外科理论与实践 ›› 2024, Vol. 29 ›› Issue (03): 236-242.doi: 10.16139/j.1007-9610.2024.03.09
龚婷婷, 钱爱华, 陈希( )
)
收稿日期:2024-04-26
出版日期:2024-05-25
发布日期:2024-09-03
通讯作者:
陈希,E-mail:cx11977@rjh.com.cn基金资助:
Gong Tingting, Qian Aihua, Chen Xi()
Received:2024-04-26
Online:2024-05-25
Published:2024-09-03
摘要:
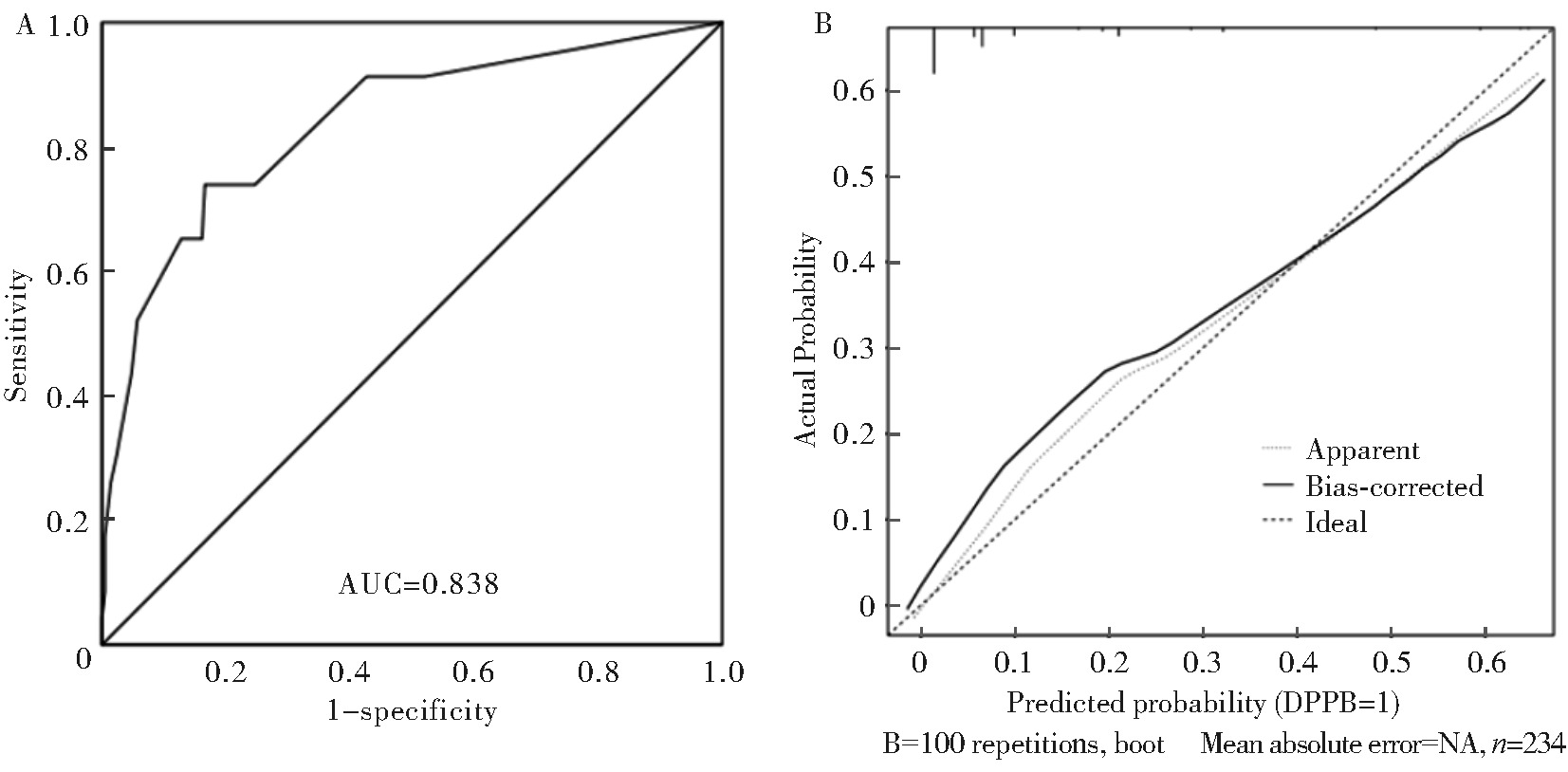
目的:分析早期胃癌内镜黏膜下剥离术(ESD)术后迟发性出血(DPPB)的影响因素并构建列线图模型。方法:收集2021年4月至2023年4月本院行ESD治疗且病理诊断为早期胃癌的234例病人临床资料,依据有无发生DPPB分组,采用Logistic回归分析筛选影响早期胃癌病人ESD后发生DPPB的危险因素;采用R软件构建预测早期胃癌ESD后发生DPPB风险的列线图模型;通过绘制受试者工作特征(ROC)曲线、校准曲线以及Hosmer-Lemeshow拟合优度检验对列线图模型进行评价。结果:234例行ESD治疗的早期胃癌病人中共23例(9.8%)发生DPPB。