诊断学理论与实践 ›› 2024, Vol. 23 ›› Issue (01): 83-89.doi: 10.16150/j.1671-2870.2024.01.011
李明1, 陈克敏2( ), 潘自来2, 罗禹1
), 潘自来2, 罗禹1
收稿日期:2023-01-29
出版日期:2024-02-25
发布日期:2024-05-30
通讯作者:
陈克敏 E-mail:keminchenrj@163.com基金资助:
LI Ming1, CHEN Kemin2(), PAN Zilai2, LUO Yu1
Received:2023-01-29
Published:2024-02-25
Online:2024-05-30
摘要:
脑梗死是全球排名第二大致死原因,在中国已成为第一大致残及死亡原因。急性缺血性脑梗死(acute ischemic stroke,AIS)则是最常见的脑梗死类型,约占全部脑梗死的80%。出血性转化(hemorrhagic transformation,HT)是AIS患者的自然转归过程之一,也是静脉溶栓治疗(intravenous thrombolysis,IVT)或血管内取栓治疗等治疗后最严重的并发症,给患者及其家庭和社会都带来沉重的负担。精准预测、评估AIS的HT具有重要临床意义。近年影像学研究集中于CT和MRI评估HT的价值。CT平扫诊断HT价值有限,AIS治疗前,阿尔伯塔脑梗死计划早期诊断评分≤7分与HT发生相关(P=0.033),高密度大脑中动脉征是发生HT的独立危险因素(OR=10.334);AIS取栓治疗后24 h复查双能CT,预测2~7 d内发生HT风险的效能较高(灵敏度82.5%、特异度100%)。CT血管造影中,血栓负荷高的患者HT发生概率上升(OR=1.28);侧支循环良好的AIS患者HT发生率低。CT灌注成像参数包括表面渗透性、脑血容量、Tmax等,均有较好的HT预测价值。MRI平扫中,FLAIR上高信号可预测HT的发生;MRI弥散加权成像,高信号区域体积可预测HT(ROC曲线下面积0.78);MRI磁敏感率加权成像,刷状征、微出血灶提示HT的发生;MRI增强T1加权成像,脑实质强化与HT发生显著相关(P<0.05);MRI灌注加权成像中,梗死区脑血容量降低可预测HT。此外,CT及MRI图像后处理系统RAPID提升了评估HT的效能。建议根据各急救中心的硬件及当地医疗情况,设置个性化的影像学检测方式及流程,预测及管理HT。
中图分类号:
李明, 陈克敏, 潘自来, 罗禹. CT及MRI预测急性缺血性脑梗死出血性转化的价值研究进展[J]. 诊断学理论与实践, 2024, 23(01): 83-89.
LI Ming, CHEN Kemin, PAN Zilai, LUO Yu. Research progress on the value of CT and MRI in predicting hemorrhagic transformation after acute ischemic stroke[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(01): 83-89.
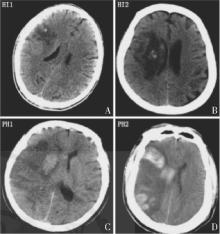
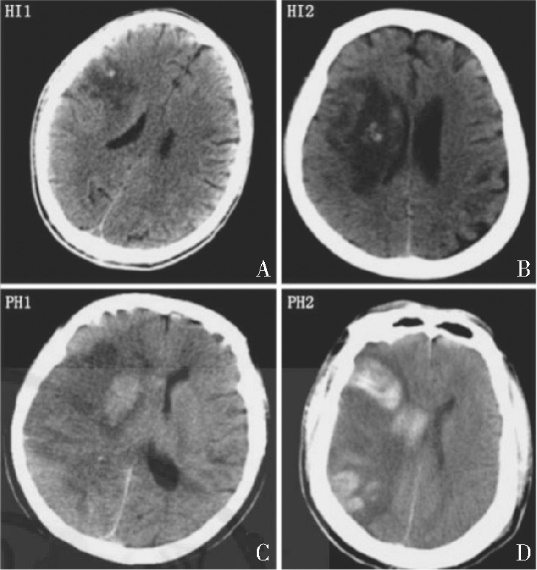
图1
HT的欧洲急性脑卒中协作研究分型 A:HI-1型,梗死灶边缘仅有小斑片状出血;B:HI-2型,梗死灶内有较多融合性斑片状出血,但无占位效应;C:PH-1型,梗死灶内出现血肿,范围≤30%,伴有较轻的占位效应;D:PH-2型,密度较高的血肿,范围>30%,且占位效应明显。
| [1] | GBD 2019 Stroke Collaborators. Global, regional, and national burden of stroke and its risk factors, 1990-2019: a systematic analysis for the global burden of disease study[J]. Lancet Neurol, 2021, 20(10):795-820. |
| [2] |
OTT B R, ZMMANI A, KLEEFIELD J, et al. The clinical spectrum of hemorrhagic infarction[J]. Stroke, 1986, 17(4):630-637.
