外科理论与实践 ›› 2021, Vol. 26 ›› Issue (01): 66-71.doi: 10.16139/j.1007-9610.2021.01.014
林松斌1, 冯青阳2, 许剑民2( )
)
收稿日期:2019-09-01
出版日期:2021-01-25
发布日期:2022-07-28
通讯作者:
许剑民
E-mail:xujmin@aliyun.com
基金资助:
LIN Songbin1, FENG Qingyang2, XU Jianmin2()
Received:2019-09-01
Online:2021-01-25
Published:2022-07-28
Contact:
XU Jianmin
E-mail:xujmin@aliyun.com
摘要:
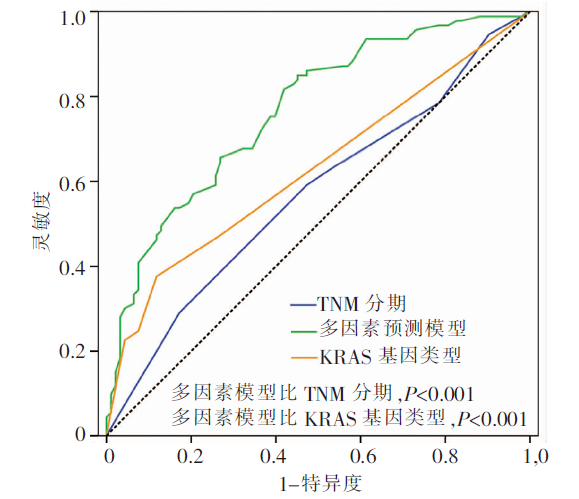
目的:研究结肠直肠癌根治术后异时性远处转移与KRAS基因突变的相关性。方法:回顾性分析结肠直肠癌原发灶根治术后异时性远处转移病人和无转移病人。运用PCR和焦磷酸测序检测KRAS基因类型。通过分析两组病人临床病理因素和KRAS基因类型的差异,寻找预测异时性远处转移的相关因素。结果:共186例病人纳入本研究,异时性远处转移组93例,无转移组93例。KRAS基因突变类型与根治术前CEA (P=0.015)和异时性远处转移(P<0.001)显著相关。多因素分析显示,女性(OR=0.426, P=0.020)、原发灶位于直肠(OR=0.408, P=0.040)、原发灶组织学类型黏液腺癌(OR=0.230, P=0.010)是异时性远处转移的3个独立保护因素;术后pN2分期(OR=4.191, P=0.003)、KRAS基因 p.G12V突变型(OR=10.568, P=0.001)和p.G13D突变型(OR=12.657, P<0.001)是异时性远处转移的2个独立危险因素。以5个独立影响因素建立预测模型,ROC曲线内部效能检验显示预测性能良好,显著优于TNM分期和KRAS基因类型的单因素分析(多因素模型AUC=0.767;TNM分期AUC=0.569;KRAS基因类型AUC=0.628;P<0.001)。结论:KRAS基因p.G12V和p.G13D突变是异时性远处转移的独立危险因素。本研究建立的多因素模型较好预测结肠直肠癌异时性远处转移。
中图分类号:
林松斌, 冯青阳, 许剑民. KRAS基因突变类型预测结肠直肠癌根治术后异时性远处转移[J]. 外科理论与实践, 2021, 26(01): 66-71.
LIN Songbin, FENG Qingyang, XU Jianmin. KRAS genotypes predict metachronous colorectal cancer distant metastases after radical resections[J]. Journal of Surgery Concepts & Practice, 2021, 26(01): 66-71.
表1
KRAS基因突变情况[n(%)]
| 项目 | 总体 | 转移组 | 无转移组 |
|---|---|---|---|
| 总计 | 186 | 93 | 93 |
| 野生型 | 117 (62.9) | 49 (52.7) | 68 (73.1) |
| 突变型 | 69 (37.1) | 44 (47.3) | 25 (26.9) |
| c.35G>A, p.G12D | 23 (12.4) | 9 (9.7) | 14 (15.1) |
| c.35G>T, p.G12V | 16 (8.6) | 12 (12.9) | 4 (4.3) |
| c.34G>T, p.G12C | 2 (1.1) | 0 | 2 (2.2) |
| c.35G>C, p.G12A | 1 (0.5) | 1 (1.1) | 0 |
| c.34G>A, p.G12S | 1 (0.5) | 1 (1.1) | 0 |
| c.34G>C, p.G12R | 1 (0.5) | 0 | 1 (1.1) |
| c.38G>A, p.G13D | 25 (13.4) | 21 (22.6) | 4 (4.3) |
表2
KRAS突变类型与临床病理因素的相关性[n(%)]
| 项目 | 总体 (n=186) | 野生型 (n=117) | c.35G>A,p.G12D (n=23) | c.35G>T,p.G12V (n=16) | c.38G>A,p.G13D (n=25) | 其他突变 类型(n=5) | 检验值 | P值 |
|---|---|---|---|---|---|---|---|---|
| 性别 | 4.080 | 0.259 | ||||||
| 男 | 110 (59.1) | 75 (64.1) | 11 (47.8) | 7 (43.8) | 14 (56.0) | 3 (60.0) | ||
| 女 | 76 (40.9) | 42 (35.9) | 12 (52.2) | 9 (56.2) | 11 (44.0) | 2 (40.0) | ||
| 年龄(岁) | 3.436 | 0.345 | ||||||
| ≤60 | 86 (46.2) | 58 (49.6) | 11 (47.8) | 4 (25.0) | 12 (48.0) | 1 (20.0) | ||
| >60 | 100 (53.8) | 59 (50.4) | 12 (52.2) | 12 (75.0) | 13 (52.0) | 4 (80.0) | ||
| 术前CEA(μg/L) | 10.330 | 0.015a) | ||||||
| <5 | 113 (60.8) | 78 (66.7) | 14 (60.9) | 4 (25.0) | 15 (60.0) | 2 (40.0) | ||
| ≥5 | 73 (39.2) | 39 (33.3) | 9 (39.1) | 12 (75.0) | 10 (40.0) | 3 (60.0) | ||
| 原发灶部位 | 4.347 | 0.637b) | ||||||
| 右半结肠 | 54 (29.0) | 34 (29.1) | 8 (34.8) | 4 (25.0) | 6 (24.0) | 2 (40.0) | ||
| 左半结肠 | 49 (26.3) | 35 (29.9) | 3 (13.0) | 3 (18.8) | 8 (32.0) | 0 | ||
| 直肠 | 83 (44.6) | 48 (41.0) | 12 (52.2) | 9 (56.2) | 11 (44.0) | 3 (60.0) | ||
| 组织学类型 | 1.655 | 0.643b) | ||||||
| 腺癌 | 155 (83.3) | 99 (84.6) | 18 (78.3) | 15 (93.8) | 21 (84.0) | 2 (40.0) | ||
| 黏液腺癌 | 31 (16.7) | 18 (15.4) | 5 (21.7) | 1 (6.2) | 4 (16.0) | 3 (60.0) | ||
| 分化程度 | 3.145 | 0.375 | ||||||
| 高/中分化 | 109 (58.6) | 66 (56.4) | 12 (52.2) | 11 (68.8) | 18 (72.0) | 2 (40.0) | ||
| 低/未分化 | 77 (41.4) | 51 (43.6) | 11 (47.8) | 5 (31.2) | 7 (28.0) | 3 (60.0) | ||
| pT分期 | 5.588 | 0.465b) | ||||||
| 1~2 | 25 (13.4) | 18 (15.4) | 1 (4.3) | 3 (18.8) | 2 (8.0) | 1 (20.0) | ||
| 3 | 65 (34.9) | 36 (30.8) | 10 (43.5) | 4 (25.0) | 12 (48.0) | 3 (60.0) | ||
| 4 | 96 (51.6) | 63 (53.8) | 12 (52.2) | 9 (56.2) | 11 (44.0) | 1 (20.0) | ||
| pN分期 | 11.302 | 0.073a)b) | ||||||
