诊断学理论与实践 ›› 2019, Vol. 18 ›› Issue (03): 353-359.doi: 10.16150/j.1671-2870.2019.03.021
王媛媛, 范秋灵( )
)
收稿日期:2018-11-01
出版日期:2019-06-25
发布日期:2019-06-25
通讯作者:
范秋灵
E-mail:cmufql@163.com
基金资助:
WANG Yuanyuan, FAN Qiuling()
Received:2018-11-01
Online:2019-06-25
Published:2019-06-25
Contact:
FAN Qiuling
E-mail:cmufql@163.com
摘要:
目的: 观察不同分期慢性肾脏病(chronic kidney disease,CKD)患者的血清降钙素原(procalcitonin,PCT)中位值,分析PCT在不同分期CKD合并细菌感染患者中的诊断最佳临界值。方法: 纳入我院肾内科住院治疗并完善PCT检测的354例CKD患者,包括合并细菌感染并予抗生素治疗的CKD患者153例,无感染症状的CKD患者201例。根据估算的肾小球滤过率(estimated glomerular filtration rate, eGFR)将所有患者分为G1期、G2期、G3期、G4期、G5期(非肾脏替代治疗)及中心静脉置管血液透析(haemodialysis, HD)组。采用Spearman相关分析评估PCT水平与血清肌酐、eGFR间的相关性。采用ROC曲线分析血清PCT诊断CKD不同分期合并细菌感染的最佳临界值,并用多因素逐步Logistic回归分析评估感染的影响因素。结果: CKD各分期感染组的血清PCT水平显著高于非感染组。PCT动态变化与临床感染恢复相平行。PCT水平与血清肌酐呈正相关(P<0.001),与eGFR呈负相关(P<0.001)。采用ROC曲线得到总CKD组及G3期、G4期、G5期(非肾脏替代治疗)、中心静脉置管HD组中,鉴别感染与非感染的血清PCT最佳临界值分别为0.40 ng/mL、0.12 ng/mL、0.23 ng/mL、0.28 ng/mL、0.60 ng/mL。多因素逐步Logistic回归分析显示,PCT、C反应蛋白、白细胞、血清白蛋白是感染的独立影响因素。结论: PCT可作为诊断CKD合并细菌感染的一个有用的临床指标,且根据肾功能分期不同,其诊断感染的阈值不同;检测PCT的动态变化对CKD患者感染的诊断和治疗监测有重要的诊断价值。
中图分类号:
王媛媛, 范秋灵. 血清降钙素原在慢性肾脏病合并细菌感染患者中的临床价值[J]. 诊断学理论与实践, 2019, 18(03): 353-359.
WANG Yuanyuan, FAN Qiuling. Clinical value of serum procalcitonin in patients of chronic kidney disease with bacterial infection[J]. Journal of Diagnostics Concepts & Practice, 2019, 18(03): 353-359.