pmid: 3738944 |
| [3] | 《中国脑卒中防治报告2019》编写组. 《中国脑卒中防治报告2019》概要[J]. 中国脑血管病杂志, 2020, 17(5):272-281. |
| Report on Stroke Prevention And Treatment in China Writing Group. Brief report on stroke prevention and treatment in China,2019[J]. Chin J Cerebrovasc Dis, 2020, 17(5): 272-281. | |
| [4] | 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性脑梗死后出血转化诊治共识2019[J]. 中华神经科杂志, 2019, 52(4):252-265. |
| Chinese Society of Neurology, Chinese Stroke Society. Consensus on diagnosis and treatment of hemorrhagic transformation after acute ischemic stroke in China 2019[J]. Chin J Neurol, 2019, 52(4):252-265. | |
| [5] |
MEHTA R H, COX M, SMITH E E, et al. Race/ethnic differences in the risk of hemorrhagic complications among patients with ischemic stroke receiving thrombolytic therapy[J]. Stroke, 2014, 45(8):2263-2269.
doi: 10.1161/STROKEAHA.114.005019 pmid: 25070958 |
| [6] | VINAY K, ABUL K A, JON C A, et al. Robbins and Cotran pathologic basis of disease[M]. 9 Ed. Amsterdam: Elsevier, 2015:129-131,1266-1267. |
| [7] |
FRIZZELL J P. Acute stroke: pathophysiology, diagnosis, and Treatment[J]. AACN Clin Issues, 2005, 16(4): 421-440.
doi: 10.1097/00044067-200510000-00002 pmid: 16269890 |
| [8] | HACKE W, KASTE M, FIESCHI C, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II)[J]. Lancet, 1998, 352(9136):1245-1251. |
| [9] | LARRUE V, VON KUMMMER R R, MÜLLER A, et al. Risk for severe hemorrhagic transformation in ischemic stroke patients treated with recombinant tissue plasminogen activator:a secondary analysis of the European-Australasian Acute Stroke Study (ECASS II)[J]. Stroke, 2011, 32(2):438-441. |
| [10] | EMBERSON J, LEES K R, LYDEN P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischae-mic stroke: a meta-analysis of individual patient data from randomised trials[J]. Lancet, 2014, 384(9958):1929-1935. |
| [11] | WHITELEY W N, SLOT K B, FERNANDES P, et al. Risk factors for intracranial hemorrhage in acute ischemic stroke patients treated with recombinant tissue plasminogen activator a systematic review and meta-analysis of 55 studies[J]. Stroke, 2012, 43(11):2904-2909. |
| [12] |
CASTELLANOS M, LEIRA R, SERENA J, et al. Plasma metalloproteinase-9 concentration predicts hemorrhagic transformation in acute ischemic stroke[J]. Stroke, 2003, 34(1):40-46.
pmid: 12511748 |
| [13] |
PRAKKAMAKUL S, YOO A J. ASPECTS CT in acute ischemia: review of current data[J]. Top Magn Reson Imaging, 2017, 26(3):103-112.
