内科理论与实践 ›› 2021, Vol. 16 ›› Issue (03): 188-192.doi: 10.16138/j.1673-6087.2021.03.010
孙超, 姚玮艳( ), 黄佳, 朱颖, 汤玉茗()
), 黄佳, 朱颖, 汤玉茗()
收稿日期:2020-12-23
出版日期:2021-06-25
发布日期:2022-07-26
通讯作者:
姚玮艳,汤玉茗
E-mail:ywy11419@rjh.com.cn;windwindy2000@126.com
SUN Chao, YAO Weiyan(), HUANG Jia, ZHU Ying, TANG Yuming()
Received:2020-12-23
Online:2021-06-25
Published:2022-07-26
Contact:
YAO Weiyan,TANG Yuming
E-mail:ywy11419@rjh.com.cn;windwindy2000@126.com
摘要:
目的:探讨无症状糜烂性食管炎(asymptomatic erosive esophagitis, AEE)的患病率、危险因素、预后及治疗。方法:回顾性分析我院5 184例无症状体检人群的胃镜检查资料,其中475例(9.2%)糜烂性食管炎(erosive esophagitis,EE)纳入AEE组。在无食管炎的人群中选择950名年龄和性别匹配且内镜检查无食管炎的受试者作为对照组。比较2组间的危险因素,分析AEE的独立危险因素、预后及对治疗的反应。结果:高体质量指数(body mass index,BMI)[优势比(odds ratio,OR)=1.101, P=0.001]、脂肪肝(OR=1.635, P=0.013)、食管裂孔疝(OR=2.302, P=0.039)和高γ-谷氨酰转移酶(gamma-glutamyl transferase,GGT)(OR=1.008, P=0.013)是AEE的危险因素。对140例AEE患者的随访发现,无论是否接受治疗,约有2/3患者的食管炎严重程度有所改善(82.4%比65.3%)。此外,质子泵抑制剂(proton pump inhibitor,PPI)治疗组食管炎改善比例远高于未治疗组(P<0.005)。结论:脂肪肝、肥胖、食管裂孔疝及高GGT为AEE危险因素。AEE的预后良好,PPI能明显改善AEE严重程度。
中图分类号:
孙超, 姚玮艳, 黄佳, 朱颖, 汤玉茗. 无症状糜烂性食管炎的危险因素分析[J]. 内科理论与实践, 2021, 16(03): 188-192.
SUN Chao, YAO Weiyan, HUANG Jia, ZHU Ying, TANG Yuming. Risk factors of asymptomatic erosive esophagitis[J]. Journal of Internal Medicine Concepts & Practice, 2021, 16(03): 188-192.
表1
AEE组与对照组临床特点及实验室检查比较[n(%)/$\bar{x}\pm s$]
| 临床特点 | 对照组 (n=950) | AEE组 (n=475) | t/χ2 | P |
|---|---|---|---|---|
| 年龄(岁) | 51.63±0.30 | 51.63±0.43 | -0.012 | 0.963 |
| 男性[n(%)] | 790(83.2) | 395(83.2) | 0 | |
| BMI(kg/m2) | 23.01±0.10 | 23.95±0.15 | 5.177 | 0.001 |
| 食管裂孔疝[n(%)] | 63(6.6) | 62(13.1) | 2.526 | <0.001 |
| C反应蛋白(mg/L) | 1.6±0.2 | 1.4±0.08 | 0.741 | 0.045 |
| 白细胞计数(×109/L) | 6.11±0.07 | 6.16±0.09 | -0.434 | 0.669 |
| 红细胞计数(×1012/L) | 4.87±0.02 | 4.94±0.03 | -1.987 | 0.091 |
| 血红蛋白(g/L) | 148.03±0.57 | 150.18±0.80 | -2.222 | 0.031 |
| 血小板(×109/L) | 208.05±2.17 | 207.81±3.15 | 0.065 | 0.866 |
| 糖化血红蛋白(%) | 5.62±0.03 | 5.75±0.05 | 2.526 | 0.003 |
| 空腹血糖(mmol/L) | 5.52±0.04 | 5.60±0.06 | 1.172 | 0.242 |
| 胰岛素抵抗(mmol·mU/L2) | 2.24±0.11 | 2.84±0.19 | 3.251 | 0.001 |
| 前白蛋白(mg/L) | 288.02±2.04 | 288.32±2.99 | 0.035 | 0.696 |