表1
入组患者基线特征
| 特征 | 感染组 (n=134) | 非感染组 (n=201) | P值 |
|---|---|---|---|
| 年龄(岁) | 54 | 49 | 0.206 |
| 性别[n(%)] | |||
| 男 | 84(62.7%) | 111(55.2%) | 0.067 |
| 女 | 50(37.3%) | 90(44.8%) | |
| 住院天数(d) | 17 | 12 | <0.001 |
| 实验室参数 | |||
| 血清PCT(ng/mL) | 0.52 | 0.10 | <0.001 |
| CRP(mg/L) | 44.25 | 3.29 | <0.001 |
| 白细胞计数(×109/L) | 8.39 | 6.40 | <0.001 |
| 粒细胞与淋巴细胞比率 | 5.23 | 2.83 | <0.001 |
| 血红蛋白(g/L) | 101.59±28.65 | 105.67±31.23 | 0.232 |
| 血清肌酐(μmol/L) | 298.50 | 292 | 0.449 |
| eGFR[mL/(min·1.73 m2)] | 18.7 | 17.9 | 0.892 |
| 血尿素氮(mmol/L) | 17.88 | 16.08 | 0.104 |
| 血清胱抑素C(mg/L) | 4.20 | 3.41 | 0.006 |
| 血清总蛋白(g/L) | 54.70 | 59.55 | <0.001 |
| 血清白蛋白(g/L) | 27.70 | 35.30 | <0.001 |
| 血清前白蛋白(mg/dL) | 23.00 | 29.20 | <0.001 |
| 血清铁(μmol/L) | 8.71±5.48 | 12.24±6.61 | 0.127 |
| 铁蛋白(μg/L) | 428.70 | 204.90 | <0.001 |
表2
CKD不同分期的PCT水平
| 组别 | PCT(ng/mL) | ||
|---|---|---|---|
| 范围 | 均数 | 中位数 | |
| G1期 | |||
| 感染组 | 0.11~4.02 | 0.64 | 0.29 |
| 非感染组 | 0.02~0.24 | 0.04 | 0.04 |
| G2期 | |||
| 感染组 | 0.14~1.13 | 0.32 | 0.24 |
| 非感染组 | 0.02~0.16 | 0.06 | 0.06 |
| G3期 | |||
| 感染组 | 0.13~100.00 | 5.18 | 0.27 |
| 非感染组 | 0.02~0.19 | 0.07 | 0.06 |
| G4期 | |||
| 感染组 | 0.17~35.44 | 2.18 | 0.45 |
| 非感染组 | 0.02~0.35 | 0.11 | 0.10 |
| G5期 | |||
| 感染组 | 0.29~44.50 | 3.18 | 0.80 |
| 非感染组 | 0.05~0.45 | 0.18 | 0.16 |
| 中心静脉置管HD | |||
| 感染组 | 0.45~100.00 | 7.42 | 1.28 |
| 非感染组 | 0.10~0.77 | 0.32 | 0.29 |
表3
血清PCT水平与血清肌酐、eGFR相关性分析(Spearman相关)
| 分组 | 血清肌酐 | eGFR | ||
|---|---|---|---|---|
| r值 | P值 | r值 | P值 | |
| 感染组PCT | 0.565 | <0.001 | -0.561 | <0.001 |
| 非感染组PCT | 0.825 | <0.000 | -0.804 | <0.000 |
表4
血清CRP与血清肌酐、eGFR相关性分析(Spearman相关)
| 分组 | 血清肌酐 | eGFR | ||
|---|---|---|---|---|
| r | P | r | P | |
| 感染组PCT | 0.023 | <0.001 | -0.034 | <0.001 |
| 非感染组PCT | 0.126 | 0.076 | -0.127 | 0.072 |
表5
PCT、CRP对CKD各分期合并细菌感染诊断价值比较