doi: 10.1097/RMR.0000000000000122 pmid: 28277460 |
| [14] | DZIALOWSKI I, HILL M D, COUTTS S B, et al. Extent of early ischemic changes on computed tomography (CT) before thrombolysis: prognostic value of the Alberta Stroke Program Early CT Score in ECASS Ⅱ[J]. Stroke, 2006, 37(4):973-978. |
| [15] |
GÁCS G, FOX A J, BARNETT H J, et al. CT visualization of intracranial arterial thromboembolism[J]. Stroke, 1983, 14(5):756-762.
pmid: 6658961 |
| [16] | 黄文磊, 吴雯菁, 姜亦伦. 多模态CT大脑中动脉高密度征对急性缺血性脑卒中出血转化的预测价值的探讨[J]. 医学影像学杂志, 2022, 32(6):919-923. |
| HUANG W L, WU W J, JIANG Y L. Study on the predictive value of high density sign of middle cerebral artery in acute ischemic stroke under multi-modeCT[J]. Med Imaging, 2022, 32(6):919-923. | |
| [17] |
YAGHI S, BOEHME A K, DIBU J, et al. Treatment and outcome of thrombolysis-related hemorrhage: a multicenter retrospective study[J]. JAMA Neurol, 2015, 72(12): 1451-1457.
doi: 10.1001/jamaneurol.2015.2371 pmid: 26501741 |
| [18] | The NINDS t-PA Stroke Study Group. Intracerebral hemorrhage after intravenous t-PA therapy for ischemic stroke[J]. Stroke, 1997, 28(11):2109-2118. |
| [19] |
TIJSSEN M P, HOFMAN P A, STADLER A A, et al. The role of dual energy CT in differentiating between brain haemorrhage and contrast medium after mechanical revascularisation in acute ischaemic stroke[J]. Eur Radiol, 2014, 24(4):834-840.
doi: 10.1007/s00330-013-3073-x pmid: 24258277 |
| [20] | 丁伟莉, 王天宇, 陈青, 等. 急性缺血性卒中血管内介入治疗术后即刻及24h双能CT检查对脑出血转化评估的作用[J]. 中国脑血管病杂志, 2023, 20(4):834-840. |
| DING W L, WANG T Y, CHEN Q, et al. Role of dual-energy CT in different time intervals for the evaluation of postoperative hemorrhagic transformation in endovascular intervention for acute ischemic stroke[J]. Chin J Cerebrovasc Dis, 2023, 20(4):834-840. | |
| [21] |
HORSCH A D, BENNINK E, VAN S T, et al. Computed tomography perfusion derived blood-brain barrier permeability does not yet improve prediction of hemorrhagic transformation[J]. Cerebrovasc Dis, 2018, 45(1-2):26-32.
doi: 10.1159/000485043 pmid: 29402765 |
| [22] |
BANG O Y, GOYAL M, LIEBESKIND D S. Collateral circulation in ischemic stroke: assessment tools and therapeutic strategies[J]. Stroke, 2015, 46(11):3302-3309.
doi: 10.1161/STROKEAHA.115.010508 pmid: 26451027 |
| [23] |
MADELUNG C F, OVESEN C, TRAMPEDACH C, et al. Leptomeningeal collateral status predicts outcome after middle cerebral artery occlusion[J]. Acta Neurol Scand, 2018, 137(1):125-132.
doi: 10.1111/ane.12834 pmid: 28905995 |
| [24] |
LI Q, GAO X, YAO Z, et al. Permeability surface of deep middle cerebral artery territory on computed tomographic perfusion predicts hemorrhagic transformation after stroke[J]. Stroke, 2017, 48(9):2412-2418.
