外科理论与实践 ›› 2020, Vol. 25 ›› Issue (04): 315-321.doi: 10.16139/j.1007-9610.2020.04.010
郭恩伟, 任大力, 章冰玉, 杨峰, 姚峪岚, 贾凌, 余琳, 冯刚( )
)
收稿日期:2020-01-07
出版日期:2020-07-25
发布日期:2022-07-18
通讯作者:
冯刚
E-mail:92102fg@sina.com
基金资助:
GUO Enwei, REN Dali, ZHANG Bingyu, YANG feng, YAO Yulan, JIA Ling, YU Lin, FENG Gang()
Received:2020-01-07
Online:2020-07-25
Published:2022-07-18
Contact:
FENG Gang
E-mail:92102fg@sina.com
摘要:
目的:研究创伤病人血清游离线粒体DNA(cell-free mitochondrial DNA, cf-mtDNA)含量变化及其与炎症反应的关系,探讨其临床价值。方法:创伤病人37例为创伤组,根据损伤程度分为多发伤组和单发伤组,及休克组和无休克组。10名健康志愿者为对照组。分别比较创伤组和对照组及创伤各亚组创伤后4 h、24 h、72 h和7 d时间点血清cf-mtDNA、 C反应蛋白(C-reactive protein, CRP)、 肿瘤坏死因子α(tumor necrosis factor-α,TNF-α)、白细胞介素6(interleukin-6,IL-6)含量差异,分析血清cf-mtDNA含量与损伤严重程度评分(injury severity score, ISS)、全身炎症反应综合征(systemic inflammatory response syndrome, SIRS)评分和血清CRP、TNF-α、IL-6含量的相关性。应用受试者工作特征(receiver operating characteristic, ROC)曲线评估创伤后血清cf-mtDNA含量诊断炎症反应的价值。结果:创伤病人伤后24 h、72 h血清cf-mtDNA含量明显高于对照组(均P<0.05)。多发伤组病人伤后4 h、24 h、72 h、7 d血清cf-mtDNA含量均明显高于单发伤组(分别P<0.05,P<0.01,P<0.01,P<0.05)。休克组病人伤后24 h血清cf-mtDNA含量明显高于无休克组病人(P<0.01)。创伤并发器官功能损伤组病人伤后4 h、24 h血清cf-mtDNA相对含量明显高于无并发器官功能损伤组(均P<0.05)。死亡病人血清cf-mtDNA含量峰值虽高于生存组,但差异无统计学意义(P>0.05)。随着创伤后血清cf-mtDNA含量升高的同时,血清TNF-α、IL-6、CRP含量也显著升高。创伤后24 h血清cf-mtDNA含量与ISS成正相关(r=0.454,P=0.004)。创伤后4 h~7 d血清cf-mtDNA含量分别与 SIRS评分、血清IL-6含量成正相关(分别r=0.458,P=0.000 1;r=0.252,P=0.005),但与血清TNF-α含量不相关(r=-0.058,P=0.511)。创伤后4~24 h血清cf-mtDNA含量与血清CRP含量成正相关(r=0.264,P=0.028)。创伤后4 h~7 d血清cf-mtDNA含量诊断炎症反应ROC曲线下面积为0.752(P=0.000 01),95%CI:0.668~0.836。根据最大约登指数计算结果,最佳临界值为0.075 3,其诊断炎症反应的灵敏度为63.6%,特异度为85.5%。结论:创伤病人创伤后早期血清cf-mtDNA含量升高,高血清cf-mtDNA含量表明创伤和炎症反应程度重。创伤后早期血清cf-mtDNA含量对炎症反应的诊断具有一定价值。
中图分类号:
郭恩伟, 任大力, 章冰玉, 杨峰, 姚峪岚, 贾凌, 余琳, 冯刚. 创伤病人血清游离线粒体含量变化及其临床意义[J]. 外科理论与实践, 2020, 25(04): 315-321.
GUO Enwei, REN Dali, ZHANG Bingyu, YANG feng, YAO Yulan, JIA Ling, YU Lin, FENG Gang. Change in amount of serum cell-free mitochondrial DNA and clinical relevance in trauma patients[J]. Journal of Surgery Concepts & Practice, 2020, 25(04): 315-321.
