诊断学理论与实践 ›› 2024, Vol. 23 ›› Issue (01): 57-66.doi: 10.16150/j.1671-2870.2024.01.008
朱霞, 王昕, 金晶晶, 肖立( )
)
收稿日期:2023-07-11
出版日期:2024-02-25
发布日期:2024-05-30
通讯作者:
肖立,E-mail:fangjx0207@foxmail.com
ZHU Xia, WANG Xin, JIN Jingjing, XIAO Li()
Received:2023-07-11
Published:2024-02-25
Online:2024-05-30
摘要:
目的:研究病灶最大径≤1 cm肺腺癌患者EGFR、ALK及ROS1基因状态。方法:收集2013年1月至2020年10月经华东医院病理科确诊为肺腺癌且病灶最大径≤1 cm,并行表皮生长因子受体(epidermal growth factor receptor, EGFR)、间变性淋巴瘤激酶(anaplastic lymphoma kinase, ALK)和(或)原癌基因酪氨酸蛋白激酶ROS(ROS proto-oncogene 1, receptor tyrosine kinase, ROS1)检测的患者的临床病理资料,回顾性分析其EGFR、ALK、ROS1基因状态及其临床病理学特点。结果:纳入1 232例病灶最大径≤1 cm肺腺癌患者,平均年龄54岁,男性387例,女性845例;多发病灶患者只选1个病灶。本组原位腺癌182例(14.8%),微浸润性腺癌778例(63.1%),浸润性非黏液性腺癌249例(20.2%),浸润性黏液腺癌23例(1.9%)。43.1%(352/817例)存在EGFR基因突变,其中46.9%(165/352例)为21L858R突变,40.6%(143/352例)为19Del突变,0.9%(3/352例)为18G719X/20S768I和21L858R/20S768I双突变。原位腺癌、微浸润性腺癌、浸润性非黏液性腺癌、浸润性黏液腺癌患者的EGFR突变率分别为31.0%(40/129)、42.0%(208/495)、58.4%(104/178)、0(0/15)。23.1%(3/13例)同一患者不同病灶EGFR突变检测结果不同(13例先后发生肺腺癌2灶,其中2例首次术后病灶为19Del突变阳性,第2次手术病灶示EGFR野生型;1例首次术后病灶为EGFR野生型,第2次病灶显示21L858R突变型)。EGFR位点突变率与组织学类型、年龄相关,>60岁年龄者及浸润性非黏液性腺癌者突变率高,而与性别、吸烟无关。1.9%(22/1168例)ALK基因重排阳性,浸润性非黏液性腺癌(5.2%)及≤60岁年龄组2.6%)患者中阳性率高,含实性成分的腺癌ALK重排阳性率(22.2%,4/18)明显高于浸润性非黏液腺癌的阳性率(5.2%,12/233)和不含实性成分的腺癌(1.1%,12/1095)(P<0.05),且与性别、吸烟无关。0.8%(6/795例)的患者ROS1基因重排阳性,阳性率与性别、年龄、吸烟、组织学类型无关。382例患者同时检测EGFR、ALK、ROS1,其中40.6%(155/382)的肿瘤含此三者中一种突变或基因重排,未发现其中两者或三者共存现象。结论:本次单中心研究显示,病灶最大径≤1 cm的肺腺癌中,微浸润腺癌占多数(63.1%);至少40%存在EGFR、ALK、ROS1三者之一基因突变或重排改变,三者均与性别、吸烟无关。EGFR突变以21L858R和19Del最常见,在>60岁的患者及浸润性非黏液性腺癌患者中发生率高。ALK重排阳性率在60岁以下的患者及含实性成分的腺癌中高。最大径≤1 cm肺脉癌病灶中ROS1重排阳性率低。同一患者不同病灶间的分子检测结果可存在差异,对于多发病灶有必要分别进行多分子检测。
中图分类号:
朱霞, 王昕, 金晶晶, 肖立. 1 232例病灶最大径≤1 cm肺腺癌EGFR、ALK、ROS1基因状态及临床病理特征的回顾分析研究[J]. 诊断学理论与实践, 2024, 23(01): 57-66.