| 谷丙转氨酶(U/L) | 28.36±0.70 | 28.95±1.01 | 0.406 | 0.534 |
| 谷草转氨酶(U/L) | 24.56±0.41 | 24.25±0.46 | -0.666 | 0.800 |
| 碱性磷酸酶(U/L) | 67.67±0.70 | 69.06±1.05 | 1.434 | 0.252 |
| GGT(U/L) | 35.69±1.39 | 44.27±3.01 | 3.007 | 0.034 |
| 总胆红素(μmol/L) | 15.62±0.23 | 15.54±0.35 | -0.512 | 0.678 |
| 直接胆红素(μmol/L) | 2.562±0.04 | 2.515±0.05 | -0.699 | 0.692 |
| 总蛋白(g/L) | 72.45±0.17 | 72.33±0.21 | -0.694 | 0.938 |
| 白蛋白(g/L) | 44.80±0.12 | 44.75±0.16 | -0.107 | 0.694 |
| 总胆汁酸(μmol/L) | 3.50±0.11 | 3.99±0.28 | 1.527 | 0.823 |
| 血尿素氮(mmol/L) | 5.31±0.05 | 5.21±0.06 | -1.576 | 0.306 |
| 肌酐(μmol/L) | 80.16±0.51 | 80.42±0.78 | 0.522 | 0.935 |
| 尿酸(μmol/L) | 344.70±2.94 | 356.32±4.19 | 2.243 | 0.041 |
| 三酰甘油(mmol/L) | 1.82±0.06 | 1.85±0.07 | 0.165 | 0.192 |
| 总胆固醇(mmol/L) | 5.12±0.04 | 5.13±0.05 | 0.247 | 0.940 |
| 高密度脂蛋白(mmol/L) | 1.30±0.01 | 1.30±0.02 | -0.836 | 0.298 |
| 低密度脂蛋白(mmol/L) | 3.17±0.03 | 3.17±0.04 | 0.338 | 0.873 |
| 游离脂肪酸(mmol/L) | 0.49±0.01 | 0.52±0.02 | 1.240 | 0.237 |
| 游离三碘甲状腺原氨酸(pmol/L) | 4.48±0.02 | 4.44±0.04 | -0.903 | 0.183 |
| 游离甲状腺素(pmol/L) | 13.36±0.07 | 13.22±0.15 | -2.951 | 0.010 |
| 促甲状腺素(mU/L) | 1.95±0.13 | 1.85±0.09 | 1.263 | 0.310 |
| 甲状腺球蛋白抗体 (U/mL) | 9.51±2.14 | 7.69±3.53 | -0.467 | 0.132 |
| 甲状腺过氧化物酶抗体 (U/mL) | 12.65±3.55 | 16.27±6.40 | -0.440 | 0.456 |
| 幽门螺杆菌感染(n/N) | 128/509 | 68/306 | 0.175 | 0.551 |
| 病理 | 72/276 | 43/182 | 0.353 | 0.552 |
| 13C呼气试验 | 16/63 | 13/34 | 1.737 | 0.188 |
| 幽门螺杆菌抗体 | 40/170 | 12/90 | 3.824 | 0.051 |
| 影像学(n/N) | ||||
| 脂肪肝 | 191/429 | 137/244 | 8.414 | 0.004 |
| 胆结石 | 30/429 | 11/244 | 3.087 | 0.195 |
| 胆囊息肉 | 17/429 | 9/244 | 0.031 | 0.859 |
| 肾结石 | 13/429 | 9/244 | 0.213 | 0.644 |
表2
AEE的单因素Logistic分析
| 变量 | P | OR | 95%CI |
|---|---|---|---|
| 脂肪肝 | 0.013 | 1.495 | 1.089~2.052 |
| BMI | 0.001 | 1.093 | 1.056~1.131 |
| GGT | 0.006 | 1.004 | 1.001~1.008 |
| 尿酸 | 0.022 | 1.004 | 1.000~1.004 |
| 胰岛素抵抗 | 0.007 | 1.233 | 1.060~1.434 |
| 糖化血红蛋白 | 0.021 | 1.275 | 1.038~1.566 |
| 血红蛋白 | 0.027 | 1.012 | 1.001~1.023 |
| 食管裂孔疝 | <0.001 | 2.114 | 1.461~3.059 |
表3
AEE多因素Logistic分析
| 变量 | P | OR | 95%CI |
|---|---|---|---|
| 脂肪肝 | 0.013 | 1.635 | 1.111~2.408 |
| GGT | 0.013 | 1.008 | 1.002~1.018 |