多因素Logistic回归分析结果显示,活检次数≥3次(95%CI:2.482~20.424,P=0.000)、病变最大直径≥3 cm(95%CI:1.620~13.244,P=0.004)、浸润深度至黏膜下层(95%CI:1.421~10.536,P=0.008)、术中出血(95%CI: 1.160~11.300,P=0.027)是早期胃癌ESD后发生DPPB的独立危险因素。ROC曲线下面积(AUC)为0.838(95%CI:0.743~0.932)。校准曲线斜率接近1。Hosmer-Lemeshow拟合优度检验,χ2=3.328,P=0.505。结论:活检次数≥3次、病变最大直径≥3 cm、浸润深度至黏膜下层、术中出血是早期胃癌ESD后发生DPPB的独立危险因素,基于这4个独立危险因素构建的列线图模型可有效预测早期胃癌ESD后发生DPPB风险。
中图分类号:
龚婷婷, 钱爱华, 陈希. 个体化预测早期胃癌内镜黏膜下剥离术后迟发性出血风险的列线图模型构建[J]. 外科理论与实践, 2024, 29(03): 236-242.
Gong Tingting, Qian Aihua, Chen Xi. Construction of a Nomogram model for personalized prediction of the risk of delayed postoperative bleeding after endoscopic submucosal dissection for early gastric cancer[J]. Journal of Surgery Concepts & Practice, 2024, 29(03): 236-242.
