诊断学理论与实践 ›› 2021, Vol. 20 ›› Issue (02): 184-189.doi: 10.16150/j.1671-2870.2021.02.012
戎天艺, 花芸, 陈德艳, 何旻( )
)
收稿日期:2020-12-31
出版日期:2021-04-25
发布日期:2022-06-28
通讯作者:
何旻
E-mail:2294398572@99.com
RONG Tianyi, HUA Yun, CHEN Deyan, HE Min()
Received:2020-12-31
Online:2021-04-25
Published:2022-06-28
Contact:
HE Min
E-mail:2294398572@99.com
摘要:
目的:探讨血清天冬酰胺内肽酶(legumain,LGMN)与急性大动脉粥样硬化(large-artery atherosclerosis, LAA)型卒中患者早期神经功能恶化(early neurological deterioration, END)间的相关性。方法:前瞻性纳入334例急性LAA型卒中患者,检测其血清LGMN水平。END定义为入院3 d内任意时间点复评美国国立卫生研究院卒中量表(National Institute of Health Stroke Scale,NIHSS)评分较入院时增加≥2分。将患者按照入院后有无发生END进行分组比较,建立Logistic回归模型分析确定END发生的独立危险因素。采用受试者操作特征(receiver operator characteristic,ROC)曲线分析血清LGMN预测患者发生END的价值。结果:334例LAA型卒中患者中有78例(23.4%)发生END,作为END组,余256例为非END组。单因素结果分析显示,END组的LGMN水平、年龄、合并疾病(高血压、糖尿病、高血脂)比例、存在易损斑块的比例、入院收缩压水平、入院NIHSS评分和空腹血糖、糖化血红蛋白、超敏C反应蛋白水平均高于非END组,差异均有统计学意义(P均<0.05)。END患者中,中度狭窄组(7.05 μg/L)及闭塞组(6.80 μg/L)的血清LGMN水平显著低于重度狭窄组(8.66 μg/L)(P<0.05)。多因素Logistic回归分析结果显示,血清LGMN水平升高是患者发生END的独立危险因素[优势比(odds ratio,OR)=1.309,95% 置信区间(confidence interval,CI)为1.188~1.441,P<0.001)],其他危险因素还包括存在易损斑块、入院收缩压高、糖化血红蛋白水平高以及入院NIHSS评分高。ROC曲线分析结果显示,血清LGMN预测END的曲线下面积为0.715(95%CI为0.663~0.763,P<0.001),此时最佳临界值为6.73 μg/L。结论:LGMN水平升高是急性LAA型卒中患者发生END的独立危险因素,可能可作为预测END的新型生物标志物。
中图分类号:
戎天艺, 花芸, 陈德艳, 何旻. 血清天冬酰胺内肽酶与急性大动脉粥样硬化型卒中间相关性的前瞻性研究[J]. 诊断学理论与实践, 2021, 20(02): 184-189.
RONG Tianyi, HUA Yun, CHEN Deyan, HE Min. Prospective study on relationship between legumain and early neurological deterioration in patients with acute large artery atherosclerotic stroke[J]. Journal of Diagnostics Concepts & Practice, 2021, 20(02): 184-189.
