外科理论与实践 ›› 2022, Vol. 27 ›› Issue (04): 330-333.doi: 10.16139/j.1007-9610.2022.04.011
孔祥余1, 梁婷2, 张诚1, 胡海1, 田伏洲3, 项雨凯1, 张红雷1, 吕贝宁1, 杨玉龙1( )
)
KONG Xiangyu1, LIANG Ting2, ZHANG Cheng1, HU Hai1, TIAN Fuzhou3, XIANG Yukai1, Zhang Honglei1, LÜ Beining1, YANG Yulong1()
摘要:
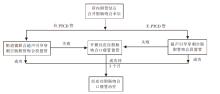
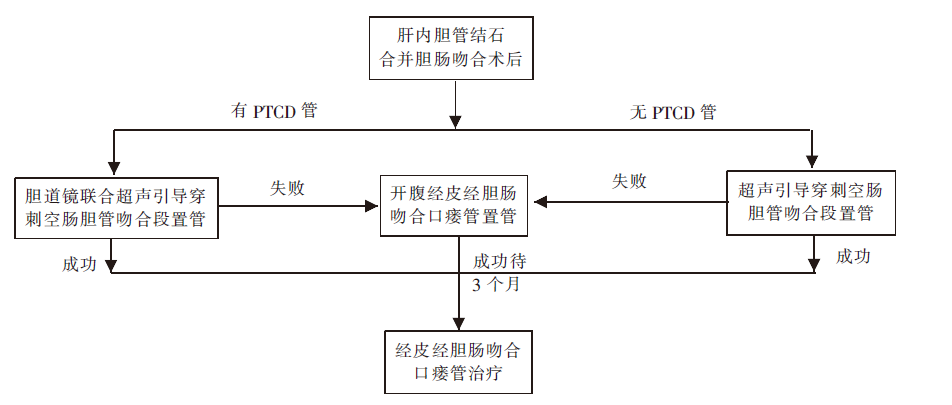
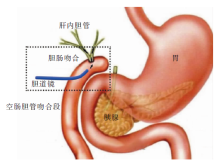
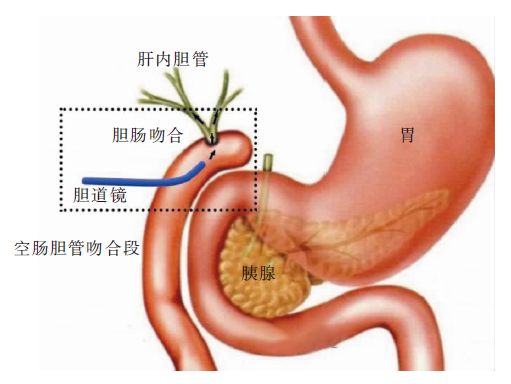
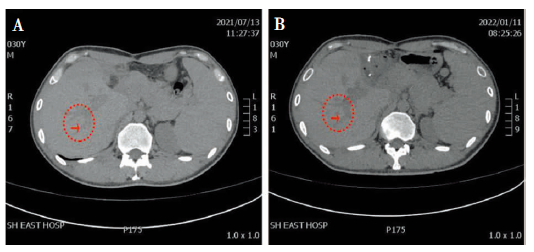
目的:探讨超声引导经皮经胆肠吻合口胆道镜治疗肝内胆管结石的方法及疗效。方法:2021年6月至2022年1月对6例胆肠吻合术后肝内胆管结石病人,在超声引导下经皮经胆肠吻合口建立通道,置入软质胆道镜取出肝内胆管结石,行扩张肝内胆管狭窄和吻合口狭窄的治疗。结果:6例病人经皮经胆肠吻合口置入胆道镜建立通道的方式分别是:3例病人在超声引导下穿刺置入;2例病人经皮经肝穿刺胆管,超声引导置入;1例病人超声引导置管失败,转开腹显示结肠后胆肠吻合,辅助经皮置入胆道镜。6例病人通道位置良好,可顺利进入左、右肝内胆管取石治疗。术后无腹腔出血、无肠瘘、无胆漏、无腹腔感染等近期并发症发生。随访1~6个月,通道形成良好,可反复多次取石、扩张肝内胆管和吻合口狭窄的治疗。结论:超声引导经皮经胆道吻合口治疗肝内胆管结石、肝内胆管狭窄、胆肠吻合口狭窄,具有微创、安全可行、效果良好的优点。
中图分类号: