诊断学理论与实践 ›› 2022, Vol. 21 ›› Issue (05): 598-605.doi: 10.16150/j.1671-2870.2022.05.009
何亲羽1,2, 王伟1, 陈立芬1, 张雪蕾1,2, 董治亚1( )
)
收稿日期:2022-03-15
出版日期:2022-10-25
发布日期:2023-01-29
通讯作者:
董治亚
E-mail:dzy831@126.com
HE Qinyu1,2, WANG Wei1, CHEN Lifen1, ZHANG Xuelei1,2, DONG Zhiya1()
Received:2022-03-15
Online:2022-10-25
Published:2023-01-29
Contact:
DONG Zhiya
E-mail:dzy831@126.com
摘要:
目的:报道2例家族性男性性早熟(familial male-limited precious puberty,FMPP)患者的临床特征、基因检测结果及治疗结果。方法:对2例FMPP患者进行详细的病史采集及体格检查,行促性腺激素释放激素(gonadotropin-releasing hormone, GnRH)激发试验、性激素、肾上腺皮质激素等检测以及相关影像学检查,同时采集相关家系成员的外周血进行基因检测,并在中文数据库及PubMed数据库中检索相关文献,进行综合探讨。结果:2例患者的初诊年龄分别为6岁1个月龄(病例1)和3岁7个月龄(病例2),均表现为阴茎、睾丸增大、生长加速、骨龄超前,病例2伴有攻击行为。实验室检查提示,2例患者的黄体生成素峰值分别为7.28 mIU/mL和4.96 mIU/mL,基础睾酮水平升高达2.49 ng/mL和3.58 ng/mL,而影像学检查未见异常。根据2例患者的病史及各项检查结果,临床诊断为中枢性性早熟。经基因检测显示,2例患儿的黄体生成素/人绒毛膜促性腺激素受体(luteinizing hormone/choriogonadotropin receptor,LHCGR)基因上均存在杂合变异[病例1存在c.1756TCTdel(p.Ser586del)变异来自其父亲;病例2存在c.1723A>C(p.Ile575Leu)变异,来自其母亲],根据美国医学遗传学与基因组学学会(The American College of Medical Genetics and Genomics, ACMG)指南评定为可能的致病性变异,故明确2例患儿均为继发于LHCGR基因突变的中枢性性早熟。检索数据库,分析35例FMPP资料完整的患者,中位发病时间在4岁,加入例1的变异,计18种基因变异被报道。结论:本文报道2例罕见FMPP病例,均为LHCGR基因突变导致,其中病例1的突变类型为国内外首次报道,病例2的突变类型已有报道。临床对于年龄小、起病或治疗效果欠佳的中枢性性早熟男童,需进一步明确有无LHCGR基因突变。
中图分类号:
何亲羽, 王伟, 陈立芬, 张雪蕾, 董治亚. LHCGR基因突变致家族性男性性早熟2例报告及文献复习[J]. 诊断学理论与实践, 2022, 21(05): 598-605.
HE Qinyu, WANG Wei, CHEN Lifen, ZHANG Xuelei, DONG Zhiya. Diagnosis and treatment of familial male precocious puberty caused by LHCGR gene mutation: two case reports and literature review[J]. Journal of Diagnostics Concepts & Practice, 2022, 21(05): 598-605.

