内科理论与实践 ›› 2025, Vol. 20 ›› Issue (03): 216-223.doi: 10.16138/j.1673-6087.2025.03.06
虞美玲, 李娇琰, 黎健, 陈影, 赵冰, 毛恩强, 杨之涛( )
)
收稿日期:2025-04-14
出版日期:2025-06-28
发布日期:2025-09-01
通讯作者:
杨之涛
E-mail:yangzhitao@hotmail.fr
YU Meiling, LI Jiaoyan, LI Jian, CHEN Ying, ZHAO Bing, MAO Enqiang, YANG Zhitao()
Received:2025-04-14
Online:2025-06-28
Published:2025-09-01
Contact:
YANG Zhitao
E-mail:yangzhitao@hotmail.fr
摘要:
目的:研究重症监护室患者中粪便艰难梭菌毒素检测阳性对临床预后的影响及危险因素。 方法:方法:回顾性分析2013—2022年间上海交通大学医学院附属瑞金医院急诊重症监护室收治的2 036例患者,比较粪便艰难梭菌毒素检测阳性组(n=225)与阴性组(n=1 811)的临床预后。采用多因素Logistic回归分析艰难梭菌毒素阳性的危险及保护因素。 结果:粪便检测艰难梭菌毒素检测阳性组患者住院时间显著延长(B=18.734 d,95%CI:14.683~22.785),治疗费用明显升高(B=68 854.912元, 95%CI :46 579.159~91 130.665),但2组死亡率差异无统计学意义。多因素分析显示,碳青霉烯类抗菌药物(OR=1.58,95%CI:1.16~2.15),血流感染(OR=1.77,95%CI: 1.17~2.66)和胆道感染(OR=1.79,95%CI :1.03 ~3.10)与粪便艰难梭菌毒素检测阳性率升高呈相关性,而甲硝唑使用(OR=0.58,95%CI :0.40~0.84)、头孢菌素抗菌药物使用(OR=0.54,95%CI: 0.39~0.74)以及女性(OR=0.60,95%CI :0.44~0.83)是保护因素。 结论:危重症患者粪便中艰难梭菌毒素检测阳性不增加患者死亡率,但会延长住院时间,增加住院费用。
中图分类号:
虞美玲, 李娇琰, 黎健, 陈影, 赵冰, 毛恩强, 杨之涛. 艰难梭菌毒素阳性延长急诊重症患者住院时间并增加费用[J]. 内科理论与实践, 2025, 20(03): 216-223.
YU Meiling, LI Jiaoyan, LI Jian, CHEN Ying, ZHAO Bing, MAO Enqiang, YANG Zhitao. Clostridioides difficile toxin positivity prolongs hospital stay and increases costs for critically ill patients in emergency patients[J]. Journal of Internal Medicine Concepts & Practice, 2025, 20(03): 216-223.

图1
ICU患者艰难梭菌毒素检测结果对预后影响研究患者筛选流程
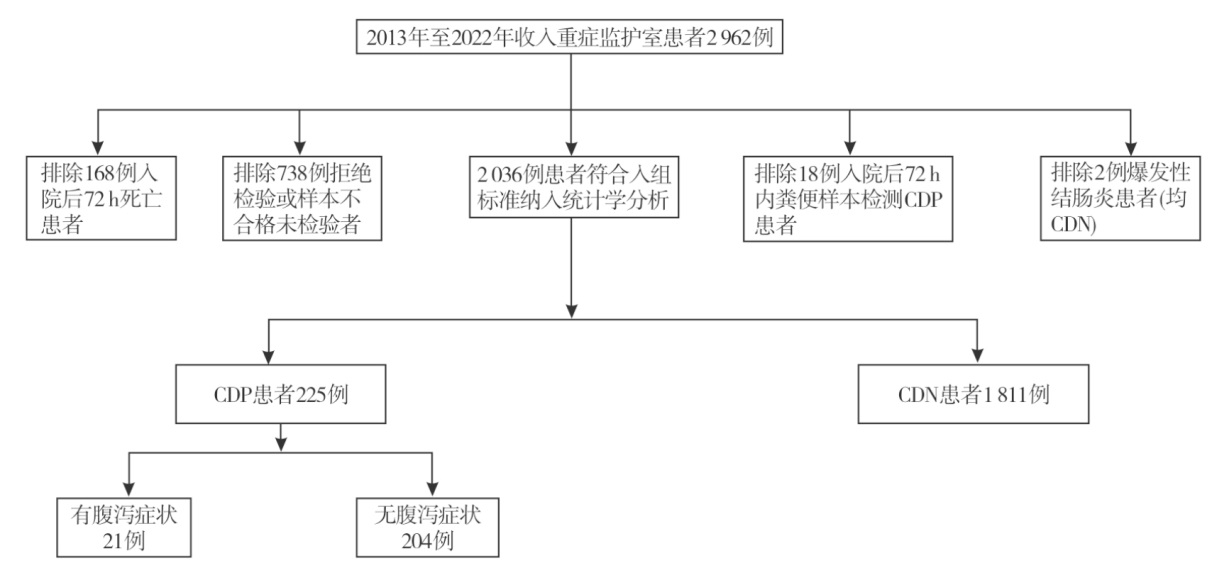
表1
CDP组和CDN组患者基线特征[n(%)/M(P25,P75)]
| 项目 | CDN组(n=1 811) | CDP组(n=225) | χ²/Z | P | |
|---|---|---|---|---|---|
| 年龄(岁) | 55 (39, 69) | 56 (39, 69) | -0.38 | 0.701 | |
| 女性[n(%)] | 664 (36.66) | 58 (25.78) | 10.36 | 0.001 | |
| APACHE Ⅱ | 11.00 (7.00, 16.00) | 11.00 (7.00, 17.00) | -1.24 | 0.217 | |
| 既往病史[n(%)] | |||||
| 冠心病 | 126 (6.96) | 19 (8.44) | 0.67 | 0.415 | |
| 脑卒中 | 118 (6.52) | 18 (8.00) | 0.70 | 0.402 | |