doi: 10.1161/STROKEAHA.117.017486 pmid: 28775139 |
| [25] | BENNINK E, HORSCH A D, DANKBAAR J W, et al. CT perfusion analysis by nonlinear regression for predic-ting hemorrhagic transformation in ischemic stroke[J]. Med Phys, 2015, 42(8):4610-4618. |
| [26] | JAIN A R, JAIN M, KANTHALA A R, et al. Association of CT perfusion parameters with hemorrhagic transformation in acute ischemic stroke[J]. AJNR Am J Neuroradiol, 2013, 34(10):1895-1900. |
| [27] |
BATCHELOR C, PORDELI P, D'ESTERRE C D, et al. Use of noncontrast computed tomography and computed tomographic perfusion in predicting intracerebral hemorrhage after intravenous alteplase therapy[J]. Stroke, 2017, 48(6):1548-1553.
doi: 10.1161/STROKEAHA.117.016616 pmid: 28446625 |
| [28] |
YASSI N, PARSONS M W, CHRISTENSEN S, et al. Prediction of poststroke hemorrhagic transformation using computed tomography perfusion[J]. Stroke, 2013, 44(11):3039-3043.
doi: 10.1161/STROKEAHA.113.002396 pmid: 24003043 |
| [29] |
SOUZA L C, PAYABVASH S, WANG Y, et al. Admission CT perfusion is an independent predictor of hemorrhagic transformation in acute stroke with similar accuracy to DWI[J]. Cerebrovasc Dis, 2012, 33(1):8-15.
doi: 10.1159/000331914 pmid: 22143195 |
| [30] | THOMALLA G, CHENG B, EBINGER M, et al. DWI-FLAIR mismatch for the identification of patients with acute ischaemic stroke within 4.5 h of symptom onset (PRE-FLAIR): a multicentre observational study[J]. Lancet Neurol, 2011, 10(11):978-986. |
| [31] |
KUFNER A, GALINOVIC I, BRUNECKER P, et al. Early infarct flair hyperintensity is associated with increased hemorrhagic transformation after thrombolysis[J]. Eur J Neurol, 2013, 20(2):281-285.
doi: 10.1111/j.1468-1331.2012.03841.x pmid: 22900825 |
| [32] | JHA R, BATTEY T W, PHAM L, et al. Fluid-attenuated inversion recovery hyperintensity correlates with MMP -9 level and hemorrhagic transformation in acute ischemic stroke[J]. Stroke, 2014, 45(4):1040-1045. |
| [33] | LÖVBLAD K O, BAIRD A E, SCHLAUG G, et al. Isc-hemic lesion volumes in acute stroke by diffusion-weighted magnetic resonance imaging correlate with clinical outcome[J]. Ann Neurol, 1997, 42(2):164-170. |
| [34] |
SINGER O C, HUMPICH M C, FIEHLER J, et al. Risk for symptomatic intracerebral hemorrhage after thrombolysis assessed by diffusion-weighted magnetic resonance imaging[J]. Ann Neurol, 2008, 63(1):52-60.
pmid: 17880020 |
| [35] | EL NAWAR R, YEUNG J, LABREUCHE J, et al. MRI-based predictors of hemorrhagic transformation in patients with stroke treated by intravenous thrombolysis[J]. Front Neurol, 2019, 10(897):1-8. |
| [36] | OPPENHEIM C, SAMSON Y, DORMONT D, et al. DWI prediction of symptomatic hemorrhagic transformation in acute MCA infarct[J]. J Neuroradiol, 2002, 29(1):6-13. |
| [37] | SHINODA N, HORI S, MIKAMI K, et al. Prediction of hemorrhagic transformation after acute thrombolysis following major artery occlusion using relative ADC ratio: a retrospective study[J]. J Neuroradiol, 2017, 44(6):361-366. |
| [38] |
BEAUCHAMP M H, BEARE R, DITCHFIELD M, et al. Susceptibility weighted imaging and its relationship to outcome after pediatric traumatic brain injury[J]. Cortex, 2013, 49(2):591-598.