表1
两组病人临床资料比较[n(%)]
| Clinical characteristics | DPPB Group(n=23) | Non-DPPB Group(n=211) | χ2 value | P value | |
|---|---|---|---|---|---|
| Gender | Male | 14(60.9) | 120(56.9) | 0.135 | 0.713 |
| Female | 9(39.1) | 91(43.1) | |||
| Age(years) | ≥60 | 13(56.5) | 114(54.1) | 0.052 | 0.820 |
| <60 | 10(43.5) | 97(45.9) | |||
| BMI(kg/m²) | ≥24 | 9(39.1) | 78(36.9) | 0.042 | 0.838 |
| <24 | 14(60.9) | 133(63.1) | |||
| High blood pressure | Yes | 8(34.8) | 51(24.2) | 1.239 | 0.266 |
| No | 15(65.2) | 160(75.8) | |||
| Diabetes | Yes | 7(30.4) | 43(20.4) | 1.248 | 0.264 |
| No | 16(69.6) | 168(79.6) | |||
| Coronary heart disease | Yes | 9(39.1) | 47(22.3) | 3.237 | 0.072 |
| No | 14(60.9) | 164(77.7) | |||
| Smoking history | Yes | 12(52.2) | 91(43.1) | 0.689 | 0.407 |
| No | 11(47.8) | 120(56.9) | |||
| Alcohol intake history | Yes | 8(34.8) | 82(38.9) | 0.146 | 0.703 |
| No | 15(65.2) | 129(61.1) | |||
| Use of antithrombotic drugs | Yes | 6(26.1) | 17(8.1) | 7.607 | 0.006 |
| No | 17(73.9) | 194(91.9) | |||
| Lesion area | Upper 1/3 | 7(30.4) | 74(35.1) | 0.245 | 0.885 |
| Middle 1/3 | 4(17.4) | 31(14.7) | |||
| Lower 1/3 | 12(52.2) | 106(50.2) | |||
| Morphology of lesions | 0-Ⅰp/0-Ⅰs | 1(4.4) | 34(16.1) | 2.364 | 0.307 |
| 0-Ⅱa-Ⅱc | 21(91.3) | 166(78.7) | |||
| 0-Ⅲ | 1(4.3) | 11(5.2) | |||
| Number of biopsies(times) | ≥3 | 11(47.8) | 27(12.8) | 18.710 | 0.000 |
| <3 | 12(52.2) | 184(87.2) | |||
| Consolidated ulcer | Yes | 10(43.5) | 43(20.4) | 6.316 | 0.012 |
| No | 13(56.5) | 168(79.6) | |||
| Maximum diameter of lesion | ≥3 cm | 15(65.2) | 68(32.2) | 9.861 | 0.002 |
| <3 cm | 8(34.8) | 143(67.8) | |||
| Infiltration depth | T1a | 11(47.8) | 173(81.9) | 14.407 | 0.000 |
| T1b | 12(52.2) | 38(18.1) | |||
| Vascular invasion | No | 20(86.9) | 195(92.4) | 0.829 | 0.363 |
| Yes | 3(13.1) | 16(7.6) | |||
| Curative resection | Yes | 21(91.3) | 195(92.4) | 0.036 | 0.849 |