| 急性胰腺炎 | 150 (8.29) | 27 (12.00) | 3.47 | 0.062 | |
| 消化道溃疡 | 48 (2.65) | 5 (2.22) | 0.15 | 0.703 | |
| 实验室指标 | |||||
| 白细胞计数(×109) | 10.90 (7.67, 14.71) | 11.23 (7.60, 15.93) | -1.26 | 0.207 | |
| C反应蛋白(mg/L) | 106.00(23.00,201.70) | 83.00 (16.00, 194.00) | -1.56 | 0.120 | |
| 肌酐(μmol/L) | 73.00 (54.00, 119.00) | 77.00 (58.00, 132.00) | -1.28 | 0.201 | |
| 白蛋白(g/L) | 30.00 (26.00, 34.00) | 30.00 (26.00, 34.00) | -1.20 | 0.229 | |
| 血流感染[n(%)] | 155 (8.56) | 36 (16.00) | 13.04 | <0.001 | |
| 中心静脉导管感染[n(%)] | 140 (7.73) | 25 (11.11) | 3.07 | 0.080 | |
| 胆道感染[n(%)] | 84 (4.64) | 19 (8.44) | 6.04 | 0.014 | |
| 住院治疗[n(%)] | |||||
| 禁食 | 1 389 (76.70) | 168 (74.67) | 0.46 | 0.498 | |
| 肠内营养 | 1 291 (71.29) | 163 (72.44) | 0.13 | 0.717 | |
| 生长抑素 | 534 (29.49) | 63 (28.00) | 0.21 | 0.644 | |
| 质子泵抑制剂 | 1 445(79.79) | 180(80.00) | 0.05 | 0.941 | |
| 免疫球蛋白 | 137 (7.56) | 24 (10.67) | 2.64 | 0.104 | |
| 胸腺肽 | 97 (5.36) | 10 (4.44) | 0.33 | 0.563 | |
| SAID | 751 (41.47) | 102 (45.33) | 1.23 | 0.268 | |
| NSAID | 651 (35.95) | 79 (35.11) | 0.06 | 0.805 | |
| 去甲肾上腺素 | 404 (22.31) | 52 (23.11) | 0.07 | 0.785 | |
| 多巴胺 | 318 (17.56) | 28 (12.44) | 3.71 | 0.054 | |
| 阿片类药物 | 425 (23.47) | 57 (25.33) | 0.39 | 0.535 | |
| CRRT | 285 (15.74) | 36 (16.00) | 0.01 | 0.919 | |
| 机械通气 | 537 (29.65) | 76 (33.78) | 1.62 | 0.203 | |
| 抗菌药物 | |||||
| 种类(种) | 2 (2,3) | 2 (1,4) | -1.41 | 0.160 | |
| 青霉素[n(%)] | 107 (5.91) | 19 (8.44) | 2.22 | 0.136 | |
| 喹诺酮[n(%)] | 493 (27.22) | 48 (21.33) | 3.56 | 0.059 | |
| 碳青霉烯类[n(%)] | 1 034 (57.10) | 155 (68.89) | 11.46 | <0.001 | |
| 万古霉素[n(%)] | 516 (28.49) | 86 (38.22) | 9.10 | 0.003 | |
| 利奈唑胺[n(%)] | 304 (16.79) | 31 (13.78) | 1.32 | 0.251 | |
| 阿米卡星[n(%)] | 91 (5.02) | 12 (5.33) | 0.04 | 0.842 | |
| 甲硝唑[n(%)] | 692 (38.21) | 50 (22.22) | 22.09 | <.001 | |
| 磺胺甲𫫇唑[n(%)] | 92 (5.08) | 13 (5.78) | 0.20 | 0.655 | |
| 第1代头孢菌素[n(%)] | 6(0.33) | 0(0) | 0.748 | 0.387 | |