图1
病例1骨龄约13岁 注:近端指骨骨骺稍增厚,桡侧向远侧有一小凸起;籽骨骨化中心出现。


图2
病例2骨龄约5岁 注:第1掌骨骨骺宽度大于其干骺端1/2,三角骨稍呈现月骨和钩骨的关节面。

表1
2例患者的实验室检查及影像学结果
| 指标 | 病例1 | 病例2 | 参考范围 |
|---|---|---|---|
| 黄体生成素峰值(mIU/mL) | 7.28 | 4.96 | - |
| 卵泡刺激素峰值(mIU/mL) | 6.96 | 9.07 | - |
| 睾酮(ng/mL) | 2.49 | 3.58 | 1.42~9.23 |
| 17羟孕酮(ng/mL) | 0.99 | 0.42 | 0.5~2.4 |
| 促肾上腺皮质激素(pg/mL) | 22.63 | 33.76 | 7.0~65.0 |
| 硫酸脱氢表雄酮(ug/dL) | 94.60 | 20.20 | - |
| β人绒毛膜促性激素(mIU/mL) | 0.30 | 0.27 | <5 |
| 骨龄 | 13岁 | 5岁 | - |
| 影像学检查 | (-) | (-) | - |
表2
文献复习资料
| 文献 | 氨基酸改变 | 病例数(n) | 遗传方式 | 起病年龄(岁) | 就诊年龄(岁) | BA-CA | 睾酮水平(ng/mL) |
|---|---|---|---|---|---|---|---|
| [ | S277I | 1 | D | 0.5 | 1.4 | 2.6 | 10.1 |
| [ | L368P | 2 | M M | 3.5 2.5 | 3.5 2.5 | 2.5 1.5 | 1.93 2.40 |
| [ [ | A373V A373V | 1 1 | M M | 1.5 5 | 1.5 8.0 | 2 5 | 4.79 2.5 |
| [ [ [ [ | M398T M398T M398T M398T | 1 1 2 2 | M P P P D D | 3 4.4 2 6 3 3 | 4.6 5.4 2.3 7.5 4.2 5.3 | 0.3 2.6 1 1 4.3 3.3 | 5.1 2.72 3.0 3.79 4.9 6.4 |
| [ [ | L457R L457R | 1 1 | D D | 2.5 2.8 | 2.5 2.8 | 3.5 3.2 | 3.92 6.2 |
| [ | I542L | 2 | M P | 3.1 4.1 | 3.1 4.1 | 0.9 4.9 | 0.74 4.8 |
| [ | D564G | 1 | M | 1.5 | 4.5 | 5.5 | 2.54 |
| [ [ | A568V A568V | 1 2 | P D P | 0.8 1.7 6.2 | 3.1 5.0 6.2 | 5.9 8 2.8 | 2.3 2.6 3.6 |
| [ | M571I | 2 | P P | 4.0 4.7 | - - | 2 2.3 | 0.91 1.05 |
| [ | A572V | 2 | D D | 5.5 4.5 | 5.5 6.8 | - 5.9 | 1.92 2.21 |
| [ 本文 | I575L I575L | 1 1 | M M | 0.5 0.2 | 2.5 3.5 | 1.5 1.5 | 3.09 3.58 |
| [ [ | T577I T577I | 1 2 | M M M | 4.0 2.8 2.5 | 7.5 3.0 2.8 | 5.5 1.6 0.1 | 6.5 5.1 1.4 |
| [ [ | D578H D578H | 1 1 | D D | 3 0.5 | 4.0 0.8 | 4 2.2 | 2.68 11.2 |
| [ | D578V | 2 | D D | 0.8 1.0 | 3.4 1.0 | 6.6 4.0 | 6.73 3.34 |