| BMI | 0.001 | 1.101 | 1.039~1.166 |
| 食管裂孔疝 | 0.039 | 2.302 | 1.045~5.074 |
表4
AEE的随访结果[n(%)]
| 指标 | PPI治疗组(n=68) | 非治疗组(n=72) |
|---|---|---|
| 进展 | 2(2.9) | 7(9.7) |
| 分级不变 | 10(14.7) | 18(25.0) |
| 改善 | 56(82.4) | 47(65.3) |
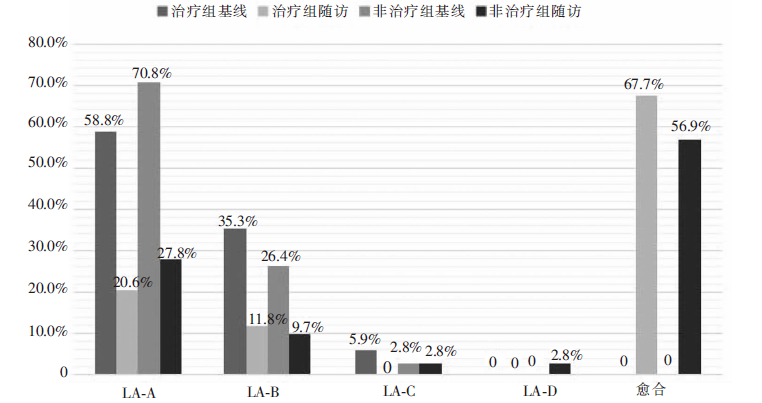
图1
治疗组和非治疗组的基线及随访的内镜结果
| [1] |
Vakil N, van Zanten SV, Kahrilas P, et al. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus[J]. Am J Gastroenterol, 2006, 101(8): 1900-1920.
doi: 10.1111/j.1572-0241.2006.00630.x URL |
| [2] |
Nozu T, Komiyama H. Clinical characteristics of asymptomatic esophagitis[J]. J Gastroenterol, 2008, 43(1): 27-31.
doi: 10.1007/s00535-007-2120-2 URL |
| [3] |
Wang PC, Hsu CS, Tseng TC, et al. Male sex, hiatus hernia, and Helicobacter pylori infection associated with asymptomatic erosive esophagitis[J]. J Gastroenterol Hepatol, 2012, 27(3): 586-591.
doi: 10.1111/j.1440-1746.2011.06881.x URL |
| [4] |
Ronkainen J, Talley NJ, Storskrubb T, et al. Erosive esophagitis is a risk factor for Barrett’s esophagus: a community-based endoscopic follow-up study[J]. Am J Gastroenterol, 2011, 106(11): 1946-1952.
doi: 10.1038/ajg.2011.326 pmid: 21946284 |
| [5] |
Lundell LR, Dent J, Bennett JR, et al. Endoscopic assessment of oesophagitis: clinical and functional correlates and further validation of the Los Angeles classification[J]. Gut, 1999, 45(2): 172-180.
pmid: 10403727 |
| [6] | Lee CL, Liu CC, Liao CC, et al. Reuse of CLO test in the diagnosis of Helicobacter pylori infection[J]. J Formos Med Assoc, 2002, 101(4): 298-300. |
| [7] |
Ferwana M, Abdulmajeed I, Alhajiahmed A, et al. Accuracy of urea breath test in Helicobacter pylori infection: meta-analysis[J]. World J Gastroenterol, 2015, 21(4): 1305-1314.
doi: 10.3748/wjg.v21.i4.1305 URL |
| [8] | 中华医学会消化病学分会. 2014年中国胃食管反流病专家共识意见[J]. 中华消化杂志, 2014, 34(10): 649-661. |
| [9] |
Lee SP, Sung IK, Kim JH, et al. The clinical features and predisposing factors of asymptomatic erosive esophagitis[J]. Dig Dis Sci, 2016, 61(12): 3522-3529.
doi: 10.1007/s10620-016-4341-9 URL |
| [10] |
Lei WY, Yu HC, Wen SH, et al. Predictive factors of silent reflux in subjects with erosive esophagitis[J]. Dig Liver Dis, 2015, 47(1): 24-29.