| 组别 | 参数 | 最佳临界值 | 灵敏度(%) | 特异度(%) | AUC | 95%CI | P值 |
|---|---|---|---|---|---|---|---|
| 总CKD | PCT | 0.40 | 76.30 | 91.10 | 0.920 | 0.892~0.948 | <0.001 |
| CRP | 10.10 | 89.63 | 88.18 | 0.942 | 0.917~0.967 | <0.001 | |
| G3期 | PCT | 0.12 | 100 | 96.43 | 0.994 | 0.985~1.000 | <0.001 |
| CRP | 7.76 | 85.71 | 100 | 0.895 | 0.804~0.987 | <0.001 | |
| G4期 | PCT | 0.23 | 84.60 | 94.10 | 0.986 | 0.970~1.000 | <0.001 |
| CRP | 10.20 | 93.20 | 79.40 | 0.902 | 0.833~0.970 | <0.001 | |
| G5期 | PCT | 0.28 | 100 | 91.50 | 0.992 | 0.984~1.000 | <0.001 |
| CRP | 12.20 | 89.70 | 94.90 | 0.929 | 0.889~0.970 | <0.001 | |
| 中心静脉置管 | PCT | 0.60 | 93.10 | 91.70 | 0.985 | 0.966~1.000 | <0.001 |
| CRP | 9.85 | 93.10 | 80.60 | 0.903 | 0.839~0.967 | <0.001 |

图1
PCT、CRP、WBC、粒细胞和淋巴细胞比率诊断感染的预测能力(ROC曲线分析)
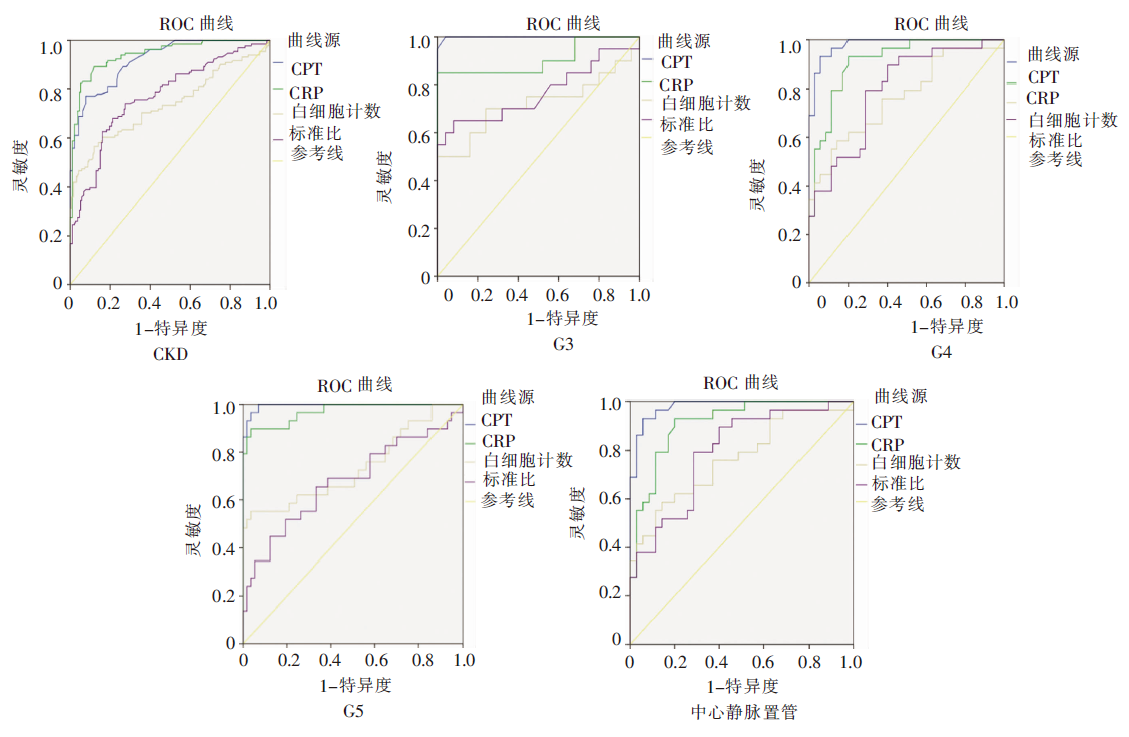
表6
CKD不同分期PCT、CRP、白细胞计数、粒细胞和淋巴细胞比的诊断价值比较(P值)
| 组别 | PCT比CRP | PCT比WBC | PCT比粒淋比 | CRP 比WBC | CRP比粒淋比 | WBC比粒淋比 |
|---|---|---|---|---|---|---|
| 总CKD | 0.216 | <0.001 | <0.001 | <0.001 | <0.001 | 0.276 |
| G3期 | 0.083 | 0.001 | 0.004 | 0.020 | 0.130 | 0.547 |
| G4期 | 0.268 | 0.002 | <0.001 | 0.007 | 0.006 | 0.665 |
| G5期 | 0.147 | 0.001 | <0.001 | <0.001 | <0.001 | 0.400 |
| 中心静脉置管HD | 0.057 | 0.001 | 0.001 | 0.013 | 0.029 | 0.620 |
表7
多因素逐步Logistic回归分析影响CKD患者感染的因素
| 因素 | B | S.E. | Wald | Exp(B) | 95%CI | P值 |
|---|---|---|---|---|---|---|
| PCT | 6.730 | 1.311 | 26.344 | 837.018 | 64.069~10935.141 | 0.000 |
| CRP | 0.108 | 0.023 | 22.077 | 1.114 | 1.065~1.166 | 0.000 |
| 白细胞计数 | 0.176 | 0.085 | 4.321 | 1.193 | 1.010~1.408 | 0.038 |
| 白蛋白 | -0.126 | 0.030 | 17.905 | 0.882 | 0.832~0.935 | 0.000 |
| [1] |
Cheikh Hassan HI, Tang M, Djurdjev O, et al. Infection in advanced chronic kidney disease leads to increased risk of cardiovascular events, end-stage kidney disease and mortality[J]. Kidney Int, 2016, 90(4):897-904.