doi: 10.1016/j.cortex.2012.08.015 pmid: 23062584 |
| [39] | TERASAWA Y, YAMAMOTO N, MORIGAKI R, et al. Brush sign on 3T T2-weighted MRI as a potential predictor of hemorrhagic transformation after tissue plasminogen activator therapy[J]. Stroke, 2014, 45(1):274-276. |
| [40] |
NAGARAJA N, TASNEEM N, SHABAN A, et al. Cerebral microbleeds are an independent predictor of hemorrhagic transformation following intravenous alteplase administration in acute ischemic stroke[J]. J Stroke Cerebrovasc Dis, 2018, 27(5):1403-1411.
doi: S1052-3057(17)30718-8 pmid: 29398533 |
| [41] |
ZAND R, TSIVGOULIS G, SINGH M, et al. Cerebral microbleeds and risk of intracerebral hemorrhage post intravenous thrombolysis[J]. J Stroke Cerebrovasc Dis, 2017, 26(3):538-544.
doi: S1052-3057(16)30592-4 pmid: 28065404 |
| [42] |
HJORT N, WU O, ASHKANIAN M, et al. MRI detection of early blood-brain barrier disruption: parenchymal enhancement predicts focal hemorrhagic transformation after thrombolysis[J]. Stroke, 2008, 39(3):1025-1028.
doi: 10.1161/STROKEAHA.107.497719 pmid: 18258832 |
| [43] | LIU H S, CHUNG H W, CHOU M C, et al. Effects of microvascular permeability changes on contrast-enhanced T1 and pharmacokinetic MR imagings after ischemia[J]. Stroke, 2013, 44(7):1872-1877. |
| [44] |
CAMPBELL B C, CHRISTENSEN S, PARSONS M W, et al. Advanced imaging improves prediction of hemorrhage after stroke thrombolysis[J]. Ann Neurol, 2013, 73(4):510-519.
doi: 10.1002/ana.23837 pmid: 23444008 |
| [45] |
MISHRA N K, CHRISTENSEN S, WOUTERS A, et al. Reperfusion of very low cerebral blood volume lesion predicts parenchymal hematoma after endovascular therapy[J]. Stroke, 2015, 46(5):1245-1249.
doi: 10.1161/STROKEAHA.114.008171 pmid: 25828235 |
| [46] |
KIM J H, BANG O Y, LIEBESKIND D S, et al. Impact of baseline tissue status (diffusion-weighted imaging lesion) versus perfusion status (severity of hypoperfusion) on hemorrhagic transformation[J]. Stroke, 2010, 41(3):135-142.
doi: 10.1161/STROKEAHA.109.563122 pmid: 20075362 |
| [47] | LI M, LV Y, WANG M, et al. Magnetic resonance perfusion-weighted imaging in predicting hemorrhagic transformation of acute ischemic stroke:a retrospective study[J]. Diagnostics, 2023, 13(22):3404. |
| [48] | VYAS D, BOHRA V, KARAN V, et al. Rapid processing of perfusion and diffusion for ischemic strokes in the extended time window: an indian experience[J]. Ann Indian Acad Neurol, 2019, 22(1):96-99. |