| No | 2(8.7) | 16(7.6) | |||
| Surgical time (h) | ≥1 | 14(60.9) | 109(51.7) | 0.706 | 0.401 |
| <1 | 9(39.1) | 102(48.3) | |||
| Intraoperative bleeding | ERB-c | 8(34.8) | 17(8.1) | 15.524 | 0.000 |
| ERB-0 | 15(65.2) | 194(91.9) | |||
表2
多因素Logistic分析影响早期胃癌病人ESD后发生DPPB的危险因素
| Factors | Description of assignment | B | Standard error | Wald | P value | OR | 95% confidence interval | |
|---|---|---|---|---|---|---|---|---|
| Lower limit | Upper limit | |||||||
| Number of biopsies (1) | “<3”=0,“≥3”=1 | 1.963 | 0.538 | 13.328 | 0.000 | 7.120 | 2.482 | 20.424 |
| Maximum diameter of lesion (1) | “<3 cm”=0,“≥3 cm”=1 | 1.533 | 0.536 | 8.176 | 0.004 | 4.631 | 1.620 | 13.244 |
| Infiltration depth (1) | “T1a”=0,“T1b”=1 | 1.353 | 0.511 | 7.013 | 0.008 | 3.870 | 1.421 | 10.536 |
| Intraoperative bleeding (1) | “No”=0,“Yes”=1 | 1.287 | 0.581 | 4.908 | 0.027 | 3.620 | 1.160 | 11.300 |
| Constant | -4.254 | 0.582 | 53.418 | 0.000 | 0.014 | |||

图1
早期胃癌病人ESD后发生DPPB风险列线图模型
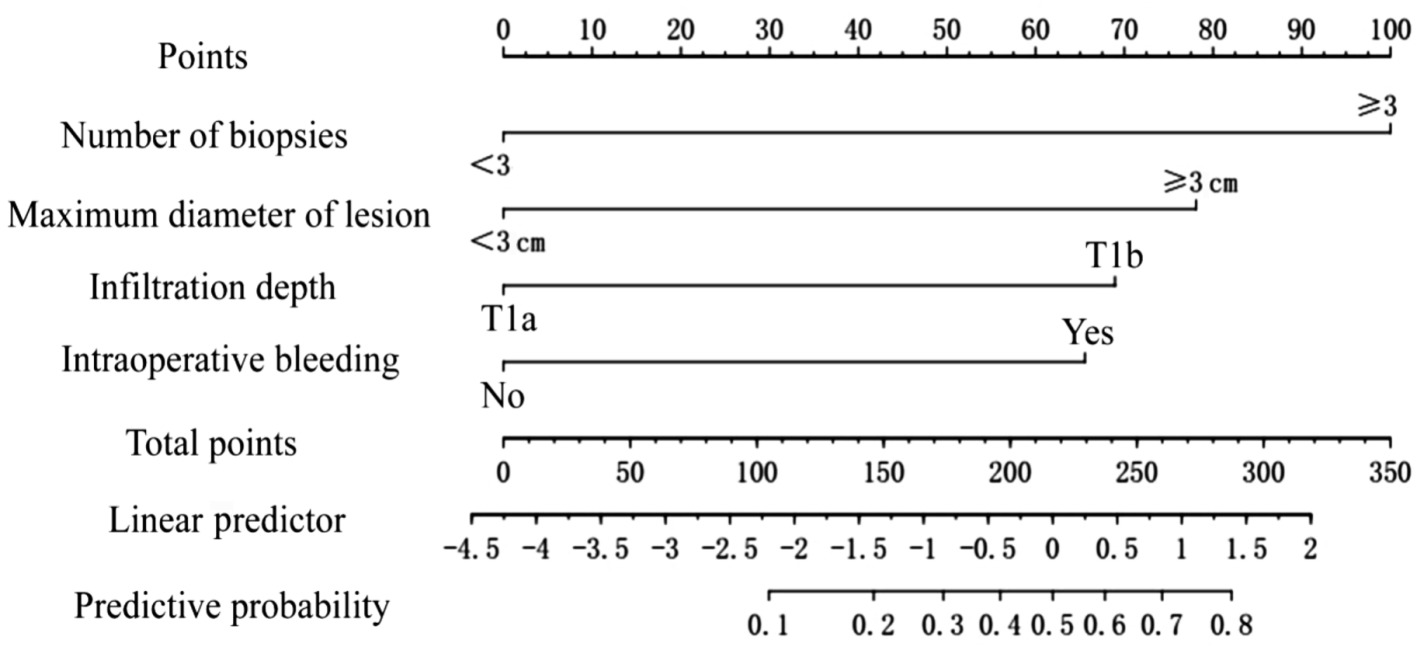
图2
列线图模型的ROC曲线和校准曲线
| [1] | 刘菊梅, 梁丽, 张继新, 等. 411例早期胃癌及癌前病变内镜黏膜下剥离术标本的病理学评估[J]. 北京大学学报(医学版), 2023, 55(2):299-307. |
| LIU J M, LIANG L, ZHANG J X, et al. Pathological evaluation of endoscopic submucosal dissection for early gastric cancer and precancerous lesion in 411 cases[J]. J Peking Univ (Health Sciences), 2023, 55(2):299-307. | |
| [2] | 王冬梅. 早期胃癌患者经内镜黏膜下剥离术治疗的有效性及对患者一次性完整切除率的影响[J]. 实用癌症杂志, 2021, 36(5):828-830. |
| WANG D M. Efficacy of endoscopic submucosal dissection in patients with early gastric cancer and its effect on one-off complete resection rate[J]. Pract J Cancer, 2021, 36(5):828-830. | |
| [3] | 王晓燕, 刘云云, 王玉欣, 等. 内镜黏膜下剥离术治疗早期胃癌及癌前病变效果及继发出血独立危险因素探讨[J]. 临床消化病杂志, 2020, 32(1):21-24. |