| 0 | 77 (41.4) | 43 (36.8) | 12 (52.2) | 12 (75.0) | 9 (36.0) | 1 (20.0) | ||
| 1 | 66 (35.5) | 41 (35.0) | 6 (26.1) | 3 (18.8) | 12 (48.0) | 4 (80.0) | ||
| 2 | 43 (23.1) | 33 (28.2) | 5 (21.7) | 1 (6.2) | 4 (16.0) | 0 | ||
| 异时性远处转移 | 19.728 | <0.001a) | ||||||
| 无 | 93 (50.0) | 68 (58.1) | 14 (60.9) | 4 (25.0) | 4 (16.0) | 3 (60.0) | ||
| 有 | 93 (50.0) | 49 (41.9) | 9 (39.1) | 12 (75.0) | 21 (84.0) | 2 (40.0) |
表3
异时性远处转移单因素/多因素分析
| 项目 | 单因素分析 | 多因素分析 | |||||
|---|---|---|---|---|---|---|---|
| OR | 95%CI | P值 | OR | 95%CI | P值 | ||
| 性别 | |||||||
| 男 | 1 | - | - | 1 | - | - | |
| 女 | 0.640 | 0.355~1.152 | 0.137 | 0.426 | 0.207~0.876 | 0.020a) | |
| 年龄(岁) | |||||||
| ≤60 | 1 | - | - | 1 | - | - | |
| >60 | 0.841 | 0.472~1.498 | 0.556 | 0.693 | 0.336~1.427 | 0.319 | |
| 术前CEA(μg/L) | |||||||
| <5 | 1 | - | - | 1 | - | - | |
| ≥5 | 1.145 | 0.635~2.063 | 0.652 | 0.899 | 0.444~1.820 | 0.767 | |
| 原发灶部位 | |||||||
| 右半结肠 | 1 | - | - | 1 | - | - | |
| 左半结肠 | 0.656 | 0.301~1.429 | 0.289 | 0.500 | 0.200~1.248 | 0.138 | |
| 直肠 | 0.658 | 0.330~1.312 | 0.234 | 0.408 | 0.173~0.961 | 0.040a) | |
| 组织学类型 | |||||||
| 腺癌 | 1 | - | - | 1 | - | - | |
| 黏液腺癌 | 0.490 | 0.220~1.090 | 0.080 | 0.230 | 0.075~0.709 | 0.010a) | |
| 分化程度 | |||||||
| 高/中分化 | 1 | - | - | 1 | - | - | |
| 低/未分化 | 0.957 | 0.534~1.715 | 0.882 | 1.377 | 0.613~3.093 | 0.439 | |
| pT分期 | |||||||
| 1~2 | 1 | - | - | 1 | - | - | |
| 3 | 1.645 | 0.645~4.197 | 0.297 | 1.304 | 0.416~4.086 | 0.649 | |
| 4 | 1.564 | 0.639~3.826 | 0.327 | 1.182 | 0.397~3.524 | 0.764 | |
| pN分期 | |||||||
| 0 | 1 | - | - | 1 | - | - | |
| 1 | 1.190 | 0.615~2.303 | 0.605 | 1.365 | 0.605~3.083 | 0.454 | |
| 2 | 2.134 | 0.993~4.585 | 0.052 | 4.191 | 1.643~10.691 | 0.003a) | |
| 原发灶术后静脉化疗 | |||||||
| FOLFOX | 1 | - | - | 1 | - | - | |
| XELOX | 1.962 | 0.740~5.198 | 0.175 | 1.806 | 0.590~5.522 | 0.300 | |
| 未化疗 | 0.864 | 0.338~2.210 | 0.761 | 0.580 | 0.181~1.856 | 0.359 | |
| KRAS基因型 | |||||||
| 野生型 | 1 | - | - | 1 | - | - | |
| c.35G>A, p.G12D | 0.892 | 0.358~2.226 | 0.807 | 1.258 | 0.454~3.485 | 0.658 | |
| c.35G>T, p.G12V | 4.163 | 1.267~13.681 | 0.019a) | 10.568 | 2.568~43.499 | 0.001a) | |
| c.38G>A, p.G13D | 7.286 | 2.352~22.567 | 0.001a) | 12.657 | 3.607~44.411 | <0.001a) | |