| [ | D578G | 1 | D | 2 | 2.1 | 0.9 | - |
| [ | D578Y | 1 | D | 0.9 | 1.3 | 3.7 | 8.9 |
| [ | D578A | 1 | D | 1 | 1.5 | 0.5 | 2.89 |
| [ | C581R | 1 | - | - | - | - | - |
| [ | C617Y | 1 | M | 6 | 6.5 | 2 | 2.79 |
| 本文 | S586X | 1 | P | 5.5 | 6.1 | 6.9 | 2.49 |
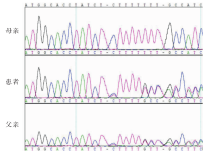
图3
病例1及父母基因测序结果 注:病例1及父亲存在相同的LHCGR基因碱基杂合缺失c.1756TCTdel(p.Ser586del)。
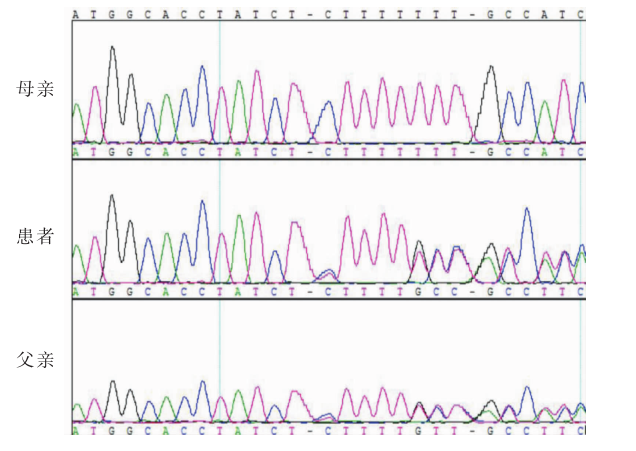

图4
病例2及父母基因测序结果 注:病例2及母亲存在相同的LHCGR基因杂合点突变:c.1723A>C(p.Ile575Leu)。
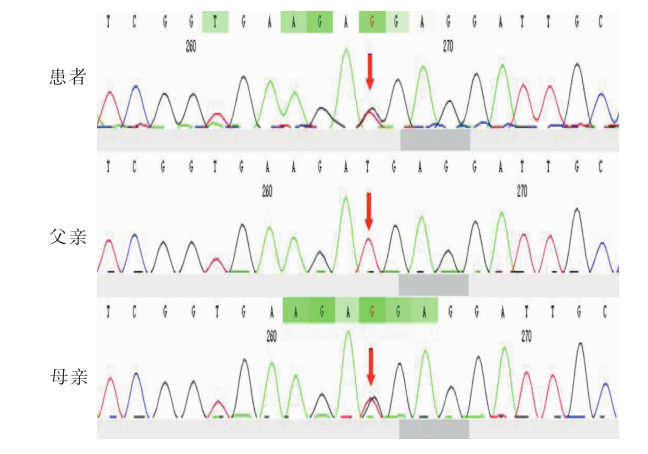

图5
LHCGR突变型蛋白三维结构模式图
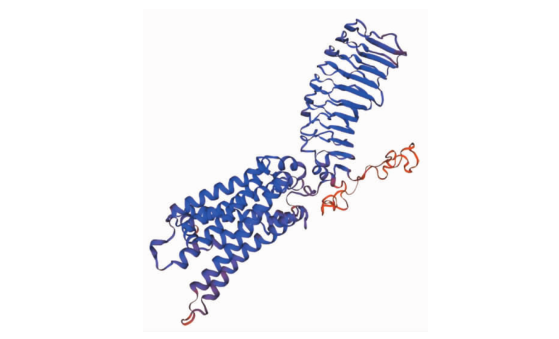
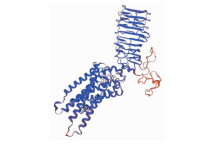
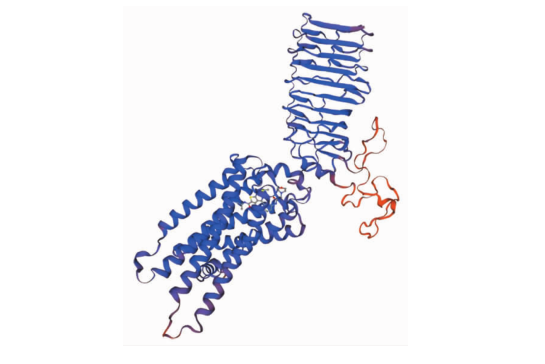
图6
LHCGR野生型蛋白三维模式图
| [1] |
Egli CA, Rosenthal SM, Grumbach MM, et al. Pituitary gonadotropin-independent male-limited autosomal dominant sexual precocity in nine generations: familial testotoxicosis[J]. J Pediatr, 1985, 106(1):33-40.
doi: 10.1016/S0022-3476(85)80460-1 URL |
| [2] |
Özcabı B, Tahmiscioğlu Bucak F, Ceylaner S, et al. Testotoxicosis: Report of Two Cases, One with a Novel Mutation in LHCGR Gene[J]. J Clin Res Pediatr Endocrinol, 2015, 7(3):242-248.
doi: 10.4274/jcrpe.2067 pmid: 26831561 |
| [3] |
Almeida MQ, Brito VN, Lins TS, et al. Long-term treatment of familial male-limited precocious puberty (testotoxicosis) with cyproterone acetate or ketoconazole[J]. Clin Endocrinol (Oxf), 2008, 69(1):93-98.
doi: 10.1111/j.1365-2265.2007.03160.x URL |
| [4] |
Gromoll J, Partsch CJ, Simoni M, et al. A mutation in the first transmembrane domain of the lutropin receptor causes male precocious puberty[J]. J Clin Endocrinol Metab, 1998, 83(2):476-80.