| [49] | CAMPBELL B C V, MAJOIE C B L M, ALBERS G W, et al. Penumbral imaging and functional outcome in patients with anterior circulation ischaemic stroke treated with endovascular thrombectomy versus medical therapy: a meta-analysis of individual patient-level data[J]. Lancet Neurol, 2019, 18(3):e2. |
| [50] | 曹阳, 刘厚军, 程鸣, 等. MR常规序列及弥散加权成像对脑梗死不同发病时期的诊断价值比较[J]. 安徽医学, 2023, 44(6):702-704. |
| CAO Y, LIU HJ, CHENG M, et al. Comparison of diagnostic value of MR conventional sequence and diffusion-weighted imaging in different stages of cerebral infarction[J]. Anhui Med, 2023, 44(6):702-704. | |
| [51] | YAO L, ZHU H, LIW W, et al. Predictive effect of cortical ribbon sign in DWI on prognosis of mechanical thrombectomy in patients with acute ischemic stroke[J]. Chin J Clin Res, 2023, 36(3):343-346. |
| [52] | 庞伟平, 王保爱. 进展性缺血性脑卒中临床诊疗研究进展[J]. 中国临床研究, 2023, 36(3):380-385. |
| PANG WP, WANG BA. Clinical diagnosis and treatment of progressive stroke[J]. Chin J Clin Res, 2023, 36(3):380-385. |
| [1] | 周敏慧, 谢心怡, 任汝静, 王刚. 以肢体无力为主要表现的原发性家族性脑钙化症一例报告[J]. 诊断学理论与实践, 2020, 19(1): 92-94. |
| [2] | 赵宗波, 贾传海, 刘晖. 动脉自旋标记磁共振灌注技术结合磁共振血管成像预测后循环脑梗死患者病情进展中的应用[J]. 诊断学理论与实践, 2019, 18(04): 412-417. |
| [3] | 李云峰, 江泓, 李宁, 孙青芳. 核磁共振成像诊断三叉神经痛的价值分析与研究[J]. 诊断学理论与实践, 2018, 17(05): 562-565. |
| [4] | 邢英琦, 陈丽敏, 陈虹秀. 经颅多普勒在脑梗死中的应用及展望[J]. 诊断学理论与实践, 2018, 17(04): 368-372. |
| [5] | 慕瑾瑾, 杨康, 冯玉兰, 傅毅. 高血压性脑出血患者伴新发无症状性脑梗死的相关危险因素分析及预后的探讨[J]. 诊断学理论与实践, 2016, 15(05): 492-497. |
| [6] | 买买提依明, 热西旦, 陈波, 张祥, 马卫英, 杨康, 傅毅. 染色体9p21多态性与急性非心源性脑梗死患者颈动脉斑块的易感性分析[J]. 诊断学理论与实践, 2016, 15(05): 498-502. |
| [7] | 金磊, 陈宁, 吴洁敏, 张蕾, 徐志毅, 倪培华,. 白细胞介素4基因多态性与脑梗死的关系[J]. 诊断学理论与实践, 2015, 14(06): 554-559. |
| [8] | 陈淳, 王家莉, 季承博, 布阿提卡木, 彭亦雩, 傅毅,. 抵抗素与脑梗死及其危险因素的相关性研究[J]. 诊断学理论与实践, 2015, 14(03): 279-282. |
| [9] | 潘慧瑾, 曾丽莉, 辛晓瑜, 郭正良, 刘建荣,. 急性脑卒中患者血清氨基末端B型利钠肽前体水平的变化及其临床意义[J]. 诊断学理论与实践, 2014, 13(05): 519-523. |
| [10] | 梁璆荔, 傅毅, 倪培华,. 载脂蛋白H基因启动子32位点多态性与脑梗死的相关性研究[J]. 诊断学理论与实践, 2013, 12(05): 559-563. |
| [11] | 朱扬, 吴洁敏, 孙家兰, 蔡健, 颜静, 金小燕, 卢钟娇, 倪培华, 傅毅,. 对氧磷酶基因多态性与脑梗死关联性的探讨[J]. 诊断学理论与实践, 2013, 12(01): 90-94. |
| [12] | 杨振华, 倪培华, 傅毅, 吴洁敏, 应雅韵, 王文惠, 堵一乔,. 脑梗死与对氧磷酶1基因-162A/G多态性的关系[J]. 诊断学理论与实践, 2011, 10(03): 247-250. |
| [13] | 金磊, 高月求, 葛海良,. 白细胞介素基因多态性与脑梗死的关系[J]. 诊断学理论与实践, 2011, 10(02): 179-181. |
| [14] | 杨振华, 王文惠, 应雅韵, 堵一乔, 倪培华,. 脑梗死与对氧磷酶1基因192G/A位点多态性的关系[J]. 诊断学理论与实践, 2011, 10(01): 50-54. |
| [15] | 倪培华, 傅毅, 陈宁, 应雅韵,. 血管内皮生长因子基因多态性与脑梗死的关系[J]. 诊断学理论与实践, 2010, 9(06): 560-565. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||