诊断学理论与实践 ›› 2024, Vol. 23 ›› Issue (06): 612-618.doi: 10.16150/j.1671-2870.2024.06.008
陆弘逾1, 刘宏2, 宋陆茜2( )
)
收稿日期:2024-04-05
出版日期:2024-12-25
发布日期:2024-12-25
通讯作者:
宋陆茜 E-mail:songluxi@139.com基金资助:
LU Hongyu1, LIU Hong2, SONG Luxi2()
Received:2024-04-05
Published:2024-12-25
Online:2024-12-25
摘要:
目的: 分析总结T细胞大颗粒淋巴细胞白血病(T-cell large granular lymphocyte leukemia,T-LGLL)患者的临床及实验室特征,探讨T-LGLL的诊断及治疗。方法: 回顾性分析2019年3月至2022年12月期间,本院收治的6例连续T-LGLL患者的临床资料,分析总结其细胞形态学、骨髓细胞免疫表型检测、基因检测结果及治疗方案,并进行随访。结果: 6例T-LGLL患者诊断时中位年龄为60岁(54~70岁)。6例患者就诊时均有贫血,其中3例需要输血,3例出现脾脏肿大,1例有淋巴结肿大。6例外周血大颗粒淋巴细胞(large granular lymphocyte,LGL)形态学特征典型,但均为低绝对值计数,中位计数1.0(0.4~1.4)×109/L。骨髓细胞免疫表型检测显示,所有患者LGL细胞均来源于胸腺后成熟T细胞,其中4例表达常见的CD3+CD8+CD57+效应T细胞特征,2例表达少见的CD3+CD8+CD57-记忆T细胞标记。基因检测显示,6例患者T细胞受体(T cell receptor,TCR)中均能检测到不同的单克隆片段,支持T细胞的异常克隆性。二代基因测序结果显示,6例患者中4例检测到STAT3突变。6例患者均接受免疫抑制治疗,随访显示,5例患者对治疗有反应,其中5例获得了持续的血液学缓解。结论: T-LGLL单独依靠典型的细胞形态学及LGL绝对计数,不足以对T-LGLL作出早期和准确诊断,而LGL免疫表型也存在较大的差异,所以应联合形态学、免疫学、TCR克隆分析、二代基因测序分子生物学数据的多参数综合诊断。目前患者对免疫抑制治疗反应良好。
中图分类号:
陆弘逾, 刘宏, 宋陆茜. T细胞大颗粒淋巴细胞白血病6例临床及实验室特征分析[J]. 诊断学理论与实践, 2024, 23(06): 612-618.
LU Hongyu, LIU Hong, SONG Luxi. Analysis of clinical and laboratory characteristics of six cases with T-cell large granular lymphocytic leukemia[J]. Journal of Diagnostics Concepts & Practice, 2024, 23(06): 612-618.
表1
T-LGLL患者的临床特征
| No. | Gender (Male/Femal) | Age (Years) | Clinical symptoms | Time to diagnosis (month) | WBC (×109/L) | ANC (×109/L) | HGB (g/L) | Plt (×109/L) | LYM (%) | Absolute count of LGL(×109/L) |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | M | 59 | Anaemia,TD,splenomegaly | 87 | 2.5 | 0.4 | 49 | 15 | 80.8 | 0.4 |
| 2 | F | 57 | Anaemia, fever, lymphadenopathy | 13 | 3.6 | 1.4 | 63 | 46 | 52.2 | 1.0 |
| 3 | F | 68 | Anaemia,TD | 60 | 3.1 | 1.8 | 61 | 242 | 40.5 | 0.6 |
| 4 | F | 70 | Anaemia | 6 | 2.3 | 0.7 | 65 | 135 | 62.5 | 1.2 |
| 5 | M | 54 | anaemia,splenomegaly | 12 | 5.4 | 1.6 | 67 | 167 | 68.0 | 1.4 |
| 6 | M | 61 | Anaemia splenomegaly | 12 | 3.5 | 2.0 | 37 | 377 | 43.0 | 0.9 |
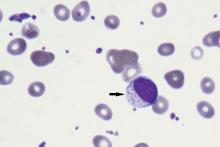
图1
T细胞大颗粒淋巴细胞白血病外周血细胞学形态学特征 注:血涂片显示染色质浓集,细胞核轻度不规则,细胞质丰富淡染,含有不同数量的嗜苯胺蓝颗粒(箭头)(瑞氏染色,×100)。

表2
T-LGLL患者的免疫表型
| No. | Proportion of T-LGL(%) | mCD3 | CD4 | CD8 | CD5 | CD7 | CD2 | TCRαβ | TCRγδ | CD57 | CD56 | CD16 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 9.6 | + | - | + | Dim | + | + | + | - | - | - | - |
| 2 | 13.6 | + | - | + | ND | P+ | + | + | - | P+ | - | - |
| 3 | 1.8 | + | - | + | Dim | + | + | + | - | - | - | - |
| 4 | 66.5 | + | - | + | - | Dim | + | + | - | + | - | - |
| 5 | 34.2 | + | - | + | Dim | Dim | + | + | - | + | - | + |
| 6 | 9.6 | + | + | + | + | + | + | + | - | + | - | - |
表3
T-LGLL T细胞克隆性检测、遗传学和分子生物学特征
| No. | TCR rearrangement | Gene segments | Karyotypy | NGS mutation | Location | VAF(%) |
|---|---|---|---|---|---|---|
| 1 | TCRD+ TCRB+ | Vδ+Dδ+Jδ regions 152.01 bp Vβ+Jβ1/2 regions 265.45 bp | 46,XY[5] | STAT3 | Y640F | 24.5 |