doi: 10.1210/jcem.83.2.4579 URL |
| [5] | 茅江峰, 伍学焱, 聂敏, 等. 生殖细胞系黄体生成素受体基因杂合突变(M398T)导致家族性男性性早熟[J]. 中华内科杂志, 2010, 49(12):1024-1027. |
| Mao JF, Wu XY, Nie M, et al. A report of familial male-limited precocious puberty caused by a germ-line heterozygous mutation (M398T) in luteinizing hormone receptor gene[J]. Chin J Inter Med, 2010, 49(12):1024-1027. | |
| [6] |
Ignacak M, Hilczer M, Zarzycki J, et al. Substitution of M398T in the second transmembrane helix of the LH receptor in a patient with familial male-limited precocious puberty[J]. Endocr J, 2000, 47(5):595-599.
pmid: 11200941 |
| [7] |
Shinagawa T, Katsumata N, Sato N, et al. Japanese familial patients with male-limited precocious puberty[J]. Endocr J, 2000, 47(6):777-782.
pmid: 11228053 |
| [8] |
Bertelloni S, Baroncelli GI, Lala R, et al. Long-term outcome of male-limited gonadotropin-independent precocious puberty[J]. Horm Res, 1997, 48(5):235-239.
pmid: 9362394 |
| [9] | Latronico AC, Abell AN, Arnhold IJ, et al. A unique constitutively activating mutation in third transmembrane helix of luteinizing hormone receptor causes sporadic male gonadotropin-independent precocious puberty[J]. J Clin Endocrinol Metab, 1998, 83(7):2435-2440. |
| [10] |
Lenz AM, Shulman D, Eugster EA, et al. Bicalutamide and third-generation aromatase inhibitors in testotoxicosis[J]. Pediatrics, 2010, 126(3):e728-e733.
doi: 10.1542/peds.2010-0596 URL |
| [11] |
Jeha GS, Lowenthal ED, Chan WY, et al. Variable presentation of precocious puberty associated with the D564G mutation of the LHCGR gene in children with testotoxicosis[J]. J Pediatr, 2006, 149(2):271-274.
doi: 10.1016/j.jpeds.2006.03.017 URL |
| [12] | 陈瑞敏, 张莹, 杨晓红, 等. 家族性男性性早熟一家系LHCGR基因突变分析[J]. 中华医学遗传学杂志, 2012, 29(6):631-634. |
| Chen RM, Zhang Y, Yang XH, et al. Analysis of a family affected with familial male-limited precocious puberty due to a Ala568Val mutation in LHCGR gene[J]. Chin J Med Genet, 2012, 29(6):631-634. | |
| [13] | Yano K, Saji M, Hidaka A, et al. A new constitutively activating point mutation in the luteinizing hormone/choriogonadotropin receptor gene in cases of male-limited precocious puberty[J]. J Clin Endocrinol Metab, 1995, 80(4):1162-1168. |
| [14] | 杨海花, 陈永兴, 卫海燕. LHCGR基因突变所致家族性男性性早熟家系分析[J]. 中国临床医学, 2020, 27(1):102-105. |
| Yang HH, Chen YX, Wei HY. Analysis of a family affected with familial male-limited precocious puberty due to a mutation in LHCGR gene[J]. Chin J Clin Med, 2020, 27(1):102-105. | |
| [15] |
Kor Y. Central precocious puberty in a case of late-diagnosed familial testotoxicosis and long-term treatment monitoring[J]. Hormones (Athens), 2018, 17(2):275-278.
doi: 10.1007/s42000-018-0029-1 pmid: 29858851 |
| [16] |
Eyssette-Guerreau S, Pinto G, Sultan A, et al. Effectiveness of anastrozole and cyproterone acetate in two brothers with familial male precocious puberty[J]. J Pediatr Endocrinol Metab, 2008, 21(10):995-1002.
pmid: 19209621 |
| [17] |
Daussac A, Barat P, Servant N, et al. Testotoxicosis without testicular mass: revealed by peripheral precocious puberty and confirmed by somatic LHCGR gene mutation[J]. Endocr Res, 2020, 45(1):32-40.
doi: 10.1080/07435800.2019.1645163 pmid: 31394950 |
| [18] |
王敏, 李敏, 刘悦笙, 等. LHCGR基因突变(Asp578His)致家族性男性性早熟1例临床特点及基因分析[J]. 中国当代儿科杂志, 2017, 19(11):1159-1164.