doi: 10.1016/j.dld.2014.09.017 URL |
| [11] |
Peng S, Cui Y, Xiao YL, et al. Prevalence of erosive esophagitis and Barrett’s esophagus in the adult Chinese population[J]. Endoscopy, 2009, 41(12): 1011-1017.
doi: 10.1055/s-0029-1215291 pmid: 19967617 |
| [12] |
Cho JH, Kim HM, Ko GJ, et al. Old age and male sex are associated with increased risk of asymptomatic erosive esophagitis: analysis of data from local health examinations by the Korean National Health Insurance Corporation[J]. J Gastroenterol Hepatol, 2011, 26(6): 1034-1038.
doi: 10.1111/j.1440-1746.2011.06686.x URL |
| [13] |
Lee D, Lee KJ, Kim KM, et al. Prevalence of asymptomatic erosive esophagitis and factors associated with symptom presentation of erosive esophagitis[J]. Scand J Gastroenterol, 2013, 48(8): 906-912.
doi: 10.3109/00365521.2013.812236 URL |
| [14] |
Wang FW, Tu MS, Chuang HY, et al. Erosive esophagitis in asymptomatic subjects: risk factors[J]. Dig Dis Sci, 2010, 55(5): 1320-1324.
doi: 10.1007/s10620-009-0888-z URL |
| [15] |
Singh S, Sharma AN, Murad MH, et al. Central adiposity is associated with increased risk of esophageal inflammation, metaplasia, and adenocarcinoma: a systematic review and meta-analysis[J]. Clin Gastroenterol Hepatol, 2013, 11(11): 1399-1412.
doi: 10.1016/j.cgh.2013.05.009 URL |
| [16] |
Loke SS, Yang KD, Chen KD, et al. Erosive esophagitis associated with metabolic syndrome, impaired liver function, and dyslipidemia[J]. World J Gastroenterol, 2013, 19(35): 5883-5888.
doi: 10.3748/wjg.v19.i35.5883 URL |
| [17] |
Gunji T, Sato H, Iijima K, et al. Risk factors for erosive esophagitis: a cross-sectional study of a large number of Japanese males[J]. J Gastroenterol, 2011, 46(4): 448-455.
doi: 10.1007/s00535-010-0359-5 URL |
| [18] |
Lee SW, Lien HC, Chang CS, et al. Association of metabolic syndrome with erosive esophagitis and Barrett’s esophagus in a Chinese population[J]. J Chin Med Assoc, 2017, 80(1): 15-18.
doi: 10.1016/j.jcma.2016.08.007 URL |
| [19] |
Kim TJ, Lee H, Baek SY, et al. Metabolically healthy obesity and the risk of erosive esophagitis: a cohort study[J]. Clin Transl Gastroenterol, 2019, 10(9): e00077.
doi: 10.14309/ctg.0000000000000077 URL |
| [20] |
Park JH, Park DI, Kim HJ, et al. Metabolic syndrome is associated with erosive esophagitis[J]. World J Gastroenterol, 2008, 14(35): 5442-5447.
doi: 10.3748/wjg.14.5442 URL |
| [21] |
Tai CM, Lee YC, Tu HP, et al. The relationship between visceral adiposity and the risk of erosive esophagitis in severely obese Chinese patients[J]. Obesity (Silver Spring), 2010, 18(11): 2165-2169.
doi: 10.1038/oby.2010.143 URL |
| [22] |
Yucel O. Interactions between Helicobacter pylori and gastroesophageal reflux disease[J]. Esophagus, 2019, 16(1): 52-62.
doi: 10.1007/s10388-018-0637-5 pmid: 30151653 |
| [23] | Xie T, Cui X, Zheng H, et al. Meta-analysis: eradication of Helicobacter pylori infection is associated with the development of endoscopic gastroesophageal reflux disease[J]. Eur J Gastroenterol Hepatol, 2013, 25(10): 1195-1205. |
| [24] |
Corley DA, Kubo A, Levin TR, et al. Helicobacter pylori and gastroesophageal reflux disease: a case-control study[J]. Helicobacter, 2008, 13(5): 352-360.
doi: 10.1111/j.1523-5378.2008.00624.x URL |
| [25] |
Lai EJ, Calderwood AH, Doros G, et al. The Boston bowel preparation scale: a valid and reliable instrument for colonoscopy-oriented research[J]. Gastrointest Endosc, 2009, 69(3 Pt 2): 620-625.