| 2 | TCRB+ TCRG+ | Vβ+Jβ1/2 regions 167 bp Vγf-Jg1.3/2.3 regions 219 bp | 46,XX[8] | EP300 KMT2D | A922E P530A | 55 51.4 |
| 3 | TCRB+ TCRG+ | Vβ+Jβ1/2 regions 189 bp Vγ10-Jγ1.3/2.3 regions 219 bp | 46,XX[20] | STAT3 APC | Y640F T1496S | 3 49.1 |
| 4 | TCRD+ TCRB+ TCRG+ | Vδ+Dδ+Jδregions 212 bp Vβ+Jβ1/2 regions 184 bp Vγ10-Jγ1.3/2.3 regions 164 bp | 46,XX[1] | STAT3 KMT2D TP53 | S614R R2471* E271A | 28 5.8 50.9 |
| 5 | TCRB+ | Vβ+Jβ1/2 regions 179 bp | 46,XY[20] | TET2 | M1522I | 46.6 |
| 6 | TCRB+ TCRG+ | Vβ+Jβ1/2 regions 257 and 262 bp Vγ10-Jγ1.3/2.3 regions 148 bp Vγf-Jg1.3/2.3 regions 216 bp Vγf-Jg1.1/2.1 regions 237 bp | 46,XY[20] | STAT3 KMT2D ANKRD11 | Y640F Q2341Gfs Y808C | 7.9 3.8 47.1 |
| [1] | SHAH M V, HOOK C C, CALL T G, et al. A population-based study of large granular lymphocyte leukemia[J]. Blood Cancer J, 2016, 6(8):e455. |
| [2] |
ALAGGIO R, AMADOR C, ANAGNOSTOPOULOS I, et al. The 5th edition of the World Health Organization classification of haematolymphoid tumours: lymphoid neoplasms[J]. Leukemia, 2022, 36(7):1720-1748.
doi: 10.1038/s41375-022-01620-2 pmid: 35732829 |
| [3] | 中国中西医结合学会检验医学专业委员会. 流式细胞术临床检验图文报告书写专家共识[J]. 中华检验医学杂志, 2024, 47(7):729-739. |
| Chinese Society of Integrated Traditional Chinese and Western Medicine Laboratory Medicine Professional Committee. Expert consensus on writing graphic and textual reports for clinical testing of flow cytometry[J]. Chin J Lab Med, 2024, 47(7):729-739. | |
| [4] | JAFFE E S, ARBER D A, CAMPO E, et al. Hematopathology 2nd[J]. Elsevier, 2017,599-608. |
| [5] |
DONG N, CASTILLO TOKUMORI F, et al. Large granular lymphocytic leukemia - a retrospective study of 319 cases[J]. Am J Hematol, 2021, 96(7):772-780.
doi: 10.1002/ajh.26183 pmid: 33819354 |
| [6] | ZHU Y, GAO Q, HU J, et al. Clinical features and treatment outcomes in patients with T-cell large granular lymphocytic leukemia: a single-institution experience[J]. Leuk Res, 2020, 90:106299. |
| [7] |
MOHAN S R, MACIEJEWSKI J P. Diagnosis and therapy of neutropenia in large granular lymphocyte leukemia[J]. Curr Opin Hematol, 2009, 16(1):27-34.
doi: 10.1097/MOH.0b013e32831c8407 pmid: 19057202 |
| [8] | 石茵, 李元媛, 刘燕, 等. 髓系肿瘤合并克隆性T大颗粒淋巴细胞增殖的临床及实验室特征[J]. 中华血液学杂志, 2020, 41(4):276-281. |
| SHI Y, LI Y Y, LIU Y, et al. Clinical and laboratory characteristics of clonal T large granular lymphocyte proliferation in myeloid tumors[J]. Chin J Hematol, 2020, 41(4):276-281. | |
| [9] |
BAREAU B, REY J, HAMIDOU M, et al. Analysis of a French cohort of patients with large granular lymphocyte leukemia: a report on 229 cases[J]. Haematologica, 2010, 95(9):1534-1541.
doi: 10.3324/haematol.2009.018481 pmid: 20378561 |
| [10] |
CLEMENTE M J, WLODARSKI M W, MAKISHIMA H, et al. Clonal drift demonstrates unexpected dynamics of the T-cell repertoire in T-large granular lymphocyte leukemia[J]. Blood, 2011, 118(16):4384-4393.
