外科理论与实践 ›› 2022, Vol. 27 ›› Issue (02): 158-164.doi: 10.16139/j.1007-9610.2022.02.014
张磊1, 毛家玺2, 李涛1, 滕飞2( ), 孙克彦1()
), 孙克彦1()
收稿日期:2022-01-17
出版日期:2022-05-25
发布日期:2022-06-16
通讯作者:
滕飞,孙克彦
E-mail:188025796@qq.com;tengfei@smmu.edu.cn
基金资助:
ZHANG Lei1, MAO Jiaxi2, LI Tao1, TENG Fei2(), SUN Keyan1()
Received:2022-01-17
Online:2022-05-25
Published:2022-06-16
Contact:
TENG Fei,SUN Keyan
E-mail:188025796@qq.com;tengfei@smmu.edu.cn
摘要:
目的: 观察肝移植治疗原发性胆汁性胆管炎(primary biliary cholangitis, PBC)的疗效及预后。方法: 回顾性分析上海交通大学医学院附属瑞金医院和上海长征医院2001年1月至2020年12月收治肝移植治疗PBC病人的临床资料。术前免疫炎症反应采用10个免疫炎症指标,包括全身免疫炎症指数、纤维蛋白原以及中性粒细胞、淋巴细胞、单核细胞、血小板、天冬氨酸转氨酶、CD4、CD8之间的比值。根据单核细胞与淋巴细胞的比值以及纤维蛋白原计算、得到评分。评分≥-0.12为高危组,<-0.12为低危组。生存率分析采用寿命表法。多因素分析采用二元Logistic回归模型和COX 回归分析。结果: 82例纳入研究。术后随访至2021年12月31日,时间4.54年(2 d~17.06年)。全部PBC肝移植病人的1、3、5、10、15年生存率为85%、79%、79%、79%、47%。中位生存期为12.92年。多因素分析显示,术前天冬氨酸转氨酶与血小板比值是影响PBC肝移植病人90 d生存的独立危险因素(P=0.013);术前单核细胞与淋巴细胞比值和术前纤维蛋白原是影响PBC病人肝移植术后住院时间的独立危险因素(P=0.002;P=0.007)。高危组总住院时间和住院费用都较低危组明显升高。结论: 术前免疫炎症反应可能影响PBC肝移植病人的近期预后。
中图分类号:
张磊, 毛家玺, 李涛, 滕飞, 孙克彦. 术前免疫炎症反应对原发性胆汁性胆管炎肝移植病人预后影响的双中心回顾性研究[J]. 外科理论与实践, 2022, 27(02): 158-164.
ZHANG Lei, MAO Jiaxi, LI Tao, TENG Fei, SUN Keyan. Effect of preoperative immunoinflammatory response on prognosis in patients undergoing liver transplantation for primary biliary cholangitis: a two-center retrospective study[J]. Journal of Surgery Concepts & Practice, 2022, 27(02): 158-164.
表1
影响PBC肝移植病人长期生存的COX分析(n=82)
| 项目 | 单因素分析 | ||
|---|---|---|---|
| HR | 95%CI | P值 | |
| 年龄(岁) | 0.984 | (0.950,1.019) | 0.370 |
| 性别(男/女) | 0.506 | (0.188,1.361) | 0.177 |
| 术前MELD评分(分) | 1.041 | (0.980,1.106) | 0.195 |
| 术前Child-Pugh评分(分) | 1.104 | (0.864,1.410) | 0.428 |
| 术前免疫炎症指标 | |||
| SII | 0.998 | (0.996,1.000) | 0.067 |
| NLR | 0.981 | (0.804,1.198) | 0.853 |
| MLR | 0.822 | (0.126,5.381) | 0.838 |
| PLR | 0.987 | (0.975,1.000) | 0.054 |
| SIRI | 1.072 | (0.873,1.318) | 0.507 |
| ANRI | 1.000 | (0.993,1.007) | 0.944 |
| ALRI | 0.998 | (0.993,1.003) | 0.388 |
| APRI | 1.120 | (0.822,1.525) | 0.472 |
| FIB | 0.958 | (0.659,1.390) | 0.820 |
| CD4/CD8 | 0.461 | (0.181,1.175) | 0.105 |
| 术后胆道并发症(有/无) | 0.039 | (0.000,18.665) | 0.304 |