doi: 10.1016/j.kint.2016.07.013 URL |
| [2] |
Ojeda R, Aljama PA. Chronic microinflammation and endothelial damage in uremia[J]. Nefrologia, 2008, 28(6):583-586.
pmid: 19016629 |
| [3] |
Wacker C, Prkno A, Brunkhorst FM, et al. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis[J]. Lancet Infect Dis, 2013, 13(5):426-435.
doi: 10.1016/S1473-3099(12)70323-7 URL |
| [4] |
de Jong E, van Oers JA, Beishuizen A, et al. Efficacy and safety of procalcitonin guidance in reducing the duration of antibiotic treatment in critically ill patients: a randomised, controlled, open-label trial[J]. Lancet Infect Dis, 2016, 16(7):819-827.
doi: 10.1016/S1473-3099(16)00053-0 URL |
| [5] |
Manzano S, Bailey B, Gervaix A, et al. Markers for bacterial infection in children with fever without source[J]. Arch Dis Child, 2011, 96(5):440-446.
doi: 10.1136/adc.2010.203760 pmid: 21278424 |
| [6] |
Grace E, Turner RM. Use of procalcitonin in patients with various degrees of chronic kidney disease including renal replacement therapy[J]. Clin Infect Dis, 2014, 59(12):1761-1767.
doi: 10.1093/cid/ciu732 URL |
| [7] |
Lavín-Gómez BA, Palomar-Fontanet R, Gago-Fraile M, et al. Inflammation markers, chronic kidney disease, and renal replacement therapy[J]. Adv Perit Dial, 2011, 27:33-37.
pmid: 22073825 |
| [8] | Meisner M, Lohs T, Huettemann E, et al. The plasma elimination rate and urinary secretion of procalcitonin in patients with normal and impaired renal function[J]. Eur J Anaesthesiol, 2001, 18(2):79-87. |
| [9] | 中华医学会呼吸病学分会. 社区获得性肺炎诊断和治疗指南[J]. 中华结核和呼吸杂志, 2006, 29(10):651-655. |
| [10] | 葛均波, 徐永健. 内科学[M]. 8版. 北京: 人民卫生出版社, 2008:41-45,496-502. |
| [11] | 中华医学会重症医学分会. 血管内导管相关感染的预防与治疗指南(2007)[J]. 中国实用外科杂志, 2008, 28(6):413-421. |
| [12] |
DeLong ER, DeLong DM, Clarke-Pearson DL. Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach[J]. Biometrics, 1988, 44(3):837-845.
pmid: 3203132 |
| [13] |
Pereira BJ, Shapiro L, King AJ, et al. Plasma levels of IL-1 beta, TNF alpha and their specific inhibitors in undialyzed chronic renal failure, CAPD and hemodialysis patients[J]. Kidney Int, 1994, 45(3):890-896.
pmid: 8196293 |
| [14] |
Dahaba AA, Rehak PH, List WF. Procalcitonin and C-reactive protein plasma concentrations in nonseptic uremic patients undergoing hemodialysis[J]. Intensive Care Med, 2003, 29(4):579-583.