doi: 10.1182/blood-2011-02-338517 pmid: 21865345 |
| [11] |
LAMY T, LOUGHRAN T P JR. How I treat LGL leukemia[J]. Blood, 2011, 117:2764-2774.
doi: 10.1182/blood-2010-07-296962 pmid: 21190991 |
| [12] | MELENHORST J J, SORBARA L, KIRBY M, et al. Large granular lymphocyte leukaemia is characterized by a clonal T-cell receptor rearrangement in both memory and effector CD8(+) lymphocyte populations[J]. Br J Haematol, 2001, 112(1):189-194. |
| [13] |
MOIGNET A, HASANALI Z, ZAMBELLO R, et al. Cyclophosphamide as a first-line therapy in LGL leukemia[J]. Leukemia, 2014, 28(5):1134-1136.
doi: 10.1038/leu.2013.359 pmid: 24280867 |
| [1] | 安慧慧, 吴涛, 刘文慧, 田思锐. 91种炎症蛋白水平与急性髓系白血病发病风险相关的孟德尔随机化研究[J]. 诊断学理论与实践, 2024, 23(5): 509-516. |
| [2] | 朱维维, 李倩, 吴凡, 翟志敏. 100例骨髓增生异常性肿瘤患者基因突变及其与临床特征间的关系[J]. 诊断学理论与实践, 2024, 23(03): 305-312. |
| [3] | 刘娟, 殷丽娟, 范德生. AR、SKP2、SOX10、PD-L1及TIL表达在三阴性乳腺癌中的意义[J]. 诊断学理论与实践, 2024, 23(02): 162-172. |
| [4] | 叶向军, 卢兴国. 第5版世界卫生组织造血淋巴肿瘤MDS和AML分类更新解读[J]. 诊断学理论与实践, 2023, 22(05): 421-428. |
| [5] | 张姣, 闾佳佳, 陆文丽, 张莉丹, 李卫. BCR-FIBCD1-ABL1融合基因阳性的儿童慢性粒细胞白血病一例报道并文献复习[J]. 诊断学理论与实践, 2023, 22(05): 472-479. |
| [6] | 石峰, 郭竹英, 郭海艳. 新型冠状病毒肺炎患者外周血淋巴细胞亚群变化的临床意义[J]. 诊断学理论与实践, 2022, 21(05): 619-624. |
| [7] | 郭慧玲, 吴涛, 薛锋, 郭敏, 王存邦, 白海. 侵袭性自然杀伤细胞白血病一例并文献复习[J]. 诊断学理论与实践, 2021, 20(06): 582-583. |
| [8] | 李松涛, 杨大恒, 孙杭, 岳玉林, 张倩, 刘倩琦, 武苏, 马长艳. 甲状腺功能血清学指标结合超声检查在鉴别儿童毒性弥漫性甲状腺肿与慢性淋巴细胞性甲状腺炎中的价值[J]. 诊断学理论与实践, 2020, 19(06): 600-604. |
| [9] | 郭娟娟, 吴涛, 贾占武, 马利, 白海, 王存邦. WT1阳性急性髓细胞性白血病合并唐氏综合征一例报告[J]. 诊断学理论与实践, 2020, 19(05): 531-533. |
| [10] | 高燕婷, 赵金艳, 王娟, 李佳, 许雯, 李莉, 蔺丽慧. 急性髓细胞性白血病患者骨髓淋巴细胞亚群分析及其临床意义[J]. 诊断学理论与实践, 2020, 19(04): 407-413. |
| [11] | 徐娜娜, 吴涛, 寇明坤, 白海. JAK2基因突变在急性髓细胞白血病中的研究进展[J]. 诊断学理论与实践, 2020, 19(02): 195-198. |
| [12] | 彭真萍, 项喜喜, 张苏江, 李佳明. 以类白血病反应为首发表现的慢性中性粒细胞白血病二例并文献复习[J]. 诊断学理论与实践, 2020, 19(02): 122-128. |
| [13] | 来小音, 孙家兰, 胡荣郭, 杨雪莲, 吴国炉, 李龙宣, 卜碧涛. T淋巴细胞亚群失衡与全身型重症肌无力临床症状加重及缓解的相关性研究[J]. 诊断学理论与实践, 2019, 18(2): 199-203. |
| [14] | 田明明, 吴涛, 薛锋, 汉英, 张丽萍, 王存邦, 白海. Ph(+)急性淋巴细胞白血病伴骨髓坏死一例[J]. 诊断学理论与实践, 2019, 18(05): 585-587. |
| [15] | 张弦, 伍平, 王卉, 王彤, 刘红星, 张改玲, 苏云超, 石延泽, 陆佩华. 急性红白血病4例病例讨论及文献复习[J]. 诊断学理论与实践, 2018, 17(06): 718-722. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||