin J Difficult Complicated Cases, 2024, 23(3):257-265. | |
| [9] | DEMI L, WOLFRAM F, KLERSY C, et al. New International Guidelines and Consensus on the Use of Lung Ultrasound[J]. J Ultrasound Med, 2023, 42(2):309-344. |
| [10] |
DENG Q, ZHANG Y, WANG H, et al. Semiquantitative lung ultrasound scores in the evaluation and follow-up of critically ill patients with COVID-19: a single-center study[J]. Acad Radiol, 2020, 27(10):1363-1372.
doi: 10.1016/j.acra.2020.07.002 pmid: 32713715 |
| [11] | 王小亭, 刘大为, 张宏民, 等. 改良床旁肺部超声评估方案对重症患者肺实变和肺不张的诊断价值[J]. 中华内科杂志, 2012, 51(12):948-951. |
| WANG X T, LIU D W, ZHANG H M, et al. The value of bedside lung ultrasound in emergency-plus protocol for the assessment of lung consolidation and atelectasis in critical patients[J]. Chin J Int Med, 2012, 51(12):948-951. | |
| [12] |
WOOTEN W M, SHAFFER L E T, HAMILTON L A. Bedside ultrasound versus chest radiography for detection of pulmonary edema: A prospective cohort study[J]. J Ultrasound Med, 2019, 38(4):967-973.
doi: 10.1002/jum.14781 pmid: 30280401 |
| [13] |
CORTELLARO F, CERIANI E, SPINELLI M, et al. Lung ultrasound for monitoring cardiogenic pulmonary edema[J]. Intern Emerg Med, 2017, 12(7):1011-1017.
doi: 10.1007/s11739-016-1510-y pmid: 27473425 |
| [14] |
PIVETTA E, GOFFI A, NAZERIAN P, et al. Lung ultrasound integrated with clinical assessment for the diagnosis of acute decompensated heart failure in the emergency department: a randomized controlled trial[J]. Eur J Heart Fail, 2019, 21(6):754-766.
doi: 10.1002/ejhf.1379 pmid: 30690825 |
| [15] | ENGHARD P, RADEMACHER S, NEE J, et al. Simplified lung ultrasound protocol shows excellent prediction of extravascular lung water in ventilated intensive care patients[J]. Crit Care, 2015, 19(1):36. |
| [16] | 蒙伟宇, 张驰, 胡军涛, 等. 基于肺部超声影像组学分析联合机器学习评估重症患者血管外肺水指数[J]. 中华危重病急救医学, 2023, 35(10):1074-1079. |
| MENG W Y, ZHANG C, HU J T, et al. Evaluation of extravascular lung water index in critically ill patients based on lung ultrasound radiomics analysis combined with machine learning[J]. Chin Crit Care Med, 2023, 35(10):1074-1079. | |
| [17] |
MAYO P H, COPETTI R, FELLER-KOPMAN D, et al. Thoracic ultrasonography: a narrative review[J]. Intensive Care Med, 2019, 45(9):1200-1211.
doi: 10.1007/s00134-019-05725-8 pmid: 31418060 |
| [18] |
IBITOYE B O, IDOWU B M, OGUNROMBI A B, et al. Ultrasonographic quantification of pleural effusion: comparison of four formulae[J]. Ultrasonography, 2018, 37(3):254-260.
doi: 10.14366/usg.17050 pmid: 29228764 |
| [19] | HANSELL L, MILROSS M, DELANEY A, et al. Lung ultrasound has greater accuracy than conventional respiratory assessment tools for the diagnosis of pleural effusion, lung consolidation and collapse: a systematic review[J]. J Physiother, 2021, 67(1):41-48. |
| [20] | LLAMAS-ÁLVAREZ A M, TENZA-LOZANO E M, LATOUR-PÉREZ J. Accuracy of lung ultrasonography in the diagnosis of pneumonia in adults: systematic review and meta-analysis[J]. Chest, 2017, 151(2):374-382. |
| [21] | SMIT M R, HAGENS L A, HEIJNEN N F L, et al. Lung ultrasound prediction model for acute respiratory distress syndrome: a multicenter prospective observational study[J]. Am J Respir Crit Care Med, 2023, 207(12):1591-1601. |
| [22] |
VOLPICELLI G, BOERO E, SVERZELLATI N, et al. Semi-quantification of pneumothorax volume by lung ultrasound[J]. Intensive Care Med, 2014, 40(10):1460-1467.
doi: 10.1007/s00134-014-3402-9 pmid: 25056671 |
| [23] | CHAN K K, JOO D A, MCRAE A D, et al. Chest ultrasonography versus supine chest radiography for diagnosis of pneumothorax in trauma patients in the emergency department[J]. Cochrane Database Syst Rev, 2020, 7(7):CD013031. |
| [24] | COSTAMAGNA A, STEINBERG I, PIVETTA E, et al. Clinical performance of lung ultrasound in predicting time-dependent changes in lung aeration in ARDS patients[J]. J Clin Monit Comput, 2023, 37(2):473-480. |
| [25] |
BOUHEMAD B, LIU Z H, ARBELOT C, et al. Ultrasound assessment of antibiotic-induced pulmonary reaeration in ventilator-associated pneumonia[J]. Crit Care Med, 2010, 38(1):84-92.
doi: 10.1097/CCM.0b013e3181b08cdb pmid: 19633538 |
| [26] | BEAUBIEN-SOULIGNY W, RHÉAUME M, BLONDIN M C, et al. A simplified approach to extravascular lung water assessment using point-of-care ultrasound in patients with end-stage chronic renal failure undergoing hemodialysis[J]. Blood Purif, 2018, 45(1-3):79-87. |
| [27] | ROMANO M, VIANA E, MARTINS J D, et al. Evaluation of congestion levels in septic patients admitted to critical care units with a combined venous excess-lung ultrasound score (VExLUS) - a research protocol[J]. POCUS J, 2023, 8(1):93-98. |
| [28] |
INNOCENTI F, SAVINELLI C, COPPA A, et al. Integrated ultrasonographic approach to evaluate fluid responsiveness in critically ill patients[J]. Sci Rep, 2023, 13(1):9159.
doi: 10.1038/s41598-023-36077-5 pmid: 37280235 |
| [29] | WANG G, JI X, XU Y, et al. Lung ultrasound: a promising tool to monitor ventilator-associated pneumonia in critically ill patients[J]. Crit Care, 2016, 20(1): 320. |
| [30] | 李黎明, 李莲花, 关键, 等. 肺部超声评分在呼吸机相关性肺炎疗效评价中的作用[J]. 中华内科杂志, 2016, 55(12):950-952. |
| LI L M, LI L H, GUAN J, et al. The value of lung ultrasound score for therapeutic effect assessment of ventilator-associated pneumonia[J]. Chin J Int Med, 2016, 55(12):950-952. | |
| [31] | BOUHEMAD B, DRANSART-RAYÉ O, MOJOLI F, et al. Lung ultrasound for diagnosis and monitoring of ventilator-associated pneumonia[J]. Ann Transl Med, 2018, 6(21): 418. |
| [32] | MATTHAY M A, ARABI Y, ARROLIGA A C, et al. A new global definition of acute respiratory distress syndrome[J]. Am J Respir Crit Care Med, 2024, 209(1):37-47. |
| [33] | VOLPICELLI G, FRACCALINI T, CARDINALE L, et al. Feasibility of a new lung ultrasound protocol to determine the extent of lung injury in COVID-19 pneumonia[J]. Chest, 2023, 163(1):176-184. |
| [34] |
ZHANG H, LIU Z, SHU H, et al. Prone positioning in ARDS patients supported with VV ECMO, what we should explore?[J]. J Intensive Care, 2022, 10(1):46.