图1
研究对象纳入和排除流程图
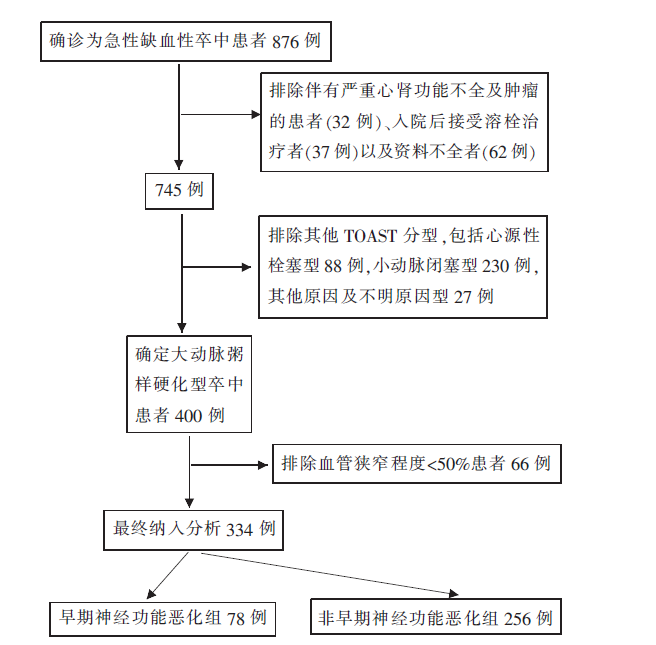
表1
END组与非END组资料比较
| 变量 | 非END组(n=256) | END组(n=78) | t值,或 χ2值,或Z值 | P值 |
|---|---|---|---|---|
| 年龄(岁)( | 71.2±10.8 | 72.8±9.7 | -1.221 | 0.224 |
| 男性[n(%)] | 159(62.1) | 45(57.7) | 0.491 | 0.484 |
| 体质量指数(kg/m2)( | 23.4±3.6 | 24.1±2.9 | -1.430 | 0.154 |
| 血管危险因素[n(%)] | ||||
| 高血压 | 183(71.5) | 67(85.9) | 6.597 | 0.010 |
| 糖尿病 | 109(42.6) | 46(59.0) | 6.462 | 0.011 |
| 心房颤动 | 36(14.1) | 9(11.5) | 0.327 | 0.568 |
| 高血脂 | 94(36.7) | 41(52.6) | 6.233 | 0.013 |
| 目前吸烟 | 87(34.0) | 26(33.3) | 0.011 | 0.915 |
| 目前喝酒 | 49(19.1) | 19(24.4) | 1.004 | 0.316 |
| 易损斑块 | 186(72.7) | 66(84.6) | 4.616 | 0.032 |
| 颅内血管狭窄程度[n(%)] | 5.755 | 0.056 | ||
| 中度 | 102(39.8) | 21(26.9) | ||
| 重度 | 84(33.0) | 26(33.3) | ||
| 闭塞 | 70(27.3) | 31(39.7) | ||
| 血压(mmHg)( | ||||
| 入院收缩压 | 138.4±16.7 | 144.9±20.9 | -2.800 | 0.005 |
| 入院舒张压 | 81.0±9.9 | 83.1±11.1 | -1.557 | 0.120 |
| LGMN(μg/L)[M(IQR)] | 5.11(4.45, 6.56) | 7.41(5.28,9.04) | -5.750 | <0.001 |
| 空腹血糖(mmol/L)[M(IQR)] | 5.49(4.87, 7.02) | 6.00(5.21,8.55) | -2.385 | 0.017 |
| 超敏C反应蛋白(mg/L)[M(IQR)] | 2.45(1.00,5.40) | 4.2(1.50,6.23) | -2.513 | 0.012 |
| 国际标准化比值( | 0.94±0.10 | 0.95±0.08 | 0.058 | 0.954 |
| D-二聚体(mg/L)( | 0.37(0.23,0.70) | 0.50(0.21,0.97) | -0.843 | 0.399 |
| 胆固醇(mmol/L)( | 4.61±1.13 | 4.76±1.16 | -1.050 | 0.295 |
| 甘油三酯(mmol/L)( | 1.57±1.60 | 1.57±0.95 | 0.002 | 0.999 |
| 高密度脂蛋白胆固醇(mmol/L)( | 1.16±0.26 | 1.20±0.29 | -1.128 | 0.260 |
| 低密度脂蛋白胆固醇(mmol/L)( | 2.78±0.85 | 2.62±1.14 | 1.127 | 0.262 |
| 糖化血红蛋白(%)( | 6.89±1.63 | 7.44±2.20 | -2.033 | 0.045 |
| 卒中部位[n(%)] | 1.762 | 0.184 | ||
| 前循环 | 156(60.9) | 54(69.2) | ||
| 后循环 | 100(39.1) | 24(30.8) | ||
| 入院NIHSS评分(分)[M(IQR)] | 4(2,6) | 5(3,8) | -4.084 | <0.001 |
| 他汀类药物[n(%)] | 52(20.3) | 16(20.5) | 0.001 | 0.969 |
表2
影响END发生因素的Logistic回归分析
| 变量 | 回归系数 | 标准误 | Wald | OR值(95%CI) | P值 |
|---|---|---|---|---|---|
| 易损斑块 | 0.892 | 0.380 | 5.500 | 2.441(1.158~5.144) | 0.019 |
| 入院收缩压 | 0.020 | 0.008 | 6.123 | 1.020(1.004~1.035) | 0.013 |
| LGMN | 0.269 | 0.049 | 29.934 | 1.309(1.188~1.441) | <0.001 |