| 第2代头孢菌素[n(%)] | 195 (10.77) | 20(8.89) | 0.748 | 0.387 | |
| 第3代头孢菌素[n(%)] | 1 150(63.50) | 106(47.11) | 22.75 | <0.001 | |
| 第4代头孢菌素[n(%)] | 40(2.21) | 14(6.22) | 12.49 | <0.001 | |
| 替加环素[n(%)] | 135 (7.45) | 15 (6.67) | 0.18 | 0.670 | |
| 预后 | |||||
| 住院时长 (d) | 23.00 (15.00, 37.00) | 39.00 (23.00, 66.00) | -8.88 | <0.001 | |
| 住院费用(元) | 73 009.11 (41 605.92, 147 581.23) | 127 163.58 (74 607.01, 262 362.70) | -8.24 | <0.001 | |
| 死亡[n(%)] | 265 (14.63) | 41 (18.22) | 2.02 | 0.155 |
表2
CDP对住院天数影响的多重线性回归分析
| 变量 | 未标准化系数 | 标准化系数 | t | P | B的95%CI | 共线性统计 | ||||
|---|---|---|---|---|---|---|---|---|---|---|
| B | SE | β | 下限 | 上限 | 容差 | VIF | ||||
| 回归方程截距 | 26.570 | 2.639 | 10.069 | 0.000 | 21.395 | 31.745 | ||||
| 年龄 | -0.051 | 0.037 | -0.032 | -1.396 | 0.163 | -0.123 | 0.021 | 0.896 | 1.116 | |
| CDP | 18.734 | 2.066 | 0.196 | 9.069 | 0.000 | 14.683 | 22.785 | 0.998 | 1.003 | |
| 冠心病 | 6.396 | 2.603 | 0.055 | 2.457 | 0.014 | 1.290 | 11.501 | 0.933 | 1.072 | |
| 白细胞计数 | 0.305 | 0.108 | 0.062 | 2.822 | 0.005 | 0.093 | 0.517 | 0.973 | 1.027 | |
| C反应蛋白 | 0.028 | 0.006 | 0.101 | 4.525 | 0.000 | 0.016 | 0.040 | 0.931 | 1.075 | |
| R2 | 0.058 | |||||||||
| 调整后 R2 | 0.056 | |||||||||
| F | F(5,2 030)=25.115, P<0.001 | |||||||||
表3
CDP对住院费用影响的多重线性回归分析
| 变量 | 未标准化系数 | 标准化系数 | t | P | B的95%CI | 共线性统计 | |||
|---|---|---|---|---|---|---|---|---|---|
| B | SE | β | 下限 | 上限 | 容差 | VIF | |||
| 回归方程截距 | 59 006.872 | 22 748.351 | 2.594 | 0.010 | 14 394.192 | 103 619.552 | |||
| APACHE Ⅱ | 3 994.021 | 577.936 | 0.164 | 6.911 | 0.000 | 2 860.608 | 5 127.434 | 0.807 | 1.239 |
| CDP | 68 854.912 | 11 358.579 | 0.130 | 6.062 | 0.000 | 46 579.159 | 91 130.665 | 0.994 | 1.006 |
| 急性胰腺炎 | -26 425.580 | 13 032.176 | -0.045 | -2.028 | 0.043 | -51 983.489 | -867.671 | 0.935 | 1.069 |
| 白细胞计数 | 722.038 | 601.734 | 0.026 | 1.200 | 0.230 | -458.047 | 1 902.123 | 0.948 | 1.055 |