| 其他突变 | 0.925 | 0.149~5.747 | 0.933 | 2.927 | 0.381~22.493 | 0.302 | |
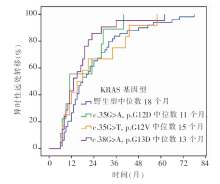
图1
不同KRAS基因型病人异时性远处转移发生中位时间
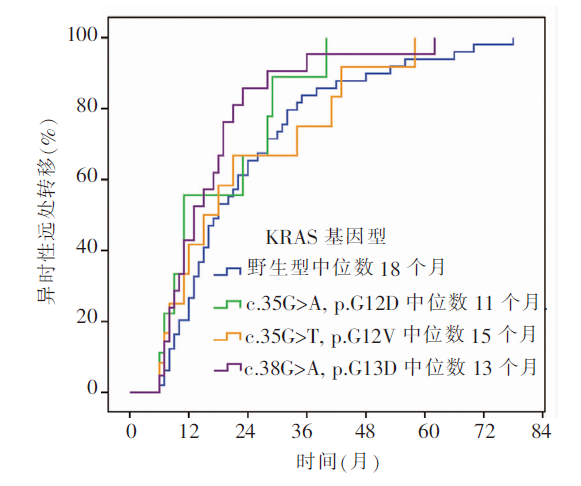

图2
异时性远处转移多因素预测模型
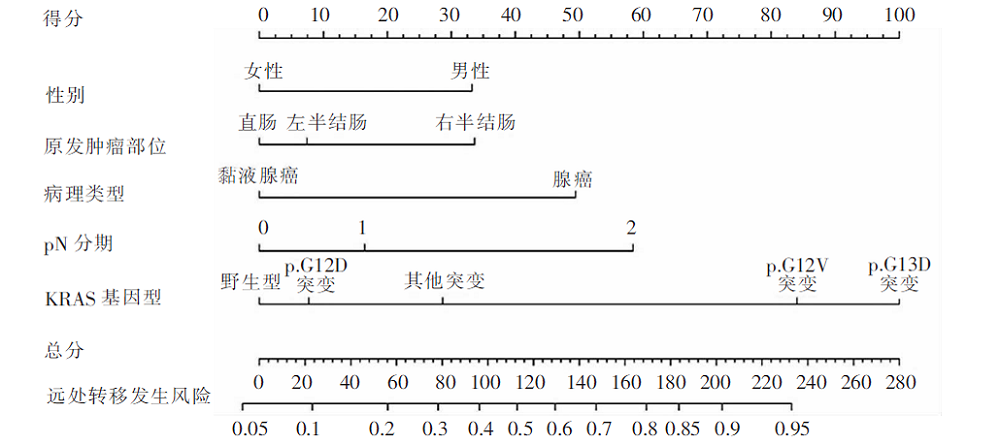
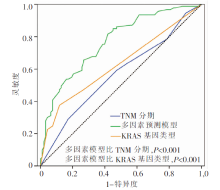
图3
预测模型内部效能检验
| [1] | Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018[J]. CA Cancer J Clin, 2018, 68(1):7-30. |
| [2] | Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015[J]. CA Cancer J Clin, 2016, 66(2):115-132. |
| [3] | 李道娟, 李倩, 贺宇彤. 结直肠癌流行病学趋势[J]. 肿瘤防治研究, 2015, 42(3):305-310. |
| [4] |
Dexiang Z, Li R, Ye W, et al. Outcome of patients with colorectal liver metastasis: analysis of 1,613 consecutive cases[J]. Ann Surg Oncol, 2012, 19(9):2860-2868.
doi: 10.1245/s10434-012-2356-9 pmid: 22526903 |
| [5] | Wang CC, Li J. An update on chemotherapy of colorectal liver metastases[J]. World J Gastroenterol, 2012, 18(1):25-33. |
| [6] | Tsai MS, Su YH, Ho MC, et al. Clinicopathological features and prognosis in resectable synchronous and metachronous colorectal liver metastasis[J]. Ann Surg Oncol, 2007, 14(2):786-794. |
| [7] |
Charette N, Vandeputte C, Starkel P. Ras in digestive oncology: from molecular biology to clinical implications[J]. Curr Opin Oncol, 2014, 26(4):454-461.
doi: 10.1097/CCO.0000000000000088 pmid: 24849046 |
| [8] | Er TK, Chen CC, Bujanda L, et al. Current approaches for predicting a lack of response to anti-EGFR therapy in KRAS wild-type patients[J]. Biomed Res Int, 2014, 2014:591867. |
| [9] | Nash GM, Gimbel M, Shia J, et al. KRAS mutation correlates with accelerated metastatic progression in patients with colorectal liver metastases[J]. Ann Surg Oncol, 2010, 17(2):572-578. |
| [10] |
Bokemeyer C, Bondarenko I, Hartmann JT, et al. Efficacy according to biomarker status of cetuximab plus FOLFOX-4 as first-line treatment for metastatic colorectal cancer: the OPUS study[J]. Ann Oncol, 2011, 22(7):1535-1546.
doi: S0923-7534(19)38435-2 pmid: 21228335 |
| [11] |
van Cutsem E, Tejpar S, Schlichting M, et al. Cetuximab plus irinotecan, fluorouracil, and leucovorin as first-line treatment for metastatic colorectal cancer: updated analysis of overall survival according to tumor KRAS and BRAF mutation status[J]. J Clin Oncol, 2011, 29(15):2011-2019.