| 术后AR(有/无) | 0.734 | (0.230,2.344) | 0.602 |
| 术后PBC复发(有/无) | 0.035 | (0.000,7.673) | 0.222 |
表2
影响PBC肝移植病人90 d生存状态的Logistic分析(n=82)
| 项目 | 单因素分析 | 多因素分析 | |||||
|---|---|---|---|---|---|---|---|
| RR | 95%CI | P值 | RR | 95%CI | P值 | ||
| 年龄(岁) | 0.985 | (0.933,1.040) | 0.579 | ||||
| 性别(男/女) | 0.176 | (0.040,0.774) | 0.021 | ||||
| 术前MELD评分(分) | 1.076 | (0.988,1.172) | 0.094 | ||||
| 术前Child-Pugh评分(分) | 1.271 | (0.885,1.827) | 0.195 | ||||
| 术前免疫炎症指标 | |||||||
| SII | 0.997 | (0.994,1.001) | 0.178 | ||||
| NLR | 1.174 | (0.948,1.453) | 0.141 | ||||
| MLR | 1.893 | (0.184,19.440) | 0.591 | ||||
| PLR | 0.975 | (0.949,1.001) | 0.056 | ||||
| SIRI | 1.175 | (0.910,1.518) | 0.216 | ||||
| ANRI | 1.000 | (0.991,1.010) | 0.940 | ||||
| ALRI | 1.001 | (0.996,1.006) | 0.673 | ||||
| APRI | 1.802 | (1.133,2.866) | 0.013 | 1.802 | (1.133,2.866) | 0.013 | |
| FIB | 0.499 | (0.187,1.330) | 0.165 | ||||
| CD4/CD8 | 0.560 | (0.172,1.824) | 0.336 | ||||
表3
影响PBC病人肝移植术后总住院时间的Logistic分析(n=74)
| 项目 | 单因素分析 | 多因素分析 | |||||
|---|---|---|---|---|---|---|---|
| RR | 95%CI | P值 | RR | 95%CI | P值 | ||
| 年龄(岁) | 1.003 | (0.966,1.040) | 0.895 | ||||
| 性别(男/女) | 0.929 | (0.333,2.591) | 0.887 | ||||
| 术前MELD评分(分) | 1.016 | (0.954,1.081) | 0.626 | ||||
| 术前Child-Pugh评分(分) | 1.090 | (0.866,1.371) | 0.465 | ||||
| 术前免疫炎症指标 | |||||||
| SII | 1.001 | (0.999,1.003) | 0.242 | ||||
| NLR | 1.387 | (1.097,1.752) | 0.006 | ||||
| MLR | 54.275 | (3.713,793.323) | 0.004 | 128.462 | (6.127,2 693.461) | 0.002 | |
| PLR | 1.007 | (0.998,1.016) | 0.149 | ||||
| SIRI | 1.446 | (1.068,1.958) | 0.017 | ||||
| ANRI | 0.995 | (0.987,1.004) | 0.272 | ||||
| ALRI | 1.002 | (0.998,1.006) | 0.371 | ||||
| APRI | 1.174 | (0.813,1.696) | 0.392 | ||||
| FIB | 0.425 | (0.226,0.797) | 0.008 | 0.343 | (0.158,0.744) | 0.007 | |
| CD4/CD8 | 1.024 | (0.621,1.687) | 0.927 | ||||
表4
MF评分高危组与低危组病人的比较[$\bar{x}\pm s$/中位数(最小值~最大值)/n]
| 项目 | 高危组(n=38) | 低危组(n=36) | Z/t/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(岁) | 49±11 | 48±14 | 0.167 | 0.868 |
| 性别(男/女) | 10/28 | 10/26 | 0.020 | 0.887 |
| 术前MELD评分(分) | 23(12~35) | 18(8~36) | 1.791 | 0.003 |