pmid: 29132462 |
|
Wang M, Li M, Liu YS, et al. Familial male-limited precocious puberty due to Asp578His mutations in the LHCGR gene: clinical characteristics and gene analysis in an infant[J]. Chin J Contemp Pediatr, 2017, 19(11):1159-1164.
pmid: 29132462 |
|
| [19] |
Siviero-Miachon AA, Kizys MM, Ribeiro MM, et al. Cosegregation of a novel mutation in the sixth transmembrane segment of the luteinizing/choriogonadotropin hormone receptor with two Brazilian siblings with severe testotoxicosis[J]. Endocr Res, 2017, 42(2):117-124.
doi: 10.1080/07435800.2016.1217005 pmid: 27532428 |
| [20] |
Martin MM, Wu SM, Martin AL, et al. Testicular seminoma in a patient with a constitutively activating mutation of the luteinizing hormone/chorionic gonadotropin receptor[J]. Eur J Endocrinol, 1998, 139(1):101-106.
pmid: 9703386 |
| [21] |
Müller J, Gondos B, Kosugi S, et al. Severe testotoxicosis phenotype associated with Asp578-->Tyr mutation of the lutrophin/choriogonadotrophin receptor gene[J]. J Med Genet, 1998, 35(4):340-341.
pmid: 9598734 |
| [22] |
Gurnurkar S, DiLillo E, Carakushansky M. A case of familial male-limited precocious puberty with a novel mutation[J]. J Clin Res Pediatr Endocrinol, 2021, 13(2):239-244.
doi: 10.4274/jcrpe.galenos.2020.2020.0067 URL |
| [23] |
Laue L, Wu SM, Kudo M, et al. Heterogeneity of activating mutations of the human luteinizing hormone receptor in male-limited precocious puberty[J]. Biochem Mol Med, 1996, 58(2):192-198.
doi: 10.1006/bmme.1996.0048 pmid: 8812739 |
| [24] |
Nagasaki K, Katsumata N, Ogawa Y, et al. Novel C617Y mutation in the 7th transmembrane segment of luteinizing hormone/choriogonadotropin receptor in a Japanese boy with peripheral precocious puberty[J]. Endocr J, 2010, 57(12):1055-1060.
pmid: 21060208 |
| [25] |
Schedewie HK, Reiter EO, Beitins IZ, et al. Testicular leydig cell hyperplasia as a cause of familial sexual precocity[J]. J Clin Endocrinol Metab, 1981, 52(2):271-278.
doi: 10.1210/jcem-52-2-271 URL |
| [26] |
Shenker A, Laue L, Kosugi S, et al. A constitutively activating mutation of the luteinizing hormone receptor in familial male precocious puberty[J]. Nature, 1993, 365(6447):652-654.
doi: 10.1038/365652a0 URL |
| [27] |
Roy N, Mascolo E, Lazzaretti C, et al. Endocrine disruption of the follicle-stimulating hormone receptor signaling during the human antral follicle growth[J]. Front Endocrinol (Lausanne), 2021, 12:791763.
doi: 10.3389/fendo.2021.791763 URL |
| [28] | Qiao J, Han B. Diseases caused by mutations in luteini-zing hormone/chorionic gonadotropin receptor[J]. Prog Mol Biol Transl Sci, 2019, 161:69-89. |
| [29] | Kremer H, Martens JW, van Reen M, et al. A limited repertoire of mutations of the luteinizing hormone (LH) receptor gene in familial and sporadic patients with male LH-independent precocious puberty[J]. J Clin Endocrinol Metab, 1999, 84(3):1136-1140. |
| [30] |
Kosugi S, Van Dop C, Geffner ME, et al. Characterization of heterogeneous mutations causing constitutive activation of the luteinizing hormone receptor in familial male precocious puberty[J]. Hum Mol Genet, 1995, 4(2):183-188.
doi: 10.1093/hmg/4.2.183 pmid: 7757065 |
| [31] |
Boot AM, Lumbroso S, Verhoef-Post M, et al. Mutation analysis of the LH receptor gene in Leydig cell adenoma and hyperplasia and functional and biochemical studies of activating mutations of the LH receptor gene[J]. J Clin Endocrinol Metab, 2011, 96(7):E1197-E1205.
doi: 10.1210/jc.2010-3031 URL |
| [32] |
Juel Mortensen L, Blomberg Jensen M, Christiansen P, et al. Germ cell neoplasia in situ and preserved fertility despite suppressed gonadotropins in a patient with testotoxicosis[J]. J Clin Endocrinol Metab, 2017, 102(12):4411-4416.
doi: 10.1210/jc.2017-01761 pmid: 29029242 |
| [33] |
Soriano-Guillén L, Lahlou N, Chauvet G, et al. Adult height after ketoconazole treatment in patients with familial male-limited precocious puberty[J]. J Clin Endocrinol Metab, 2005, 90(1):147-151.
doi: 10.1210/jc.2004-1438 URL |
| [34] |
Lane LC, Flowers J, Johnstone H, et al. Adult height in patients with familial male-limited precocious puberty and the role of an aromatase inhibitor in patient management[J]. J Pediatr Endocrinol Metab, 2018, 31(5):551-560.
doi: 10.1515/jpem-2017-0363 pmid: 29654692 |
| [35] |
Fanelli F, Verhoef-Post M, Timmerman M, et al. Insight into mutation-induced activation of the luteinizing hormone receptor: molecular simulations predict the functional behavior of engineered mutants at M398[J]. Mol Endocrinol, 2004, 18(6):1499-1508.
doi: 10.1210/me.2003-0050 pmid: 15016840 |
| [36] |
Latronico AC, Brito VN, Carel JC. Causes, diagnosis, and treatment of central precocious puberty[J]. Lancet Diabetes Endocrinol, 2016, 4(3):265-274.
doi: 10.1016/S2213-8587(15)00380-0 URL |
| [37] | 中华医学会儿科学分会内分泌遗传代谢学组,《中华儿科杂志》编辑委员会. 中枢性性早熟诊断与治疗共识(2015)[J]. 中华儿科杂志, 2015, 53(6):412-418. |
| Endocrine Genetic Metabolism Group of Pediatric Branch of Chinese Medical Association, Editorial Committee of Chinese Journal of Pediatrics. Consensus on diagnosis and treatment of central precocious puberty(2015)[J]. Chin J Pediatr, 2015, 53(6):412-418. | |
| [38] | Laue L, Jones J, Barnes KM, et al. Treatment of familial male precocious puberty with spironolactone, testolactone, and deslorelin[J]. J Clin Endocrinol Metab, 1993, 76(1):151-155. |
| [39] |
Mitre N, Lteif A. Treatment of familial male-limited precocious puberty (testotoxicosis) with anastrozole and bicalutamide in a boy with a novel mutation in the luteinizing hormone receptor[J]. J Pediatr Endocrinol Metab, 2009, 22(12):1163-1167.
pmid: 20333877 |
| [40] |
Leschek EW, Flor AC, Bryant JC, et al. Effect of antiandrogen, aromatase inhibitor, and gonadotropin-releasing hormone analog on adult height in familial male precocious puberty[J]. J Pediatr, 2017, 190:229-235.
doi: 10.1016/j.jpeds.2017.07.047 URL |
| [41] |
Wit JM, Hero M, Nunez SB. Aromatase inhibitors in pediatrics[J]. Nat Rev Endocrinol, 2011, 8(3):135-147.
doi: 10.1038/nrendo.2011.161 pmid: 22024975 |
| [1] | 李林, 安静静, 王俊祺, 王歆琼, 董治亚. 16S rRNA第二代测序技术分析特发性身材矮小儿童肠道菌群构成的特征及相关发病机制研究[J]. 诊断学理论与实践, 2021, 20(02): 149-154. |
| [2] | 马晓宇, 杨媛艳, 陆文丽, 倪继红, 王俊琪, 陈烨, 秦雪艳, 董治亚, 王伟. 晨尿促性腺激素全定量测定在前瞻性鉴别女童中枢性性早熟进展类型中的应用价值[J]. 诊断学理论与实践, 2020, 19(05): 516-520. |
| [3] | 马晓宇, 陆文丽, 倪继红, 王俊琪, 陈烨, 秦雪艳, 董治亚, 王伟. 尿促性腺激素全定量测定在预测女童乳房早发育类型中的应用价值[J]. 诊断学理论与实践, 2019, 18(03): 291-295. |
| [4] | 黄亚, 徐利, 葛凤菊, 吴鋆龙, 陈亚宁, 祁秀娟. 激光辅助孵化完全去除透明带对冷冻单囊胚移植结局的影响[J]. 诊断学理论与实践, 2019, 18(03): 334-339. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||