表1
创伤病人不同时间血清cf-mtDNA含量M(QL,QU)与对照组比较
| 组别 | 例数 | 4 h | 24 h | 72 h | 7 d |
|---|---|---|---|---|---|
| 创伤组 | 37 | 0.028(0.016,0.076) | 0.100(0.028,0.262)※△ | 0.043(0.018,0.119)※ | 0.039(0.018,0.103) |
| 对照组 | 10 | 0.011(0.008,0.506) | 0.011(0.008,0.506) | 0.011(0.008,0.506) | 0.011(0.008,0.506) |
表2
多发伤组与单发伤组病人不同时间血清cf-mtDNA含量M(QL,QU)比较
| 组别 | 例数 | ISS(分) | 4 h | 24 h | 72 h | 7 d |
|---|---|---|---|---|---|---|
| 单发伤组 | 17 | 18(16,25) | 0.018(0.014,0.034) | 0.018(0.014,0.034)△△ | 0.018(0.012,0.034) | 0.02(0.008,0.057) |
| 18~39岁 | 3 | 9(9,16) | 0.018(0.007,0.019) | 0.028(0.009,0.141) | 0.016(0.006,0.018) | 0.016(0.003,0.019) |
| 40~59岁 | 8 | 25(16,27) | 0.020(0.016,0.039) | 0.042(0.023,0.094) | 0.020(0.012,0.065) | 0.052(0.018,0.172) |
| ≥60岁 | 6 | 18(16,18) | 0.020(0.010,0.030) | 0.047(0.021,0.148) | 0.034(0.008,0.050) | 0.016(0.006,0.049) |
| 多发伤组 | 20 | 28(26,36) | 0.051(0.017,0.123)★ | 0.209(0.069,0.486)△△★★ | 0.092(0.042,0.160)★★ | 0.051(0.025,0.192)★ |
| 18~39岁 | 6 | 37(30,39) | 0.129(0.088,0.265) | 0.386(0.236,0.825)△★ | 0.133(0.045,0.222)★ | 0.219(0.018,0.898) |
| 40~59岁 | 8 | 27(26,37) | 0.056(0.030,0.123) | 0.242(0.079,0.505)★ | 0.116(0.042,0.165)★ | 0.056(0.025,0.139) |
| ≥60岁 | 6 | 27(21,31) | 0.017(0.015,0.046) | 0.065(0.063,0.138)△ | 0.066(0.025,0.133) | 0.043(0.024,0.082) |
表3
无休克创伤组与创伤性休克组病人伤后4 h~7 d血清cf-mtDNA含量M(QL,QU)比较
| 组别 | 例数 | ISS(分) | 4 h | 24 h | 72 h | 7 d |
|---|---|---|---|---|---|---|
| 创伤性休克组 | 15 | 29(25,36) | 0.040(0.016,0.135) | 0.255(0.079,0.493)★★△△ | 0.043(0.018,0.122) | 0.090(0.018,0.174) |
| 无休克创伤组 | 22 | 23.5(17.8,27) | 0.024(0.016,0.056) | 0.064(0.023,0.137)△ | 0.041(0.020,0.067) | 0.027(0.019,0.082) |
表4
创伤无并发器官功能损伤组与创伤并发器官功能损伤组病人伤后4 h~7 d血清cf-mtDNA含量M(QL,QU)比较
| 组别 | 例数 | ISS(分) | 4 h | 24 h | 72 h | 7 d |
|---|---|---|---|---|---|---|
| 器官功能衰竭组 | 13 | 29(25.5,37) | 0.074(0.035,0.132)★ | 0.242(0.073,0.389)★△ | 0.048(0.028,0.108) | 0.086(0.020,0.200) |
| 无器官功能衰竭组 | 24 | 27(17.3,27) | 0.017(0.014,0.047) | 0.066(0.023,0.140)△△ | 0.034(0.013,0.066) | 0.025(0.012,0.075) |
表5
多发伤与单发伤病人伤后4 h至7 d血清TNF-α含量($\bar{x}$)(ng/L)比较
| 组别 | 例数 | ISS(分)M(QL,QU) | 4 h | 24 h | 72 h | 7 d |
|---|---|---|---|---|---|---|
| 单发伤组 | 17 | 18(16,25) | 7.41 ± 4.31 | 10.67 ± 6.41※ | 7.26 ± 4.11 | 9.37 ± 7.34 |