doi: 10.1200/JCO.2010.33.5091 pmid: 21502544 |
| [12] | Ye LC, Liu TS, Ren L, et al. Randomized controlled trial of cetuximab plus chemotherapy for patients with KRAS wild-type unresectable colorectal liver-limited metastases[J]. J Clin Oncol, 2013, 31(16):1931-1938. |
| [13] |
Schemper M, Smith TL. A note on quantifying follow-up in studies of failure time[J]. Control Clin Trials, 1996, 17(4):343-346.
doi: 10.1016/0197-2456(96)00075-x pmid: 8889347 |
| [14] |
Silvestri A, Pin E, Huijbers A, et al. Individualized therapy for metastatic colorectal cancer[J]. J Intern Med, 2013, 274(1):1-24.
doi: 10.1111/joim.12070 pmid: 23527888 |
| [15] | Saijo N. Critical comments for roles of biomarkers in the diagnosis and treatment of cancer[J]. Cancer Treat Rev, 2012, 38(1):63-67. |
| [1] | 殷剑光, 宗雅萍, 沈晓卉, 赵敬坤, 陆爱国. 同时性多原发结肠直肠癌治疗与预后分析(附39例报告)[J]. 外科理论与实践, 2022, 27(06): 540-544. |
| [2] | 包全, 邢宝才. 复杂双叶多发性结肠直肠癌肝转移外科治疗策略[J]. 外科理论与实践, 2022, 27(02): 128-130. |
| [3] | 刘诗光, 赵敬坤, 陆爱国, 毛志海. 趋化因子CXCL5和程序性死亡配体 1在结肠直肠癌组织的表达与病人预后的关系[J]. 外科理论与实践, 2021, 26(06): 543-549. |
| [4] | 严美悦, 杨向阳, 戴亭亭, 张书信, 李京向. 改良Kraske术治疗巨大骶前囊肿(附1例报告)[J]. 外科理论与实践, 2021, 26(06): 561-563. |
| [5] | 张华, 陆炜, 杨承翌, 项明洁. 血清人衰老关键蛋白1检测对结肠直肠癌的诊断和预后价值[J]. 诊断学理论与实践, 2021, 20(05): 462-465. |
| [6] | 蔡三军. 结肠直肠癌诊治的思考[J]. 外科理论与实践, 2021, 26(04): 297-299. |
| [7] | 张弢, 叶枫, 赵任. 结肠直肠癌的微创手术——在工具和价值间的不断平衡优化[J]. 外科理论与实践, 2021, 26(04): 300-304. |
| [8] | 杨飖, 傅传刚. NOSES在结肠直肠癌手术中的应用现状与展望[J]. 外科理论与实践, 2021, 26(04): 305-311. |
| [9] | 王常刚, 刘坤, 冯浩然, 蒋奕玫, 施毅卿, 陈献则, 宋子甲, 李军, 李佑, 蔡东莉, 赵任. 结肠直肠癌B7S1表达与免疫浸润的关系[J]. 外科理论与实践, 2021, 26(04): 336-342. |
| [10] | 茅届齐, 徐多刚, 张米粒, 肖蕴誉, 明旭, 李雨哲, 曹灿, 于亮, 李继坤. 结肠直肠癌病人D-二聚体升高的研究[J]. 外科理论与实践, 2021, 26(04): 361-366. |
| [11] | 杨盈赤, 宋建宁, 张忠涛. 中国腹腔镜结肠直肠手术的回顾与展望——基于手术病例登记研究和数据库建立的思考[J]. 外科理论与实践, 2021, 26(04): 277-280. |
| [12] | 顾晋. 局部晚期结肠直肠癌治疗和联合脏器切除[J]. 外科理论与实践, 2021, 26(04): 290-296. |
| [13] | 吴春晓, 龚杨明, 顾凯, 庞怡, 鲍萍萍, 王春芳, 施亮, 向詠梅, 窦剑明, 付晨, 施燕. 2016年上海市结肠直肠癌发病和死亡情况与2002—2016年间的变化趋势分析[J]. 外科理论与实践, 2021, 26(04): 325-335. |
| [14] | 程国柱, 蔡国响. 结肠直肠癌腹膜转移的腹腔药物治疗研究[J]. 外科理论与实践, 2021, 26(01): 34-37. |
| [15] | 关天培, 雷子颖, 崔书中. 结肠直肠癌腹膜转移防治临床研究[J]. 外科理论与实践, 2021, 26(01): 7-10. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||