ZHU Xia, WANG Xin, JIN Jingjing, XIAO Li. Analysis of relationship between gene status (EGFR, ALK, ROS1)and clinicopathological features in 1 232 cases of lung adenocarcinoma with lesion of maximum diameter≤1 cm[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(01): 57-66.
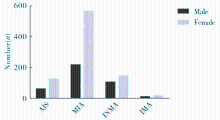
图1
1 232例病灶≤1 cm肺腺癌病理分型 AIS: 原位腺癌(adenocarcinoma in situ);MIA:微浸润性腺癌(minimal invasive adenocarcinoma);INMA:浸润性腺癌(invasive non-mucinous adenocarcinoma); IMA:黏液性腺癌(invasive mucinous adenocarcinoma)
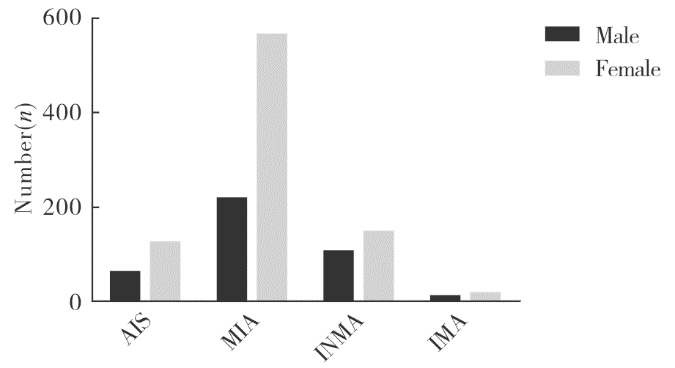
图2
352例EGFR突变阳性病例中不同突变位点比较
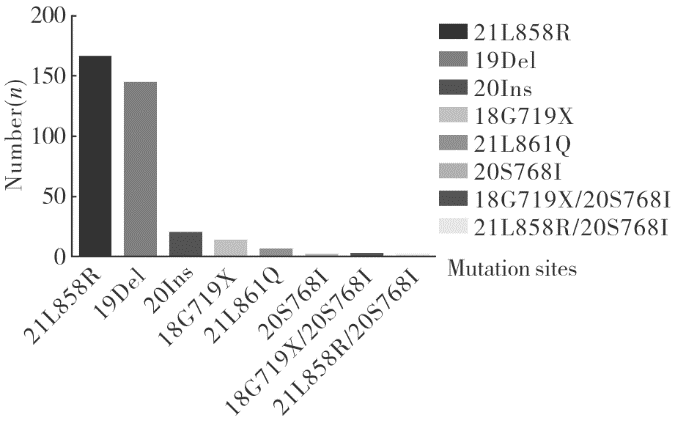
表1
352例 EGFR突变阳性患者突变类型及临床病理特征
| Clinical characteristics | L858R | 19Del | 20Ins | G719X | L861Q | S768I | G719X/S768I | L858R/S768I | 总计 |
|---|---|---|---|---|---|---|---|---|---|
| Total cases (%) | 165(46.9) | 143(40.6) | 20(5.7) | 14(4.0) | 6(1.7) | 1(0.3) | 2(0.6) | 1(0.3) | 352 |
| Sex | |||||||||
| M | 51 | 44 | 4 | 5 | 2 | 0 | 0 | 0 | 106 |
| F | 114 | 99 | 16 | 9 | 4 | 1 | 2 | 1 | 246 |
| Age/year | |||||||||
| ≤60 | 79 | 97 | 15 | 8 | 5 | 1 | 1 | 1 | 207 |
| >60 | 86 | 46 | 5 | 6 | 1 | 0 | 1 | 0 | 145 |
| Smoke | |||||||||
| Yes | 5 | 5 | 2 | 0 | 1 | 0 | 0 | 0 | 13 |
| No | 160 | 138 | 18 | 14 | 5 | 1 | 2 | 1 | 339 |
| Histologic type | |||||||||
| AIS | 11 | 23 | 3 | 1 | 2 | 0 | 0 | 0 | 40 |
| MIA | 102 | 76 | 15 | 10 | 2 | 1 | 1 | 1 | 208 |
| INMA | 52 | 44 | 2 | 3 | 2 | 0 | 1 | 0 | 104 |
| IMA | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
表2
817例行EGFR基因检测且病灶≤1 cm肺腺癌临床病理特征