| 糖化血红蛋白 | 0.179 | 0.074 | 5.808 | 1.196(1.034~1.384) | 0.016 |
| 入院NIHSS评分 | 0.064 | 0.025 | 6.243 | 1.066(1.014~1.120) | 0.012 |
图2
血清LGMN预测LAA型卒中患者发生END的ROC曲线
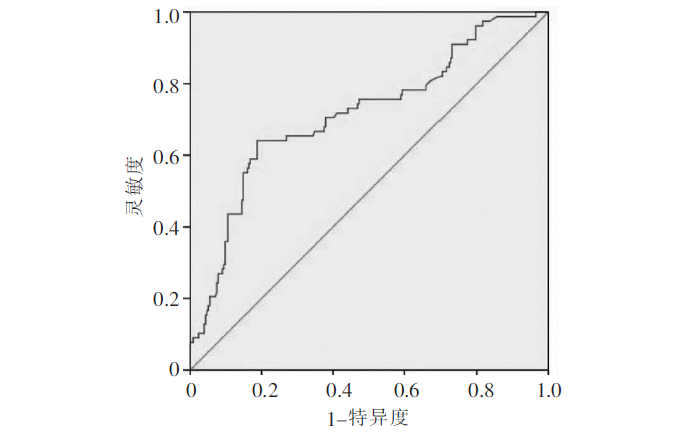
表3
END组颅内血管不同程度狭窄组的实验室指标比较
| 变量 | 中度狭窄组组(n=21) | 重度狭窄组(n=26) | 闭塞组(n=31) | P值 |
|---|---|---|---|---|
| LGMN(μg/L)[M(IQR)] | 7.05(4.71, 7.95)a) | 8.66(7.46,11.28) | 6.80(4.87,7.82)a) | 0.004 |
| 空腹血糖(mmol/L)[M(IQR)] | 5.97(4.81, 8.18) | 6.09(5.36,8.74) | 6.00(5.25,9.45) | 0.630 |
| 超敏C反应蛋白(mg/L)[M(IQR)] | 2.30(1.40, 4.70) | 4.00(1.73,6.53) | 4.30(1.80, 7.70) | 0.354 |
| 国际标准化比值( | 0.94±0.09 | 0.95±0.06 | 0.95±0.08 | 0.987 |
| D-二聚体(mg/L)( | 0.40(0.19, 0.99) | 0.47(0.20,0.60) | 0.53(0.21,1.69) | 0.441 |
| 胆固醇(mmol/L)( | 5.08±1.13 | 4.72±1.13 | 4.57±1.19 | 0.300 |
| 甘油三酯(mmol/L)( | 1.72±0.78 | 1.38±0.51 | 1.63±1.28 | 0.422 |
| 高密度脂蛋白胆固醇(mmol/L)( | 1.25±0.34 | 1.20±0.26 | 1.20±0.29 | 0.568 |
| 低密度脂蛋白胆固醇(mmol/L)( | 2.98±1.29 | 2.35±1.26 | 2.60±0.86 | 0.173 |
| 糖化血红蛋白(%)( | 6.90±1.66 | 7.45±1.81 | 7.79±2.75 | 0.367 |
| [1] |
Birschel P, Ellul J, Barer D. Progressing stroke: towards an internationally agreed definition[J]. Cerebrovasc Dis, 2004, 17(2-3):242-252.
pmid: 14718754 |
| [2] |
Weimar C, Mieck T, Buchthal J, et al. Neurologic wor-sening during the acute phase of ischemic stroke[J]. Arch Neurol, 2005, 62(3):393-397.
doi: 10.1001/archneur.62.3.393 URL |
| [3] |
Dávalos A, Toni D, Iweins F, et al. Neurological deterioration in acute ischemic stroke: potential predictors and associated factors in the European cooperative acute stroke study (ECASS) I[J]. Stroke, 1999, 30(12):2631-2636.
pmid: 10582989 |
| [4] | Yi X, Zhou Q, Sui G, et al. Matrix metalloproteinase-9 gene polymorphisms are associated with ischemic stroke severity and early neurologic deterioration in patients with atrial fibrillation[J]. Brain Behav, 2019, 9(6):e01291. |
| [5] |
Tisserand M, Seners P, Turc G, et al. Mechanisms of unexplained neurological deterioration after intravenous thrombolysis[J]. Stroke, 2014, 45(12):3527-3534.