| C反应蛋白 | 157.321 | 33.133 | 0.103 | 4.748 | 0.000 | 92.342 | 222.299 | 0.968 | 1.033 |
| 肌酐 | 78.469 | 21.622 | 0.082 | 3.629 | 0.000 | 36.066 | 120.872 | 0.883 | 1.133 |
| 白蛋白 | -497.693 | 625.675 | -0.018 | -0.795 | 0.426 | -1 724.728 | 729.343 | 0.900 | 1.111 |
| R2 | 0.080 | ||||||||
| 调整后 R2 | 0.077 | ||||||||
| F | F(7,2 028)=25.211, P<0.001 | ||||||||
表4
CDP危险因素的多因素回归分析
| 变量 | 变量水平 | β | 多因素回归分析OR(95% CI) | P |
|---|---|---|---|---|
| 性别 | 女性 | -0.500 | 0.60 (0.44 ~ 0.83) | 0.002 |
| 男性 | 对照 | |||
| 血流感染 | 阳性 | 0.570 | 1.77 (1.17 ~ 2.66) | 0.007 |
| 阴性 | 对照 | |||
| 胆道感染 | 阳性 | 0.580 | 1.79 (1.03 ~ 3.10) | 0.039 |
| 阴性 | 对照 | |||
| 碳青霉烯 | 使用 | 0.460 | 1.58 (1.16 ~ 2.15) | 0.003 |
| 未使用 | 对照 | |||
| 甲硝唑静脉注射 | 使用 | -0.540 | 0.58 (0.40 ~ 0.84) | 0.004 |
| 未使用 | 对照 | |||
| 头孢菌素 | 使用 | -0.620 | 0.54 (0.39 ~ 0.74) | <.001 |
| 未使用 | 对照 |
| [7] | Karanika S, Paudel S, Zervou FN, et al. Prevalence and clinical outcomes of Clostridium difficile infection in the intensive care unit[J]. Open Forum Infect Dis, 2015, 3(1):ofv186. |
| [8] | Loo VG, Poirier L, Miller MA, et al. A predominantly clonal multi-institutional outbreak of Clostridium difficile-associated diarrhea with high morbidity and mortality[J]. N Engl J Med, 2005, 353(23):2442-2449. |
| [9] | Zahar JR, Schwebel C, Adrie C, et al. Outcome of ICU patients with Clostridium difficile infection[J]. Crit Care, 2012, 16(6):R215. |
| [10] |
Worley J, Delaney ML, Cummins CK, et al. Genomic determination of relative risks for Clostridioides difficile infection from asymptomatic carriage in Intensive Care Unit patients[J]. Clin Infect Dis, 2021, 73(7):e1727-e1736.
doi: 10.1093/cid/ciaa894 pmid: 32676661 |
| [11] |
Longtin Y, Paquet-Bolduc B, Gilca R, et al. Effect of detecting and isolating Clostridium difficile carriers at hospital admission on the incidence of C difficile infections[J]. JAMA Intern Med, 2016, 176(6):796-804.