| Clinical characteristics | Mutant type | Wild type | Mutation rate | P |
|---|---|---|---|---|
| Total cases | 352 | 465 | 43.1% | |
| Sex | ||||
| M | 106 | 155 | 40.6% (106/261) | 0.328 |
| F | 246 | 310 | 44.2% (246/556) | |
| Age/year | ||||
| ≤60 | 207 | 337 | 38.1% (207/544) | 0.001 |
| >60 | 145 | 128 | 53.1% (145/273) | |
| Smoke | ||||
| Yes | 13 | 17 | 43.3% (13/30) | 0.978 |
| No | 339 | 448 | 43.1% (339/787) | |
| Histologic type | ||||
| AIS | 40 | 89 | 31.0% (40/129) | 0.001 |
| MIA | 208 | 287 | 42.0% (208/495) | |
| INMA | 104 | 74 | 58.4% (104/178) | |
| IMA | 0 | 15 | 0 (0/15) |
表3
3例EGFR多位点突变共存患者的临床病理特征
| Case | Mutation site | Sex | Age | Smoke | Histologic type | Lymph node metastasis |
|---|---|---|---|---|---|---|
| A | G719X/S768I | F | 62 | No | INMA | No |
| B | G719X/S768I | F | 49 | No | MIA | No |
| C | L858R/S768I | F | 25 | No | MIA | No |
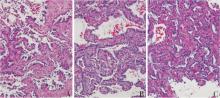
图3
EGFR双位点突变病理组织学特点(HE, ×200) 病例A示腺泡为主,局灶可见丝状微乳头结构。病例B示浸润区域主要为腺泡结构,局灶可见乳头结构。病例C示贴壁生长为主,局灶可见腺泡结构。
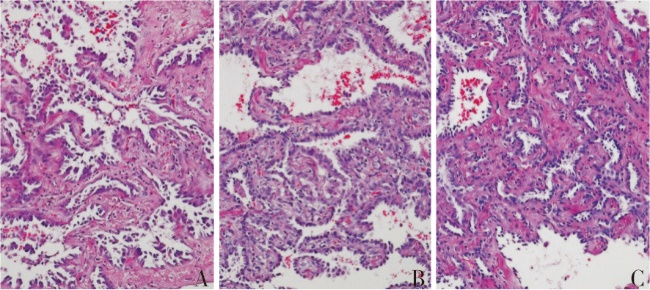
表4
1 168例行ALK重排检测且病灶大小≤1 cm肺腺癌患者的临床病理特征
| Clinical characteristics | Positive | Negative | Positive rate | P |
|---|---|---|---|---|
| Total cases | 22 | 1146 | 1.9% | |
| Sex | ||||
| M | 3 | 368 | 0.8% (3/371) | 0.065 |
| F | 19 | 778 | 2.4% (19/797) | |
| Age/year | ||||
| ≤60 | 20 | 735 | 2.6% (20/755) | 0.009 |
| >60 | 2 | 411 | 0.5% (2/413) | |
| Smoke | ||||
| Yes | 0 | 43 | 0(0/43) | 1.000 |
| No | 22 | 1103 | 2.0% (2/1125) | |
| Histologic type | ||||
| AIS | 1 | 169 | 0.6% (1/170) | 0.003 |
| MIA | 9 | 733 | 1.2% (9/742) | |