doi: 10.1161/STROKEAHA.114.006745 pmid: 25336515 |
| [6] |
Battey TW, Karki M, Singhal AB, et al. Brain edema predicts outcome after nonlacunar ischemic stroke[J]. Stroke, 2014, 45(12):3643-3648.
doi: 10.1161/STROKEAHA.114.006884 URL |
| [7] |
Treadwell SD, Thanvi B. Malignant middle cerebral artery (MCA) infarction: pathophysiology, diagnosis and mana-gement[J]. Postgrad Med J, 2010, 86(1014):235-242.
doi: 10.1136/pgmj.2009.094292 pmid: 20354047 |
| [8] |
Siegler JE, Martin-Schild S. Early neurological deterioration(END) after stroke: the END depends on the definition[J]. Int J Stroke, 2011, 6(3):211-212.
doi: 10.1111/j.1747-4949.2011.00596.x pmid: 21557807 |
| [9] |
Alvarez V, Rossetti AO, Papavasileiou V, et al. Acute seizures in acute ischemic stroke: does thrombolysis have a role to play?[J]. J Neurol, 2013, 260(1):55-61.
doi: 10.1007/s00415-012-6583-6 URL |
| [10] |
Hart RG, Diener HC, Coutts SB, et al. Embolic strokes of undetermined source: the case for a new clinical construct[J]. Lancet Neurol, 2014, 13(4):429-438.
doi: 10.1016/S1474-4422(13)70310-7 URL |
| [11] |
Glass CK, Witztum JL. Atherosclerosis. the road ahead[J]. Cell, 2001, 104(4):503-516.
pmid: 11239408 |
| [12] |
Mattock KL, Gough PJ, Humphries J, et al. Legumain and cathepsin-L expression in human unstable carotid plaque[J]. Atherosclerosis, 2010, 208(1):83-89.
doi: 10.1016/j.atherosclerosis.2009.07.022 pmid: 19671471 |
| [13] |
Clerin V, Shih HH, Deng N, et al. Expression of the cysteine protease legumain in vascular lesions and functional implications in atherogenesis[J]. Atherosclerosis, 2008, 201(1):53-66.
doi: 10.1016/j.atherosclerosis.2008.01.016 URL |
| [14] |
Papaspyridonos M, Smith A, Burnand KG, et al. Novel candidate genes in unstable areas of human atherosclerotic plaques[J]. Arterioscler Thromb Vasc Biol, 2006, 26(8):1837-1844.
pmid: 16741146 |
| [15] | 中华医学会神经病学分会, 中华医学会神经病学分会脑血管病学组. 中国急性缺血性脑卒中诊治指南2018[J]. 中华神经科杂志, 2018, 51(9):666-682. |
| [16] |
Adams HP Jr, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10 172 in Acute Stroke Treatment[J]. Stroke, 1993, 24(1):35-41.
doi: 10.1161/01.str.24.1.35 pmid: 7678184 |
| [17] |
Sakurai K, Isahaya K, Takaishi S, et al. Effects of early statin treatment on inflammatory biomarkers and clinical deterioration in patients with acute ischemic stroke[J]. Rinsho Shinkeigaku, 2011, 51(1):6-13.
doi: 10.5692/clinicalneurol.51.6 URL |
| [18] |
Shirahama-Noda K, Yamamoto A, Sugihara K, et al. Biosynthetic processing of cathepsins and lysosomal degradation are abolished in asparaginyl endopeptidase-deficient mice[J]. J Biol Chem, 2003, 278(35):33194-33199.
doi: 10.1074/jbc.M302742200 pmid: 12775715 |
| [19] |
Morita Y, Araki H, Sugimoto T, et al. Legumain/asparaginyl endopeptidase controls extracellular matrix remodeling through the degradation of fibronectin in mouse renal proximal tubular cells[J]. FEBS Lett, 2007, 581(7):1417-1424.
doi: 10.1016/j.febslet.2007.02.064 URL |
| [20] |
Sun W, Lin Y, Chen L, et al. Legumain suppresses oxLDL-induced macrophage apoptosis through enhancement of the autophagy pathway[J]. Gene, 2018, 652:16-24.
doi: 10.1016/j.gene.2018.02.012 URL |
| [21] |
Umei TC, Kishimoto Y, Aoyama M, et al. High plasma levels of legumain in patients with complex coronary lesions[J]. J Atheroscler Thromb, 2020, 27(7):711-717.
doi: 10.5551/jat.52027 URL |
| [22] |
Lunde NN, Holm S, Dahl TB, et al. Increased levels of legumain in plasma and plaques from patients with carotid atherosclerosis[J]. Atherosclerosis, 2017, 257:216-223.