doi: 10.1001/jamainternmed.2016.0177 pmid: 27111806 |
| [12] | Peterson LR, O’Grady S, Keegan M, et al. Reduced Clostridioides difficile infection in a pragmatic stepped-wedge initiative using admission surveillance to detect colonization[J]. PLoS One, 2020, 15(3):e0230475. |
| [13] | Rao K, Malani PN. Diagnosis and treatment of Clostridioides (Clostridium) difficile infection in adults in 2020[J]. JAMA, 2020, 323(14):1403-1404. |
| [14] | Ang CW, Heyes G, Morrison P, et al. The acquisition and outcome of ICU-acquired Clostridium difficile infection in a single centre in the UK[J]. J Infect, 2008, 57(6):435-440. |
| [15] | Wang P, Zhou Y, Wang Z, et al. Identification of Clostridium difficile ribotype 027 for the first time in Mainland China[J]. Infect Control Hosp Epidemiol, 2014, 35(1):95-98. |
| [16] |
Zhou Y, Mao L, Yu J, et al. Epidemiology of Clostridium difficile infection in hospitalized adults and the first isolation of C. difficile PCR ribotype 027 in central China[J]. BMC Infect Dis, 2019, 19(1):232.
doi: 10.1186/s12879-019-3841-6 pmid: 30845918 |
| [17] |
Trubiano JA, Cheng AC, Korman TM, et al. Australasian Society Of Infectious Diseases updated guidelines for the management of Clostridium difficile infection in adults and children in Australia and New Zealand[J]. Intern Med J, 2016, 46(4):479-493.
doi: 10.1111/imj.13027 pmid: 27062204 |
| [18] | 中华医学会外科学分会, 中国研究型医院学会感染性疾病循证与转化专业委员会. 中国艰难梭菌感染诊治及预防指南(2024)[J]. 中华外科杂志, 202, 62(10):893-908. |
| [19] | Lawrence SJ, Puzniak LA, Shadel BN, et al. Clostridium difficile in the intensive care unit: epidemiology, costs, and colonization pressure[J]. Infect Control Hosp Epidemiol, 2007, 28(2):123-130. |
| [20] |
Martin SS, Aday AW, Almarzooq ZI, et al. 2024 heart disease and stroke statistics: a report of US and global data from the American Heart Association[J]. Circulation, 2024, 149(8):e347-e913.
doi: 10.1161/CIR.0000000000001209 pmid: 38264914 |
| [21] |
Le Monnier A, Duburcq A, Zahar JR, et al. Hospital cost of Clostridium difficile infection including the contribution of recurrences in French acute-care hospitals[J]. J Hosp Infect, 2015, 91(2):117-122.
doi: 10.1016/j.jhin.2015.06.017 pmid: 26253518 |
| [22] | Zhang S, Palazuelos-Munoz S, Balsells EM, et al. Cost of hospital management of Clostridium difficile infection in United States-a meta-analysis and modelling study[J]. BMC Infect Dis, 2016, 16(1):447. |
| [23] |
Jones AM, Kuijper EJ, Wilcox MH. Clostridium difficile: a European perspective[J]. J Infect, 2013, 66(2):115-128.
doi: 10.1016/j.jinf.2012.10.019 pmid: 23103666 |
| [24] |
Kahraman F, Yılmaz AS, Demir M, et al. APACHE Ⅱ score predicts in-hospital mortality more accurately than inflammatory indices in patients with acute coronary syndrome[J]. Kardiologiia, 2022, 62(9):54-59.
doi: 10.18087/cardio.2022.9.n1979 pmid: 36206138 |
| [25] | Mouliou DS. C-reactive protein: pathophysiology, diagnosis, false test results and a novel diagnostic algorithm for clinicians[J]. Diseases, 2023, 11(4):132. |
| [26] |
Morrison DJ, Preston T. Formation of short chain fatty acids by the gut microbiota and their impact on human metabolism[J]. Gut Microbes, 2016, 7(3):189-200.