doi: 10.1016/j.gie.2008.05.057 URL |
| [26] |
Min YW, Kim Y, Gwak GY, et al. Non-alcoholic fatty liver disease and the development of reflux esophagitis: a cohort study[J]. J Gastroenterol Hepatol, 2018, 33(5): 1053-1058.
doi: 10.1111/jgh.14042 URL |
| [27] |
Choi JS, Kim HM, Yang YJ, et al. Fatty liver disease and the risk of erosive oesophagitis in the Korean population: a cross-sectional study[J]. BMJ Open, 2019, 9(1): e023585.
doi: 10.1136/bmjopen-2018-023585 URL |
| [28] | Jung SH, Oh JH, Kang SG. Clinical characteristics and natural history of asymptomatic erosive esophagitis[J]. Turk J Gastroenterol, 2014, 25(3): 248-252. |
| [1] | 孙超, 黄佳, 朱颖, 姚玮艳, 汤玉茗. 无症状糜烂性食管炎与结直肠息肉的关系[J]. 内科理论与实践, 2022, 17(03): 233-237. |
| [2] | 杨建军, 宋致成, 顾岩. 肥胖合并食管裂孔疝的外科治疗策略[J]. 外科理论与实践, 2021, 26(5): 394-398. |
| [3] | 胡志伟, 汪忠镐, 吴继敏. 胃食管反流病的外科手术治疗[J]. 外科理论与实践, 2021, 26(5): 399-403. |
| [4] | 王虹. 胃食管反流病的临床表现分类及精准治疗策略[J]. 诊断学理论与实践, 2021, 20(03): 251-256. |
| [5] | 赵雨娉, 汤玉茗, 姚玮艳. 应用固态高分辨率食管测压检测胃食管反流病的研究进展[J]. 内科理论与实践, 2021, 16(01): 64-66. |
| [6] | 徐蓓莉, 邹燕婷, 罗添成, 蔡瑜, 张顺财,. 舒必利对非糜烂性胃食管反流病的疗效分析[J]. 内科理论与实践, 2020, 15(02): 105-110. |
| [7] | 花荣, 姚琪远. 病态肥胖伴胃食管反流病的减重术式选择[J]. 外科理论与实践, 2018, 23(06): 499-501. |
| [8] | 唐陈月, 徐琛莹, 俞丽芬. 上海12 293例体检人群中酸相关性疾病的内镜检出特征分析[J]. 诊断学理论与实践, 2018, 17(01): 51-55. |
| [9] | 花荣, 陈浩, 丁锐, 许博, 沈奇伟, 姚琪远,. 袖状胃切除手术前后的胃食管反流病[J]. 外科理论与实践, 2017, 22(06): 493-498. |
| [10] | 张成, 克力木, 汪忠镐,. 胃食管反流病如何选择抗反流术式[J]. 外科理论与实践, 2016, 21(02): 114-117. |
| [11] | 田书瑞, 吴继敏, 汪忠镐, 胡志伟, 纪涛, 邓昌荣, 战秀岚, 田鑫帅, 张玉, 马松松,. 防粘连复合补片在腹腔镜食管裂孔疝修补术中的应用[J]. 外科理论与实践, 2016, 21(02): 126-129. |
| [12] | 汤玉茗, 钱爱华, 朱颖, 姚玮艳, 黄佳,. 难治性与非难治性胃食管反流病食管动力比较[J]. 内科理论与实践, 2015, 10(06): 418-420. |
| [13] | 吴云林, 毛峻岭, 吴巍, 黄天生, 陆敏, 陈晓敏, 罗方秀, 陆亭伟, 袁晓琴, 李佑, 项明,. 2013年上海嘉定地区胃镜筛查胃癌漏诊的临床研究[J]. 诊断学理论与实践, 2014, 13(04): 383-387. |
| [14] | 吴云林, 王晓瑜,. 胃癌的内镜早期诊断[J]. 诊断学理论与实践, 2014, 13(04): 349-352. |
| [15] | 张伟, 仇明, 单成祥, 姜治国, 刘晟, 江道振, 郑向民, 沈宏亮,. 复合补片和生物补片治疗食管裂孔疝的疗效对比研究[J]. 外科理论与实践, 2014, 19(02): 145-148. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||