| 术前Child-Pugh评分(分) | 10±2 | 9±2 | 2.476 | 0.016 |
| 术前免疫炎症指标 | ||||
| SII | 344.37(80.57~1 343.95) | 121.16(28.62~1 036.10) | 2.056 | <0.001 |
| NLR | 4.83(1.58~14.36) | 2.45(0.53~6.48) | 2.426 | <0.001 |
| MLR | 0.52(0.21~1.43) | 0.23(0.11~0.60) | 3.156 | <0.001 |
| PLR | 86.16(38.95~277.08) | 78.72(21.13~309.38) | 0.899 | 0.394 |
| SIRI | 1.83(0.26~8.76) | 0.39(0.13~3.64) | 2.546 | <0.001 |
| ANRI | 26.02(2.51~467.74) | 36.46(11.06~185.27) | 1.402 | 0.039 |
| ALRI | 152.55(12.33~737.29) | 97.95(10.90~251.58) | 1.345 | 0.054 |
| APRI | 1.27(0.16~6.64) | 1.10(0.22~3.57) | 1.685 | 0.007 |
| FIB | 1.63(0.51~3.78) | 2.04(1.45~5.89) | 2.037 | <0.001 |
| CD4/CD8 | 1.75(0.82~5.08) | 1.88(0.83~4.53) | 0.603 | 0.860 |
| 术后总住院时间(d) | 47(13~158) | 32(18~84) | 1.515 | 0.020 |
| 术后ICU住院时间(d) | 8(2~73) | 7(5~34) | 0.937 | 0.344 |
| 术后住院费用(万元) | 20.90(12.34~57.90) | 18.33(11.38~32.09) | 1.490 | 0.024 |
| 术后胆道并发症(有/无) | 6/32 | 4/32 | 0.062 | 0.804 |
| 术后AR(有/无) | 11/27 | 5/31 | 2.474 | 0.116 |
| 术后PBC复发(有/无) | 4/34 | 6/30 | 0.187 | 0.666 |
图1
PBC肝移植病人的组间生存分析比较 A:MF评分高危组与低危组病人的90 d生存分析比较;B:MF评分高危组与低危组病人的长期生存分析比较;C:前10年组与后10年组病人的90 d生存分析比较;D:前10年组与后10年组病人的长期生存分析比较。
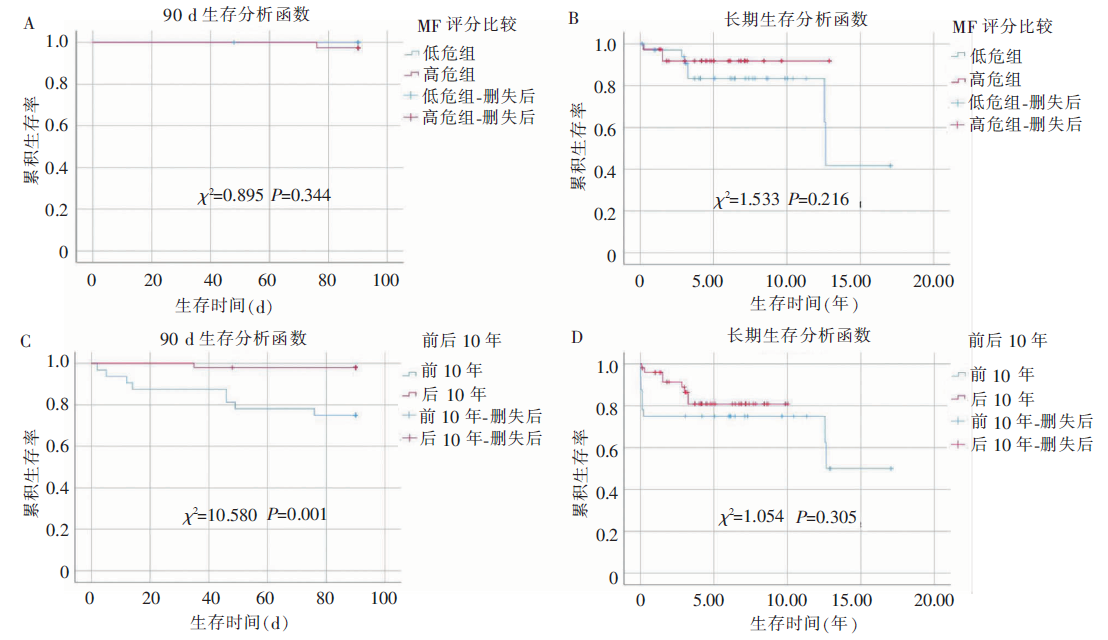
表5
2001—2020年前、后10年病人的比较[$\bar{x}\pm s$/中位数(最小值~最大值)/n]
| 项目 | 前10年组(n=32) | 后10年组(n=50) | Z/t/χ2值 | P值 |
|---|---|---|---|---|
| 年龄(岁) | 50(6~62) | 52(7~72) | 0.745 | 0.635 |
| 性别(男/女) | 12/20 | 13/37 | 1.218 | 0.270 |
| 术前MELD评分(分) | 22(11~38) | 19(8~36) | 1.137 | 0.150 |
| 术前Child-Pugh评分(分) | 10±2 | 9±2 | 2.367 | 0.020 |
| 术后总住院时间(d) | 38(2~80) | 34(13~158) | 0.541 | 0.931 |
| 术后ICU住院时间(d) | 7(2~17) | 8(4~73) | 0.701 | 0.709 |
| 术后住院费用(万元) | 20.04(10.12~57.90) | 18.95(10.67~42.68) | 1.115 | 0.166 |
| 术后胆道并发症(有/无) | 4/28 | 6/44 | 0.000 | 1.000 |
| 术后AR(有/无) | 10/22 | 8/42 | 2.649 | 0.104 |
| 术后PBC复发(有/无) | 6/26 | 4/46 | 1.222 | 0.269 |
| [1] |
Palmer M, Regev A, Lindor K, et al. Consensus guidelines: best practices for detection, assessment and ma-nagement of suspected acute drug‐induced liver injury occurring during clinical trials in adults with chronic cholestatic liver disease[J]. Aliment Pharmacol Ther, 2020, 51(1):90-109.
doi: 10.1111/apt.15579 URL |
| [2] |
Kaplan MM, Gershwin ME. Primary biliary cirrhosis[J]. N Engl J Med, 2005, 353(12):1261-1273.
doi: 10.1056/NEJMra043898 URL |
| [3] |
Lindor KD, Gershwin ME, Poupon R, et al. Primary bi-liary cirrhosis[J]. Hepatology, 2009, 50(1):291-308.
doi: 10.1002/hep.22906 pmid: 19554543 |
| [4] |
Boonstra K, Beuers U, Ponsioen CY. Epidemiology of primary sclerosing cholangitis and primary biliary cirrhosis: a systematic review[J]. J Hepatol, 2012, 56(5):1181-1188.
doi: S0168-8278(12)00043-8 pmid: 22245904 |
| [5] |
Carey EJ, Ali AH, Lindor KD. Primary biliary cirrhosis[J]. Lancet, 2015, 386(10003):1565-1575.
doi: 10.1016/S0140-6736(15)00154-3 URL |
| [6] |
Selmi C, Bowlus CL, Gershwin ME, et al. Primary biliary cirrhosis[J]. Lancet, 2011, 377(9777):1600-1609.
doi: 10.1016/S0140-6736(10)61965-4 URL |
| [7] | 张奉春, 王立, 帅宗文, 等. 原发性胆汁性胆管炎诊疗规范(2021)[J]. 中华内科杂志, 2021, 60(8):709-715. |
| [8] |
Hirschfield GM, Mason A, Luketic V, et al. Efficacy of obeticholic acid in patients with primary biliary cirrhosis and inadequate response to ursodeoxycholic acid[J]. Gastroenterology, 2015, 148(4):751-761, e758.
doi: 10.1053/j.gastro.2014.12.005 pmid: 25500425 |
| [9] |
Pratt DS. Primary biliary cholangitis-a new name and a new treatment[J]. N Engl J Med, 2016, 375(7):685-687.
doi: 10.1056/NEJMe1607744 URL |
| [10] |
Kuiper EMM, Hansen BE, de Vries RA, et al. Improved prognosis of patients with primary biliary cirrhosis that have a biochemical response to ursodeoxycholic acid[J]. Gastroenterology, 2009, 136(4):1281-1287.
doi: 10.1053/j.gastro.2009.01.003 pmid: 19208346 |
| [11] |
Mao JX, Guo WY, Guo M, et al. Acute rejection after liver transplantation is less common, but predicts better prognosis in HBV-related hepatocellular carcinoma patients[J]. Hepatol Int, 2020, 14(3):347-361.
doi: 10.1007/s12072-020-10022-4 URL |
| [12] |
Mao JX, Teng F, Liu C, et al. Immunometabolic inflammation and hepatocellular carcinoma[J]. Hepatobiliary Pancreat Dis Int, 2019, 18(3):298-300.
doi: 10.1016/j.hbpd.2019.03.012 URL |
| [13] | Leung KK, Deeb M, Hirschfield GM. Review article: pathophysiology and management of primary biliary cholangitis[J]. Aliment Pharmacol Ther, 2020, 52(7):1150-1164. |
| [14] |
Ahrens EH, Payne MA, Kunkel HG, et al. Primary bi-liary cirrhosis. 1950[J]. Medicine (Baltimore), 1994, 73(5):264-280.
doi: 10.1097/00005792-199409000-00005 URL |
| [15] |
Sherlock S. Primary billiary cirrhosis (chronic intrahepa-tic obstructive jaundice)[J]. Gastroenterology, 1959, 37:574-586.
doi: 10.1016/S0016-5085(19)35377-6 URL |
| [16] |
Beuers U, Gershwin ME, Gish RG, et al. Changing nomenclature for PBC: from ‘cirrhosis’ to ‘cholangitis’[J]. Gastroenterology, 2015, 149(6):1627-1629.