doi: 10.1080/19490976.2015.1134082 pmid: 26963409 |
| [27] | Buffie CG, Bucci V, Stein RR, et al. Precision microbiome reconstitution restores bile acid mediated resistance to Clostridium difficile[J]. Nature, 2015, 517(7533):205-208. |
| [28] | Maffei S, Forini F, Canale P, et al. Gut microbiota and sex hormones: crosstalking players in cardiometabolic and cardiovascular disease[J]. Int J Mol Sci, 2022, 23(13):7154. |
| [1] | Quan M, Zhang X, Fang Q, et al. Fighting against Clostridioides difficile infection: current medications[J]. Int J Antimicrob Agents, 2024, 64(1):107198. |
| [2] | Salvati F, Catania F, Murri R, et al. Clostridioides difficile infection: an update[J]. Infez Med, 2024, 32(3):280-291. |
| [3] | Prechter F, Katzer K, Bauer M, et al. Sleeping with the enemy: Clostridium difficile infection in the intensive care unit[J]. Crit Care, 2017, 21(1):260. |
| [4] | Lee CC, Chiu CW, Lee JC, et al. Risk factors and clinical impact of carbapenem-resistant enterobacterales coinfections among hospitalized patients with Clostridioides difficile infection[J]. Infect Drug Resist, 2022,15:6287-6295. |
| [5] | Dubberke ER, Olsen MA. Burden of Clostridium difficile on the healthcare system[J]. Clin Infect Dis, 2012,55 Suppl 2:S88-S92. |
| [6] | Lessa FC, Winston LG, McDonald LC, et al. Burden of Clostridium difficile infection in the United States[J]. N Engl J Med, 2015, 372(24):2369-2370. |
| [29] | Miller MA, Louie T, Mullane K, et al. Derivation and validation of a simple clinical bedside score (ATLAS) for Clostridium difficile infection which predicts response to therapy[J]. BMC Infect Dis, 2013,13:148. |
| [30] | Brown KA, Khanafer N, Daneman N, et al. Meta-analysis of antibiotics and the risk of community-associated Clostridium difficile infection[J]. Antimicrob Agents Chemother, 2013, 57(5):2326-2332. |
| [31] | McDonald LC, Gerding DN, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults and children: 2017 update by the Infectious Diseases Society of America (IDSA) and Society for Healthcare Epidemiology of America (SHEA)[J]. Clin Infect Dis, 2018, 66(7):e1-e48. |
| [32] |
Slimings C, Riley TV. Antibiotics and hospital-acquired Clostridium difficile infection: update of systematic review and meta-analysis[J]. J Antimicrob Chemother, 2014, 69(4):881-891.
doi: 10.1093/jac/dkt477 pmid: 24324224 |
| [33] | Wren CM, Cowper J, Greer N, et al. Effect of reduced fluoroquinolone use on cephalosporin use, susceptibilities and Clostridioides difficile infections[J]. Antibiotics (Basel), 2022, 11(10):1312. |
| [1] | 张祎博, 吴文娟, 毕宇芳, 景峰, 顾志冬, 杨之涛, 尚寒冰, 林靖生, 陈尔真. 大型方舱医院感染预防与控制体系的建设和实践探索[J]. 诊断学理论与实践, 2022, 21(02): 165-168. |
| [2] | 王亦晨, 周剑平, 杨振华, 王敏慧, 刘佳, 倪语星, 张祎博, 石大可, 徐玉敏. 新型冠状病毒肺炎救治临时定点医院工作人员医院感染防控管理方案[J]. 诊断学理论与实践, 2022, 21(02): 270-272. |
| [3] | 庄蕾, 高卫益. 新型冠状病毒肺炎疫情期间非定点医疗机构“分区管理”策略[J]. 诊断学理论与实践, 2022, 21(02): 245-247. |
| [4] | 陈嘉仪, 周增丁, 曹伟伟, 赵小婕, 梁晓虹, 王正廷, 项晓刚, 郭颖. 新型冠状病毒肺炎疫情下普通医院转定点医院闭环工作人员管理防控经验[J]. 内科理论与实践, 2022, 17(02): 159-163. |
| [5] | 李丽, 朱咏臻, 周敏, 钱嘉, 方丽莉. 2017年至2021年上海嘉定区某医院多重耐药菌分析[J]. 诊断学理论与实践, 2022, 21(01): 62-67. |
| [6] | 吴浩, 房华, 汪瑞忠, 瞿静华, 沈孝峰, 陈华萍, 顾文超. 抗菌药物管理协作干预改进抗菌药物使用前微生物标本送检[J]. 诊断学理论与实践, 2019, 18(1): 93-97. |
| [7] | 李梅玲, 李磊, 张如愿, 刘嘉琳, 瞿洪平. 微量元素补充对术后脓毒症病人炎症反应的影响[J]. 外科理论与实践, 2018, 23(06): 533-538. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||