| 多发伤组 | 20 | 28(26,36) | 10.83 ± 5.45※※ | 17.22 ± 9.27△△★★※※ | 13.74 ± 5.00★★※※ | 12.37 ± 7.73※ |
| 对照组 | 10 | 0(0,0) | 4.67 ± 0.47 | 4.67 ± 0.47 | 4.67 ± 0.47 | 4.67 ± 0.47 |
表6
多发伤与单发伤病人伤后4 h~7 d血清IL-6含量($\bar{x}$)(ng/L)比较
| 组别 | 例数 | ISS(分)M(QL,QU) | 4 h | 24 h | 72 h | 7 d |
|---|---|---|---|---|---|---|
| 单发伤组 | 17 | 18(16,25) | 72.74 ± 46.96※ | 86.38 ± 51.21※ | 55.23 ± 74.58 | 39.43 ± 40.16 |
| 多发伤组 | 20 | 28(26,36) | 95.07 ± 82.3※ | 162.64 ± 165.19△★★※※ | 59.97 ± 71.55 | 53.59 ± 62.28 |
| 对照组 | 10 | 0(0,0) | 6.62 ± 2.31 | 6.62 ± 2.31 | 6.62 ± 2.31 | 6.62 ± 2.31 |
表7
多发伤与单发伤病人伤后4 h~7 d血清CRP含量($\bar{x}$)(mg/L)比较
| 组别 | 例数 | ISS(分)M(QL,QU) | 4 h | 24 h | 72 h | 7 d |
|---|---|---|---|---|---|---|
| 单发伤组 | 17 | 18(16,25) | 11.79 ± 10.12 | 105.18 ± 64.76△△※※ | 112.51 ± 67.34△△※※ | 95.42 ± 72.28△△※※ |
| 多发伤组 | 20 | 28(26,36) | 16.04 ± 14.77 | 117.01 ± 57.27△△※※ | 156.88 ± 43.83△△★※※ | 103.01 ± 65.06△△※※ |
| 对照组 | 10 | 0(0,0) | 4.46 ± 2.75 | 4.46 ± 2.75 | 4.46 ± 2.75 | 4.46 ± 2.75 |
表8
多发伤与单发伤病人伤后4 h~7 d SIRS评分($\bar{x}$)(分)比较
| 组别 | 例数 | ISS(分)M(QL,QU) | 4 h | 24 h | 72 h | 7 d |
|---|---|---|---|---|---|---|
| 单发伤组 | 17 | 18(16,25) | 1.47 ± 1.01※※ | 1.82 ± 1.19※※ | 1.53 ± 0.80※※ | 1.53 ± 1.23※※ |
| 多发伤组 | 20 | 28(26,36) | 2.10 ± 0.85★※※ | 2.55 ± 0.76★※※ | 2.05 ± 0.71※※ | 1.85 ± 0.93※※ |
| 对照组 | 10 | 0(0,0) | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 ± 0.00 | 0.00 ± 0.00 |
表9
死亡组与生存组血清cf-mtDNA相对含量峰值M(QL,QU)比较
| 组别 | 例数 | 血浆cf-mtDNA相对含量峰值 |
|---|---|---|
| 死亡组 | 5 | 0.203(0.079,0.485) |
| 生存组 | 32 | 0.138(0.064,0.289) |
| P值 | 0.519 |
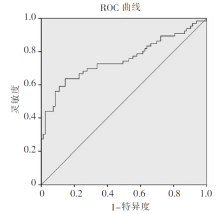
图1
创伤后4 h~7 d血清cf-mtDNA相对含量诊断炎症反应ROC曲线

| [1] |
Soreide K. Epidemiology of major trauma[J]. Br J Surg, 2009, 96(7):697-698.
doi: 10.1002/bjs.6643 URL |
| [2] |
Zhang Q, Raoof M, Chen Y, et al. Circulating mitochondrial DAMPs cause inflammatory responses to injury[J]. Nature, 2010, 464(7285):104-107.
doi: 10.1038/nature08780 URL |
| [3] |
Lam NY, Rainer TH, Chiu RW, et al. Plasma mitochondrial DNA concentrations after trauma[J]. Clin Chem, 2004, 50(1):213-216.
doi: 10.1373/clinchem.2003.025783 URL |
| [4] |
Thurairajah K, Briggs GD, Balogh ZJ. The source of cell-free mitochondrial DNA in trauma and potential therapeutic strategies[J]. Eur J Trauma Emerg Surg, 2018, 44(3):325-334.