doi: 10.1186/s40560-022-00640-5 pmid: 36195935 |
| [35] |
WANG R, QI B, ZHANG X, et al. Prophetic values of lung ultrasound score on post-extubation distress in patients with acute respiratory distress syndrome[J]. Eur J Med Res, 2022, 27(1):27.
doi: 10.1186/s40001-022-00652-9 pmid: 35193686 |
| [36] | 郑秋咪, 何燕莲, 李玄丹, 等. 血清自分泌运动因子水平及肺部超声评分与ARDS患者病情及28天死亡的关系[J]. 中华结核和呼吸杂志, 2023, 46(1):40-45. |
| ZHENG Q M, HE Y L, LI X D, et al. Correlation between serum autotaxin level and pulmonary ultrasound score with the disease severity and 28-day mortality in patients with acute respiratory disease syndrome[J]. Chin J Tuberc Respir Dis, 2023, 46(1):40-45. |
| [1] | 冯原, 何钊, 孙青芳, 孙伯民, 严福华, 杨广中. 磁共振介入成像及其临床应用进展[J]. 诊断学理论与实践, 2024, 23(02): 108-113. |
| [2] | 王砚春, 卢仁泉. 出凝血检测在肿瘤患者中的应用价值探讨[J]. 诊断学理论与实践, 2023, 22(04): 341-347. |
| [3] | 游利. 重视骨转换指标的临床应用及评估[J]. 诊断学理论与实践, 2020, 19(03): 214-218. |
| [4] | 陈辰, 张月, 胡晓波. 尿路感染报警信息阈值设置和临床应用评价[J]. 诊断学理论与实践, 2020, 19(02): 168-171. |
| [5] | 余红, 王一飞, 陈佳, 陈洁, 李斌. 青蒿素及其衍生物在皮肤疾病中的作用机制研究及临床应用[J]. 诊断学理论与实践, 2019, 18(2): 233-236. |
| [6] | 上海市医学会分子诊断专科分会, 上海市临床检验中心, 上海东方肝胆外科医院, 中华医学会检验医学分会临床免疫学组, 中国中西医结合检验学会肝病学术委员会, 全军肝胆外科专业委员会, 上海免疫学会肿瘤免疫分会, 上海抗癌协会肿瘤标志物分会. 多学科甲胎蛋白异质体临床应用专家共识[J]. 诊断学理论与实践, 2018, 17(01): 19-24. |
| [7] | 朱巍巍, 万颖蕾, 刘锦燕, 张华, 陈华, 项明洁. 内毒素的检测方法与临床应用进展[J]. 诊断学理论与实践, 2017, 16(06): 668-671. |
| [8] | 彭奕冰, 章黎华. 免疫球蛋白游离轻链的检测与临床应用[J]. 诊断学理论与实践, 2017, 16(05): 468-471. |
| [9] | 沈立松, 马妍慧,. 质谱技术在检验医学中的应用现状和前景[J]. 诊断学理论与实践, 2012, 11(05): 536-538. |
| [10] | 李彪,朱承谟. 正电子放射性药物的临床应用与进展[J]. 诊断学理论与实践, 2005, 4(02): 93-95. |
| [11] | 朱承谟. 积极开展PET、SPECT显像的临床应用和研究[J]. 诊断学理论与实践, 2005, 4(02): 89-90. |
| [12] | 王鸿利. 血液学实验诊断的现状特点与应用价值[J]. 诊断学理论与实践, 2004, 3(06): 5-7. |
| [13] | 康熙雄,王雅杰,张锟. 蛋白质组学及其临床应用[J]. 诊断学理论与实践, 2004, 3(05): 14-16. |
| [14] | 崔丽英. 肌电图的临床应用现状与进展[J]. 诊断学理论与实践, 2004, 3(02): 67-69. |
| [15] | 刘学键 ,李世正,陆民,秦中平 ,李克雷. 四肢血管畸形的影像学检查临床应用评价[J]. 诊断学理论与实践, 2002, 1(04): 51-52. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||