| INMA | 12 | 221 | 5.2% (12/233) | |
| IMA | 0 | 23 | 0 (0/23) |
表5
22例ALK重排阳性病例临床病理特点
| Sex | Number of cases |
|---|---|
| M | 3 |
| F | 19 |
| Age/year | |
| ≤60 | 20 |
| >60 | 2 |
| Smoke | |
| Yes | 0 |
| No | 22 |
| Histologic type | |
| AIS | 1 |
| MIA | 9 |
| INMA | 12 |
| IMA | 0 |
| Histological features | |
| Contains micropapillary component | 2 |
| Contains solid components | 4 |
| Contains micropapillary/solid components | 4 |
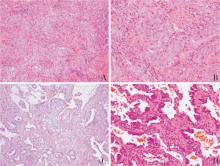
图4
ALK基因重排阳性病例病理形态学特征(HE) A:浸润性非黏液性腺癌,实性生长为主,低倍镜下肿瘤细胞呈巢状分布,未见明显腺样结构(×100);B:中倍镜放大显示肿瘤细胞核圆形或卵圆形,可见核仁,肿瘤细胞巢中央可见坏死(×200);C:腺泡及筛状腺体(×100);D:肿瘤细胞大部分区贴壁生长,局灶见微乳头结构凸起(×200)。
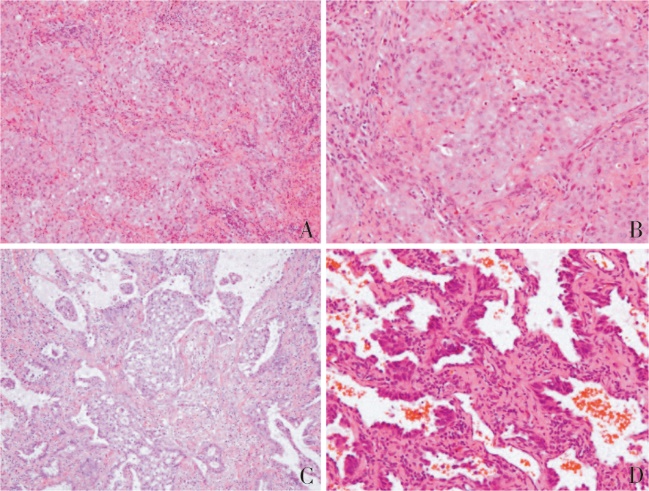
表6
795例病灶≤1 cm肺腺癌ROS1重排检测患者临床病理特征
| Clinical characteristics | Positive | Negative | Positive rate | P |
|---|---|---|---|---|
| Total cases | 6 | 789 | 0.8% (6/795) | |
| Sex | ||||
| M | 1 | 252 | 0.4% (1/253) | 0.671 |
| F | 5 | 537 | 0.9% (5/542) | |
| Age/year | ||||
| ≤60 | 4 | 495 | 0.8% (4/499) | 1.000 |
| >60 | 2 | 294 | 0.7% (2/296) | |
| Smoke | ||||
| Yes | 0 | 27 | 0 (0/27) | 1.000 |
| No | 6 | 762 | 0.8% (6/768) | |
| Histologic type | ||||
| AIS | 1 | 95 | 1.0% (1/96) | 0.279 |
| MIA | 1 | 520 | 0 (0/521) | |
| INMA | 3 | 158 | 2.5% (4/161) | |
| IMA | 1 | 16 | 5.9% (1/17) |
表7
6例ROS1基因重排阳性病例临床病理特征总结
| Case | Sex | Age/year | Maximum diameter | Pathological diagnosis and morphological characteristics |
|---|---|---|---|---|
| 1 | F | 55 | 0.5cm | AIS |
| 2 | F | 55 | 0.5cm | IMA with micropapillary and ethmoid structures |