doi: 10.1007/s00068-018-0954-3 URL |
| [5] |
McIlroy DJ, Bigland M, White AE, et al. Cell necrosis-independent sustained mitochondrial and nuclear DNA release following trauma surgery[J]. J Trauma Acute Care Surg, 2015, 78(2):282-288.
doi: 10.1097/TA.0000000000000519 pmid: 25602756 |
| [6] |
Yamanouchi S, Kudo D, Yamada M, et al. Plasma mitochondrial DNA levels in patients with trauma and severe sepsis: Time course and the association with clinical status[J]. J Crit Care, 2013, 28(6):1027-1031.
doi: 10.1016/j.jcrc.2013.05.006 pmid: 23787023 |
| [7] |
Hu Q, Zhou Q, Wu J, et al. The role of mitochondrial DNA in the development of ischemia reperfusion injury[J]. Shock, 2019, 51(1):52-59.
doi: 10.1097/SHK.0000000000001190 URL |
| [8] |
Gu X, Yao Y, Wu G, et al. The plasma mitochondrial DNA is an independent predictor for post-traumatic systemic inflammatory response syndrome[J]. PLoS One, 2013, 8(8):e72834.
doi: 10.1371/journal.pone.0072834 URL |
| [9] |
Wang HC, Lin YJ, Tsai NW, et al. Serial plasma deo-xyribonucleic acid levels as predictors of outcome in acute traumatic brain injury[J]. J Neurotrauma, 2014, 31(11):1039-1045.
doi: 10.1089/neu.2013.3070 URL |
| [10] | Zhang J, Chen X, Liu Z, et al. Association between plasma mitochondrial DNA and sterile systemic inflammatory response syndrome in patients with acute blunt traumatic injury[J]. Int J Clin Exp Med, 2017, 10:3254-3262. |
| [11] |
Gu X, Wu G, Yao Y, et al. Intratracheal administration of mitochondrial DNA directly provokes lung inflammation through the TLR9-p38 MAPK pathway[J]. Free Radic Biol Med, 2015, 83:149-158.
doi: 10.1016/j.freeradbiomed.2015.02.034 URL |
| [12] |
Xie L, Liu S, Cheng J, et al. Exogenous administration of mitochondrial DNA promotes ischemia reperfusion injury via TLR9-p38 MAPK pathway[J]. Regul Toxicol Pharmacol, 2017, 89:148-154.
doi: 10.1016/j.yrtph.2017.07.028 URL |
| [13] |
West AP, Koblansky AA, Ghosh S. Recognition and signaling by toll-like receptors[J]. Annu Rev Cell Dev Biol, 2006, 22:409-437.
doi: 10.1146/annurev.cellbio.21.122303.115827 URL |
| [14] |
Zhang Q, Itagaki K, Hauser CJ. Mitochondrial DNA is released by shock and activates neutrophils via P38 map kinase[J]. Shock, 2010, 34(1):55-59.
doi: 10.1097/SHK.0b013e3181cd8c08 pmid: 19997055 |
| [15] |
Zhang JZ, Liu Z, Liu J, et al. Mitochondrial DNA induces inflammation and increases TLR9/NF-κB expression in lung tissue[J]. Int J Mol Med, 2014, 33(4):817-824.
doi: 10.3892/ijmm.2014.1650 URL |
| [16] |
Timmermans K, Kox M, Scheffer GJ, et al. Plasma nuc-lear and mitochondrial DNA levels, and markers of inflammation, shock, and organ damage in patients with septic shock[J]. Shock, 2016, 45(6):607-612.
doi: 10.1097/SHK.0000000000000549 pmid: 26717107 |
| [17] | Qin C, Gu J, Liu R, et al. Release of mitochondrial DNA correlates with peak inflammatory cytokines in patients with acute myocardial infarction[J]. Anatol J Cardiol, 2017, 17(3):224-228. |
| [18] |
Simmons JD, Lee YL, Mulekar S, et al. Elevated levels of plasma mitochondrial DNA DAMPs are linked to clinical outcome in severely injured human subjects[J]. Ann Surg, 2013, 258(4):591-598.
doi: 10.1097/SLA.0b013e3182a4ea46 pmid: 23979273 |
| [19] |
Aswani A, Manson J, Itagaki K, et al. Scavenging circulating mitochondrial DNA as a potential therapeutic option for multiple organ dysfunction in trauma hemorrhage[J]. Front Immunol, 2018, 9:891.