| WANG X Y, LIU Y Y, WANG Y X, et al. Clinical effects and independent risk factors for secondary bleeding in patients with early gastric cancer and precancerous lesions treated with endoscopic submuscosal dissection[J]. Chin J Clin Gastroenterol, 2020, 32(1):21-24. | |
| [4] | 朱睿, 马翠云, 闵敏. 消化道早癌内镜黏膜下剥离术术后迟发性出血研究进展[J]. 四川大学学报(医学版), 2022, 53(3):381-385. |
| ZHU R, MA C Y, MIN M. Research progress in delayed bleeding after endoscopic submucosal dissection of early-stage gastrointestinal cancer[J]. J Sichuan Univ (Medical Science), 2022, 53(3):381-385. | |
| [5] | 刘宇航, 赵海英, 王拥军, 等. 预防胃内镜黏膜下剥离术后迟发性出血的研究进展[J]. 中国综合临床, 2023, 39(3):191-195. |
| LIU Y H, ZHAO H Y, WANG Y J, et al. Research progress in preventing delayed bleeding after gastric endoscopic submucosal dissection[J]. Clin Med China, 2023, 39(3):191-195. | |
| [6] | 滕玉芳, 杨华, 徐桂芳, 等. 早期胃癌内镜黏膜下剥离术后幽门螺杆菌未根除风险列线图预测模型构建[J]. 现代医学, 2023, 51(2):183-190. |
| TENG Y F, YANG H, XU G F, et al. Establishment of a nomogram model for predicting Helicobacter pylori positive patients with early gastric cancer after endoscopic submucosal dissection[J]. Mod Med J, 2023, 51(2):183-190. | |
| [7] | 池进有, 何腾飞, 吴玉英, 等. 结直肠息肉内镜下切除术后迟发性出血的危险因素列线图预测模型的构建[J]. 现代消化及介入诊疗, 2020, 25(11):1504-1508. |
| CHI J Y, HE T F, WU Y Y, et al. Construction of a nomogram predictive model for delayed bleeding after endoscopic resection of colorectal polyps[J]. Mod Dig Intervent, 2020, 25(11):1504-1508. | |
| [8] | 北京市科委重大项目《早期胃癌治疗规范研究》专家组. 早期胃癌内镜下规范化切除的专家共识意见(2018,北京)[J]. 中华消化内镜杂志,2019, 36(6):381-392. |
| Expert Group of Beijing Municipal Science and Techno-logy Commission Major Project “Standardization Study on the Treatment of Early Gastric Cancer”. Expert consensus on standardized resection of early gastric cancer by endoscopy (2018, Beijing)[J]. Chin J Dig Endosc,2019, 36(6):381-392. | |
| [9] |
Endoscopic Classification Review Group. Update on the paris classification of superficial neoplastic lesions in the digestive tract[J]. Endoscopy, 2005, 37(6):570-578.