| 3 | F | 67 | 0.6cm | INMA (Acinar predominant adenocarcinoma, Acinar type accounted for 80%, papillary type 10% and micropapillary type 10%) |
| 4 | M | 58 | 1cm | INMA (Acinar primary adenocarcinoma, visible papillary structure ) |
| 5 | F | 59 | 1cm | INMA, (Acinar primary adenocarcinoma, micropapillary, air cavity spread) |
| 6 | F | 62 | 1cm | INMA (acinar type 50%, micropapillary type 50%, visible air cavity spread) |
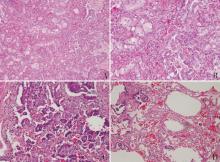
图5
ROS1基因重排阳性病例病理形态学特征 A:黏液腺癌,低倍镜下腺腔内见黏液,可见筛状及微乳头结构(HE ×100);B:中倍镜放大显示筛状及微乳头结构,肿瘤细胞核圆形或卵圆形,可见核仁(HE ×200);C另一病例显示微乳头样结构为主(HE ×200);D:气腔播散(HE ×100)
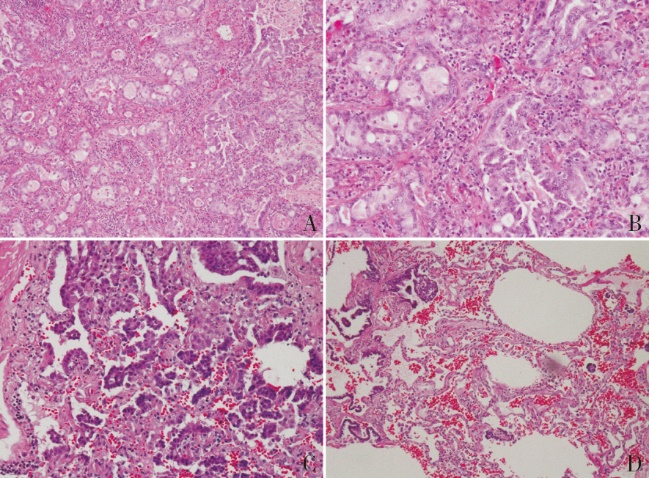
表8
同一患者2次手术切除标本分子检测结果不同的病例的临床病理特征
| Case | Sex | Age | Smoke | The first molecular detection | Histologic type/maximum diameter | The second molecular detection | Histologic type/maximum diameter |
|---|---|---|---|---|---|---|---|
| ① | M | 43 | No | EGFR 19Del | INMA/1.2 cm | EGFR- | MIA/0.6 cm |
| ALK- | ALK- | ||||||
| ROS1- | ROS1- | ||||||
| ② | F | 49 | No | EGFR 19Del | MIA/0.6 cm | EGFR- | MIA/0.5 cm |
| ALK- | |||||||
| ROS1- | |||||||
| ③ | M | 76 | No | EGFR- | INMA/3 cm | 21L858R | INMA/0.8 cm |
| ALK- | ALK- |
| [1] | SUNG H, FERLAY J, SIEGEL R L, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2021, 71(3):209-249. |
| [2] | CAO W, CHEN H D, YU Y W, et al. Changing profiles of cancer burden worldwide and in China: a secondary analysis of the global cancer statistics 2020[J]. Chin Med J (Engl), 2021, 134(7):783-791. |
| [3] |
王泽洲, 郑莹. 1990年至2020年间全球及我国肺癌的发病流行趋势及防控措施[J]. 诊断学理论与实践, 2023, 22(01): 1-7.