doi: 10.1007/s00134-003-1664-8 URL |
| [15] |
Herget-Rosenthal S, Marggraf G, Pietruck F, et al. Procalcitonin for accurate detection of infection in haemodialysis[J]. Nephrol Dial Transplant, 2001, 16(5):975-979.
doi: 10.1093/ndt/16.5.975 URL |
| [16] |
Shikata K, Makino H. Microinflammation in the pathogenesis of diabetic nephropathy[J]. J Diabetes Investig, 2013, 4(2):142-149.
doi: 10.1111/jdi.12050 URL |
| [17] |
Tian J, Hou X, Hu L, et al. Efficacy comparison of atorvastatin versus rosuvastatin on blood lipid and microinflammatory state in maintenance hemodialysis patients[J]. Ren Fail, 2017, 39(1):153-158.
doi: 10.1080/0886022X.2016.1256309 URL |
| [18] |
Gupta J, Mitra N, Kanetsky PA, et al. Association between albuminuria, kidney function, and inflammatory biomarker profile in CKD in CRIC[J]. Clin J Am Soc Nephrol, 2012, 7(12):1938-1946.
doi: 10.2215/CJN.03500412 URL |
| [19] |
Pavkov ME, Nelson RG, Knowler WC, et al. Elevation of circulating TNF receptors 1 and 2 increases the risk of end-stage renal disease in American Indians with type 2 diabetes[J]. Kidney Int, 2015, 87(4):812-819.
doi: 10.1038/ki.2014.330 pmid: 25272234 |
| [20] | Tasic D, Radenkovic S, Kocic G, et al. Microinflammation factors in the common diseases of the heart and kidneys[J]. Dis Markers, 2015, 2015:470589. |
| [21] |
Akchurin OM, Kaskel F. Update on inflammation in chro-nic kidney disease[J]. Blood Purif, 2015, 39(1-3):84-92.
doi: 10.1159/000368940 URL |
| [22] |
Lee WS, Kang DW, Back JH, et al. Cutoff value of serum procalcitonin as a diagnostic biomarker of infection in end-stage renal disease patients[J]. Korean J Intern Med, 2015, 30(2):198-204.
doi: 10.3904/kjim.2015.30.2.198 URL |
| [23] |
Dumea R, Siriopol D, Hogas S, et al. Procalcitonin: diagnostic value in systemic infections in chronic kidney di-sease or renal transplant patients[J]. Int Urol Nephrol, 2014, 46(2):461-468.
doi: 10.1007/s11255-013-0542-8 URL |
| [24] | Meisner M, Lohs T, Huettemann E, et al. The plasma elimination rate and urinary secretion of procalcitonin in patients with normal and impaired renal function[J]. Eur J Anaesthesiol, 2001, 18(2):79-87. |
| [25] |
Nakamura Y, Murai A, Mizunuma M, et al. Potential use of procalcitonin as biomarker for bacterial sepsis in patients with or without acute kidney injury[J]. J Infect Chemother, 2015, 21(4):257-263.
doi: 10.1016/j.jiac.2014.12.001 URL |
| [26] |
Strassmann G, Fong M, Kenney JS, et al. Evidence for the involvement of interleukin 6 in experimental cancer cachexia[J]. J Clin Invest, 1992, 89(5):1681-1684.
doi: 10.1172/JCI115767 pmid: 1569207 |
| [27] | Zha Y, Qian Q. Protein Nutrition and Malnutrition in CKD and ESRD[J]. Nutrients, 2017, 9(3),pii: E208. |
| [28] |
Obialo CI, Okonofua EC, Nzerue MC, et al. Role of hypoalbuminemia and hypocholesterolemia as copredictors of mortality in acute renal failure[J]. Kidney Int, 1999, 56(3):1058-1063.