doi: 10.3389/fimmu.2018.00891 URL |
| [20] |
Faust HE, Reilly JP, Anderson BJ, et al. Plasma mitochondrial DNA levels are associated with ARDS in trauma and sepsis patients[J]. Chest, 2020, 157(1):67-76.
doi: 10.1016/j.chest.2019.09.028 URL |
| [21] |
McIlroy DJ, Minahan K, Keely S, et al. Reduced deo-xyribonuclease enzyme activity in response to high postinjury mitochondrial DNA concentration provides a therapeutic target for systemic inflammatory response syndrome[J]. J Trauma Acute Care Surg, 2018, 85(2):354-358.
doi: 10.1097/TA.0000000000001919 pmid: 30080781 |
| [1] | 蔡飞宇 程二林 艾合买提江·玉素甫. 拱顶石穿支皮瓣修复手、足部软组织缺损[J]. 组织工程与重建外科杂志, 2022, 18(4): 311-. |
| [2] | 董继英 吴珊 王棽 严敏 米晶 林琥燕 曾颖 张逸秋 宋晨璐 裴庆 朱婕 温晓钰 陆文婷 姚敏. 光电治疗对皮肤创伤性瘢痕的疗效研究[J]. 组织工程与重建外科杂志, 2022, 18(2): 133-. |
| [3] | 李长生 李事成. 后路手术治疗急诊创伤性腰椎滑脱症的临床效果分析[J]. 组织工程与重建外科杂志, 2021, 17(6): 553-. |
| [4] | 沐阳, 陈欣. 血浆降钙素原和C反应蛋白对多发伤病人预后评估的价值[J]. 外科理论与实践, 2021, 26(6): 532-536. |
| [5] | 高嘉蔓 徐梁 姜陶然 俞哲元 曹德君. 肋硬骨-软骨联合隆鼻修复创伤后鼻畸形[J]. 组织工程与重建外科杂志, 2021, 17(3): 227-. |
| [6] | 郭静, 沈银忠. HIV感染/AIDS合并结核病的临床及免疫学特点研究进展[J]. 诊断学理论与实践, 2021, 20(04): 401-406. |
| [7] | 张立鹏, 王忠敏, 赵新建. 创伤性脾破裂行脾动脉介入栓塞与外科手术治疗的临床比较研究[J]. 外科理论与实践, 2020, 25(03): 222-226. |
| [8] | 王紫,孙婷也,陶筱婷,王昕,庄美婷,李海洲,李青峰. M2型巨噬细胞调控增生性瘢痕形成的权重基因共表达网络分析[J]. 组织工程与重建外科杂志, 2019, 15(3): 146-151. |
| [9] | 宋阿会,佟琰,刘英莉. BK通道抑制剂对人脐带华通胶来源的间充质干细胞的增殖、凋亡及细胞因子的影响[J]. 组织工程与重建外科杂志, 2019, 15(1): 5-9. |
| [10] | 张舒, 王露露, 孙璟, 江石湖. 降钙素原和C反应蛋白在急性胆源性胰腺炎中的诊断及预后价值比较[J]. 诊断学理论与实践, 2019, 18(06): 668-671. |
| [11] | 王媛媛, 范秋灵. 血清降钙素原在慢性肾脏病合并细菌感染患者中的临床价值[J]. 诊断学理论与实践, 2019, 18(03): 353-359. |
| [12] | 刘莉,刘宏超. 颈阔肌肌皮瓣在颌面部创伤修复中的应用[J]. 组织工程与重建外科杂志, 2018, 14(5): 272-274. |
| [13] | 周思政,李青峰. 皮肤创伤愈合和增生性瘢痕动物模型的研究进展[J]. 组织工程与重建外科杂志, 2018, 14(1): 48-52. |
| [14] | 王鸿珍, 徐文彬,. 原发性高血压患者乙醛脱氢酶2基因多态性与血清高敏C反应蛋白水平的关系[J]. 内科理论与实践, 2018, 13(06): 349-353. |
| [15] | 杜坤, 杨喜, 卞炳贤, 任懿倩, 张广慧. 血清presepsin(sCD14-ST)、降钙素原、C反应蛋白和白介细胞素-6诊断血流细菌感染的诊断性能比较[J]. 诊断学理论与实践, 2018, 17(05): 581-585. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||