doi: 10.16150/j.1671-2870.2023.01.001 |
| WANG Z Z, ZHENG Y. Lung cancer worldwide and in China from 1990 to 2020: prevalence and prevention measures[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(01):1-7. | |
| [4] | ZHUANG X, ZHAO C, LI J, et al. Clinical features and therapeutic options in non-small cell lung cancer patients with concomitant mutations of EGFR, ALK, ROS1, KRAS or BRAF[J]. Cancer Med, 2019, 8(6):2858-2866. |
| [5] |
DU X, SHAO Y, QIN H F, et al. ALK-rearrangement in non-small-cell lung cancer (NSCLC)[J]. Thorac Cancer, 2018, 9(4):423-430.
doi: 10.1111/1759-7714.12613 pmid: 29488330 |
| [6] |
LIN J J, SHAW A T. Recent Advances in Targeting ROS1 in Lung Cancer[J]. J Thorac Oncol, 2017, 12(11):1611-1625.
doi: S1556-0864(17)30668-8 pmid: 28818606 |
| [7] | CHAPMAN A M, SUN K Y, RUESTOW P, et al. Lung cancer mutation profile of EGFR, ALK, and KRAS: Meta-analysis and comparison of never and ever smokers[J]. Lung Cancer, 2016,102:122-134. |
| [8] |
ARTEAGA C L, ENGELMAN J A. ERBB receptors: from oncogene discovery to basic science to mechanism-based cancer therapeutics[J]. Cancer Cell, 2014, 25(3):282-303.
doi: 10.1016/j.ccr.2014.02.025 pmid: 24651011 |
| [9] |
DEARDEN S, STEVENS J, WU Y L, et al. Mutation incidence and coincidence in non small-cell lung cancer: meta-analyses by ethnicity and histology (mutMap)[J]. Ann Oncol, 2013, 24(9):2371-2376.
doi: 10.1093/annonc/mdt205 pmid: 23723294 |
| [10] | SHI Y, LI J, ZHANG S, et al. Molecular epidemiology of EGFR mutations in Asian patients with advanced non-small-cell lung cancer of adenocarcinoma histology - mainland China subset analysis of the PIONEER study[J]. PLoS One, 2015, 10(11):e0143515. |
| [11] |
TSAO A S, SCAGLIOTTI G V, BUNN P A, et al. Scientific advances in lung cancer 2015[J]. Journal of Thoracic Oncology, 2016, 11(5):613-638.
doi: S1556-0864(16)30022-3 pmid: 27013409 |
| [12] | 贺佳子, 黄清洁, 李莉, 等. 396例非小细胞肺癌EGFR,KRAS,ALK和BRAF基因突变状态及其临床病理特征[J]. 临床与病理杂志, 2020, 40(09):2252-2258. |
| HE J Z, HUANG Q J, LI L, et al. Mutation status of EGFR, KRAS, ALK and BRAF genes and their clinicopathological characteristics in 396 patients with non-small cell lung cancer[J]. J Clin Pathol Res, 2020, 40(09):2252-2258. | |
| [13] | 眭玉霞, 邓晓宇, 伍铮, 等. 非小细胞肺癌驱动基因突变与临床病理特征的关系[J]. 临床与实验病理学杂志, 2020, 36(09):1023-1028. |
| SUI Y X, DENG X Y, WU Z, et al. Comprehensive investigation of driver gene expression and clinicopathological characteristics in non-small cell lung cancer[J]. J Clin Pathol Res, 2020, 36(09):1023-1028. | |
| [14] | STEWART E L, TAN S Z, LIU G, et al. Known and putative mechanisms of resistance to EGFR targeted therapies in NSCLC patients with EGFR mutations-a review[J]. Transl Lung Cancer Res, 2015, 4(1):67-81. |
| [15] |
KOBAYASHI S, CANEPA H M, BAILEY A S, et al. Compound EGFR mutations and response to EGFR tyrosine kinase inhibitors[J]. J Thorac Oncol, 2013, 8(1):45-51.
doi: 10.1097/JTO.0b013e3182781e35 pmid: 23242437 |
| [16] |
DUYSTER J, BAI R Y, MORRIS S W. Translocations involving anaplastic lymphoma kinase (ALK)[J]. Oncogene, 2001, 20(40):5623-5637.