pmid: 10469374 |
| [29] |
Sridhar NR, Josyula S. Hypoalbuminemia in hemodialyzed end stage renal disease patients: risk factors and relationships--a 2 year single center study[J]. BMC Nephrol, 2013, 14:242.
doi: 10.1186/1471-2369-14-242 URL |
| [30] |
Allawi AAD. Malnutrition, inflamation and atherosclerosis (MIA syndrome) in patients with end stage renal disease on maintenance hemodialysis (a single centre experience[J]. Diabetes Metab Syndr, 2018, 12(2):91-97.
doi: 10.1016/j.dsx.2017.09.003 URL |
| [1] | 何亲羽, 王伟, 陈立芬, 张雪蕾, 董治亚. LHCGR基因突变致家族性男性性早熟2例报告及文献复习[J]. 诊断学理论与实践, 2022, 21(05): 598-605. |
| [2] | 陈志敏, 何浩岚. 艾滋病合并马尔尼菲篮状菌病的诊治现状[J]. 诊断学理论与实践, 2022, 21(04): 425-430. |
| [3] | 沈银忠. 《人类免疫缺陷病毒感染/艾滋病合并结核分枝杆菌感染诊治专家共识》解读[J]. 诊断学理论与实践, 2022, 21(04): 431-436. |
| [4] | 陈宏, 沈银忠. 人类免疫缺陷病毒感染/艾滋病合并结核病的诊治进展[J]. 诊断学理论与实践, 2022, 21(04): 530-534. |
| [5] | 何新, 陈慧, 冯炜炜. 机器学习算法在辅助超声诊断附件肿块良恶性中的应用研究进展[J]. 诊断学理论与实践, 2022, 21(04): 541-546. |
| [6] | 徐子真, 李擎天, 刘湘帆, 李莉, 李惠, 王也飞, 吴洁敏, 陈宁, 梁璆荔, 陈松立, 戴健敏, 宋珍, 丁磊. 实验诊断学在线课程的建立和实践[J]. 诊断学理论与实践, 2022, 21(04): 547-550. |
| [7] | 赵然, 詹维伟, 侯怡卿. 计算机辅助诊断系统辅助超声诊断甲状腺弥漫性病变合并结节良恶性的应用价值[J]. 诊断学理论与实践, 2022, 21(03): 390-394. |
| [8] | 郭业兵, 郑金峰. 阴道壁胃肠道外间质瘤一例报道并文献复习[J]. 诊断学理论与实践, 2022, 21(03): 405-407. |
| [9] | 王刚, 陈生弟. 神经病学的诊断:起源、发展及挑战[J]. 诊断学理论与实践, 2022, 21(01): 1-4. |
| [10] | 唐静仪, 余群, 刘军. 结合人工智能的结构影像分析对阿尔茨海默病的早期预测及精准诊断研究进展[J]. 诊断学理论与实践, 2022, 21(01): 12-17. |
| [11] | 魏文石. 直面我国阿尔茨海默病诊治的挑战——《中国阿尔茨海默病报告2021》解读[J]. 诊断学理论与实践, 2022, 21(01): 5-7. |
| [12] | 王蔚, 王小钦. 缺铁性贫血的病因诊断[J]. 诊断学理论与实践, 2021, 20(06): 529-532. |
| [13] | 岳婧婧, 宋琦, 江旭峰, 王黎, 赵维莅, 严福华. 磁共振全身扩散加权成像结合T2WI抑脂序列与FDG-PET/CT在初发淋巴瘤分期及病灶检出的对比研究[J]. 诊断学理论与实践, 2021, 20(06): 540-546. |
| [14] | 王昭晖, 吴海波. 胃神经鞘瘤31例临床病理学分析[J]. 诊断学理论与实践, 2021, 20(06): 552-556. |
| [15] | 王广宇, 杨昕, 张立娟, 谭姣容. 住院新诊断2型糖尿病男性患者血浆总睾酮水平与骨钙素的相关性研究[J]. 诊断学理论与实践, 2021, 20(06): 573-578. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||