doi: 10.1016/j.atherosclerosis.2016.11.026 URL |
| [23] |
Wang ZH, Liu XL, Zhong M, et al. Pleiotropic effects of atorvastatin on monocytes in atherosclerotic patients[J]. J Clin Pharmacol, 2010, 50(3):311-319.
doi: 10.1177/0091270009340889 URL |
| [24] |
Dall E, Brandstetter H. Activation of legumain involves proteolytic and conformational events, resulting in a context- and substrate-dependent activity profile[J]. Acta Crystallogr Sect F Struct Biol Cryst Commun, 2012, 68(Pt1):24-31.
doi: 10.1107/S1744309111048020 URL |
| [1] | 宋洛卿, 戴廷军. 原发性抗磷脂综合征合并烟雾综合征一例并文献复习[J]. 诊断学理论与实践, 2022, 21(04): 497-503. |
| [2] | 梁亚丽, 赵海港, 项广宇. 应激性高血糖比值预测急性缺血性脑卒中患者溶栓治疗后1年不良预后的价值[J]. 诊断学理论与实践, 2021, 20(06): 562-566. |
| [3] | 刘安平, 凌枫, 史超, 孙璟. 上海社区老年脑卒中患者跌倒风险因素分析及风险识别模型的建立[J]. 诊断学理论与实践, 2021, 20(05): 475-479. |
| [4] | 王晨琛, 杨文波, 华玮, 陈晔芬, 苏秀秀, 龚俊世, 方跃华. 左心耳解剖形态、功能与非瓣膜性心房颤动患者脑卒中发生风险的相关性研究[J]. 诊断学理论与实践, 2020, 19(02): 151-156. |
| [5] | 计海峰, 杨雪莲, 姚峪岚, 蔡丽瑛, 来小音, 吴大玉, 徐瑜梅, 江梅. SOAR评分对急性缺血性卒中患者不良预后风险预测价值的探讨[J]. 诊断学理论与实践, 2018, 17(04): 423-427. |
| [6] | 胡荣郭, 庞德芳, 黄澍, 沈振坤, 陈玮, 杨育伟, 来小音, 朱玮, 吴菲菲, 计海峰, 吴大玉, 江梅, 孙家兰, 李龙宣. 急性缺血性卒中早期血浆miRNAs水平与房颤发生间的关系[J]. 诊断学理论与实践, 2017, 16(01): 98-103. |
| [7] | 徐亚伟, 唐恺,. 左心耳封堵预防房颤卒中的原理及临床价值[J]. 诊断学理论与实践, 2015, 14(03): 211-214. |
| [8] | 余跃天, 朱琤, 毛恩强, 舒良, 殷荣, 李昱洁, 刘春艳, 曹建国, 皋源,. 阿托伐他汀对缺血性脑卒中患者医院获得性肺炎的影响[J]. 诊断学理论与实践, 2015, 14(02): 169-174. |
| [9] | 潘慧瑾, 曾丽莉, 辛晓瑜, 郭正良, 刘建荣,. 急性脑卒中患者血清氨基末端B型利钠肽前体水平的变化及其临床意义[J]. 诊断学理论与实践, 2014, 13(05): 519-523. |
| [10] | 林继先, 赵静,. 生物标志物在缺血性脑卒中应用的研究进展[J]. 诊断学理论与实践, 2013, 12(03): 363-366. |
| [11] | 柳叶, 杨钊, 程琳, 刘建荣,. 主动脉弓上磁共振血管成像在缺血性脑卒中临床应用的意义[J]. 诊断学理论与实践, 2013, 12(03): 274-278. |
| [12] | 李京杭, 高平进,. 血浆同型半胱氨酸与高血压靶器官损害及并发症关系的分析[J]. 诊断学理论与实践, 2012, 11(06): 572-575. |
| [13] | 魏素平, 张春和,. 胶质纤维酸性蛋白与急性缺血性脑卒中的相关性研究[J]. 诊断学理论与实践, 2012, 11(03): 306-307. |
| [14] | 沈琳辉, 赵咏桔,. 脂联素的调控机制及其在缺血性脑卒中时的作用[J]. 诊断学理论与实践, 2011, 10(01): 86-90. |
| [15] | 王兆钺,. 血栓病的诊断指南解读[J]. 诊断学理论与实践, 2008, 7(05): 570-573. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||