pmid: 11607814 |
| [17] |
MOTEGI A, FUJIMOTO J, KOTANI M, et al. ALK receptor tyrosine kinase promotes cell growth and neurite outgrowth[J]. J Cell Sci, 2004, 117(Pt 15):3319-3329.
pmid: 15226403 |
| [18] |
IWAHARA T, FUJIMOTO J, WEN D, et al. Molecular characterization of ALK, a receptor tyrosine kinase expressed specifically in the nervous system[J]. Oncogene, 1997, 14(4):439-449.
doi: 10.1038/sj.onc.1200849 pmid: 9053841 |
| [19] | DEVARAKONDA S, MORGENSZTERN D, GOVINDAN R. Genomic alterations in lung adenocarcinoma[J]. Lancet Oncol, 2015, 16(7):e342-351. |
| [20] |
SHAW A T, ENGELMAN J A. ALK in lung cancer: past, present, and future[J]. J Clin Oncol, 2013, 31(8):1105-1111.
doi: 10.1200/JCO.2012.44.5353 pmid: 23401436 |
| [21] | ACQUAVIVA J, WONG R, CHAREST A. The multifa-ceted roles of the receptor tyrosine kinase ROS in development and cancer[J]. Biochim Biophys Acta, 2009, 1795(1):37-52. |
| [22] |
RIKOVA K, GUO A, ZENG Q, et al. Global survey of phosphotyrosine signaling identifies oncogenic kinases in lung cancer[J]. Cell, 2007, 131(6):1190-1203.
doi: 10.1016/j.cell.2007.11.025 pmid: 18083107 |
| [23] | STRANSKY N, CERAMI E, SCHALM S, et al. The landscape of kinase fusions in cancer[J]. Nat Commun, 2014,5:4846. |
| [24] | Cancer Genome Atlas Research N. Comprehensive molecular profiling of lung adenocarcinoma[J]. Nature, 2014, 511(7511):543-550. |
| [25] |
BERGETHON K, SHAW A T, OU S H, et al. ROS1 rearrangements define a unique molecular class of lung cancers[J]. J Clin Oncol, 2012, 30(8):863-870.
doi: 10.1200/JCO.2011.35.6345 pmid: 22215748 |
| [26] | TAKEUCHI K, SODA M, TOGASHI Y, et al. RET,ROS1 and ALK fusions in lung cancer[J]. Nat Med, 2012, 18(3):378-381. |
| [27] |
VANSTEENKISTE J, CRINO L, DOOMS C, et al. 2nd ESMO Consensus Conference on Lung Cancer: early-stage non-small-cell lung cancer consensus on diagnosis, treatment and follow-up[J]. Ann Oncol, 2014, 25(8):1462-1474.
doi: 10.1093/annonc/mdu089 pmid: 24562446 |
| [28] |
HIRSCH F R, SCAGLIOTTI G V, MULSHINE J L, et al. Lung cancer: current therapies and new targeted treatments[J]. Lancet, 2017, 389(10066):299-311.
doi: S0140-6736(16)30958-8 pmid: 27574741 |
| [1] | 肖辅国, 潘自来. 浸润前病变的CT值变化在鉴别肺纯磨玻璃结节性质的价值探讨[J]. 诊断学理论与实践, 2019, 18(05): 521-525. |
| [2] | 曹琪琪, 杨文洁, 严福华, 刘燕. 血管集束征在肺磨玻璃结节定性诊断中的价值研究[J]. 诊断学理论与实践, 2018, 17(05): 521-525. |
| [3] | 杜海磊, 车嘉铭, 朱良纲, 李鹤成, 杭钧彪. 病理T1期浸润性肺腺癌不同病理亚型的临床特征及其预后分析[J]. 诊断学理论与实践, 2018, 17(01): 82-86. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||