doi: 10.1053/j.gastro.2015.08.031 URL |
| [17] |
Harms MH, Janssen QP, Adam R, et al. Trends in liver transplantation for primary biliary cholangitis in Europe over the past three decades[J]. Aliment Pharmacol Ther, 2019, 49(3):285-295.
doi: 10.1111/apt.15060 URL |
| [18] |
Parés A, Caballería L, Rodés J. Excellent long-term survival in patients with primary biliary cirrhosis and biochemical response to ursodeoxycholic acid[J]. Gastroenterology, 2006, 130(3):715-720.
doi: 10.1053/j.gastro.2005.12.029 URL |
| [19] |
Corpechot C, Abenavoli L, Rabahi N, et al. Biochemical response to ursodeoxycholic acid and long-term prognosis in primary biliary cirrhosis[J]. Hepatology, 2008, 48(3):871-877.
doi: 10.1002/hep.22428 URL |
| [20] |
Corpechot C, Chazouillères O, Poupon R. Early primary biliary cirrhosis: biochemical response to treatment and prediction of longterm outcome[J]. J Hepatol, 2011, 55(6):1361-1367.
doi: 10.1016/j.jhep.2011.02.031 URL |
| [21] |
Yoo JJ, Cho EJ, Lee B, et al. Prognostic value of biochemical response models for primary biliary cholangitis and the additional role of the neutrophil-to-lymphocyte ratio[J]. Gut Liver, 2018, 12(6):714-721.
doi: 10.5009/gnl18271 URL |
| [1] | 杨雪, 刘锦, 王铮, 陶杰, 郝杰, 李宇, 孙昊. 他克莫司降低肝移植病人ERCP术后胰腺炎发生的临床观察[J]. 外科理论与实践, 2022, 27(3): 253-255. |
| [2] | 吴浩翔, 吕子成, 侯宇宸, 张子杰, 乔子耘, 冯浩, 夏强. 儿童肝移植中他克莫司浓度个体内变异[J]. 外科理论与实践, 2022, 27(02): 145-151. |
| [3] | 黄纪伟, 邱国腾, 曾勇. 肝细胞癌外科治疗进展[J]. 外科理论与实践, 2022, 27(02): 113-118. |
| [4] | 冯浩, 吕子成, 夏强. 肝癌肝移植全过程管理及治疗进展[J]. 外科理论与实践, 2022, 27(02): 119-122. |
| [5] | 杨玲, 范慧倩, 严胜琦. 胆汁淤积性肝病治疗进展[J]. 内科理论与实践, 2022, 17(01): 29-37. |
| [6] | 李涛, 陈皓. 肝硬化门静脉高压症的肝移植治疗[J]. 外科理论与实践, 2021, 26(03): 189-194. |
| [7] | 戚德彬, 陈鹏, 佟辉, 彭承宏, 李涛. 肝移植术后撤除免疫抑制剂的回顾性分析[J]. 外科理论与实践, 2021, 26(03): 231-235. |
| [8] | 黄成, 孙惠川. 《原发性肝癌诊疗规范(2019年版)》肝脏外科领域更新的展望[J]. 外科理论与实践, 2020, 25(01): 6-9. |
| [9] | 佟辉, 陈鹏, 张家强, 谢俊杰, 李涛, 祝哲诚, 彭承宏. 加速康复外科在肝癌肝移植中的临床应用[J]. 外科理论与实践, 2020, 25(01): 45-49. |
| [10] | 华静, 倪茜茜,. 胆汁淤积性肝病的药物治疗进展[J]. 内科理论与实践, 2018, 13(06): 334-338. |
| [11] | 滕飞, 傅志仁. 基于门静脉重建方案的肝移植围术期门静脉血栓处理策略[J]. 外科理论与实践, 2018, 23(03): 191-195. |
| [12] | 宫钰, 胡志强, 黄晓武. 肝移植术后移植物抗宿主病[J]. 外科理论与实践, 2018, 23(03): 196-199. |
| [13] | 佟辉, 张家强, 祝哲诚, 彭承宏, 李涛. 超“UCSF标准”肝细胞癌肝移植术前经肝动脉化疗栓塞的疗效[J]. 外科理论与实践, 2018, 23(03): 241-246. |
| [14] | 李涛, 祝哲诚, 彭承宏. 肝移植“精准”治疗原发性肝脏恶性肿瘤[J]. 外科理论与实践, 2018, 23(03): 200-204. |
| [15] | 李甫, 张晞文,. 肝移植术后胆管狭窄介入诊疗的进展[J]. 外科理论与实践, 2017, 22(06): 538-541. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||