doi: 10.1055/s-2005-861352 pmid: 15933932 |
| [10] | 中华医学会肿瘤学分会,中华医学会杂志社. 中华医学会胃癌临床诊疗指南(2021版)[J]. 中华医学杂志, 2022, 102(16):1169-1189. |
| Chinese Medical Association Oncology Branch,Journal of the Chinese Medical Association. Clinical guidelines for gastric cancer diagnosis and treatment of Chinese Medical Association (2021 edition)[J]. Natl Med J China, 2022, 102(16):1169-1189. | |
| [11] | 朱思莹, 冀明. 早期胃癌的规范化诊断和治疗[J]. 中华内科杂志, 2020, 59(3):236-239. |
| ZHU S Y, JI M. Standardized diagnosis and treatment of early gastric cancer[J]. Chin J Intern Med, 2020, 59(3):236-239. | |
| [12] | 蔡畅, 金小亮, 陆一帆, 等. 早期胃癌内镜黏膜下剥离术后随访研究[J]. 浙江医学, 2023, 45(5):517-522. |
| CAI C, JIN X L, LU Y F, et al. Follow-up study after endoscopic submucosal dissection for early gastric cancer[J]. Zhejiang Med J, 2023, 45(5):517-522. | |
| [13] | 李云, 夏秀丽, 徐超, 等. 内镜下经多隧道黏膜下剥离术和内镜黏膜下剥离术治疗消化道早癌及癌前病变的疗效及安全性[J]. 中国老年学杂志, 2020, 40(3):505-508. |
| LI Y, XIA X L, XU C, et al. Efficacy and safety of endoscopic submucosal dissection through multiple tunnels and endoscopic submucosal dissection for the treatment of early cancer and precancerous lesions of the digestive tract[J]. Chin J Geriatr, 2020, 40(3):505-508. | |
| [14] | 国家消化内镜专业质控中心, 国家消化系统疾病临床医学研究中心上海, 国家消化道早癌防治中心联盟, 等. 中国内镜黏膜下剥离术相关不良事件防治专家共识意见(2020,无锡)[J]. 中华消化内镜杂志,2020, 37(6):390-403. |
| National Gastrointestinal Endoscopy Quality Control Center, National Clinical Research Center for Digestive Di-seases Shanghai, National Alliance for the Prevention and Treatment of Early Digestive Cancer, et al. Expert consensus on the prevention and treatment of adverse events related to endoscopic submucosal dissection in China (2020, Wuxi)[J]. Chin J Dig Endosc,2020, 37(6):390-403. | |
| [15] | 陈静, 朱贞祥, 徐绍莲, 等. 早期胃癌内镜黏膜下剥离术后迟发性出血风险现状及其影响因素分析[J]. 中华保健医学杂志, 2023, 25(1):79-82. |
| CHEN J, ZHU Z X, XU S L, et al. Risk and influencing factors of delayed bleeding after endoscopic submucosal dissection of early gastric cancer[J]. Chin J Care Med, 2023, 25(1):79-82. | |
| [16] | 公宇, 张月明, 朱继庆, 等. 内镜黏膜下剥离术治疗早期胃癌及癌前病变发生迟发性出血的相关因素分析[J]. 中华肿瘤杂志, 2021, 43(8):861-865. |
| GONG Y, ZHANG Y M, ZHU J Q, et al. Analysis of related factors of delayed bleeding after endoscopic submucosal dissection for early gastric cancer and precancerous lesions[J]. Chin J Oncol, 2021, 43(8):861-865. | |
| [17] |
HASHIMOTO M, HATTA W, TSUJI Y, et al. Rebleeding in patients with delayed bleeding after endoscopic submucosal dissection for early gastric cancer[J]. Dig Endosc, 2021, 33(7):1120-1130.
doi: 10.1111/den.13943 pmid: 33539035 |
| [18] | 严海荣, 严苏, 李锐, 等. 早期胃癌内镜黏膜下剥离术后迟发性出血风险预测评分系统的研究[J]. 南京医科大学学报(自然科学版), 2021, 41(9):1348-1353. |
| YAN H R, YAN S, LI R, et al. Research on the scoring system for predicting delayed bleeding after endoscopic submucosal dissection for early gastric cancer[J]. J Nanjing Med Univ (Natural Science), 2021, 41(9):1348-1353. | |
| [19] | 李军, 丁娟, 马志杰. 早期胃癌患者ESD术后迟发性出血危险因素的Logistic回归方程构建及预测价值[J]. 实用癌症杂志, 2023, 38(5):815-819. |
| LI J, DING J, MA Z J. Logistic regression equation construction and predictive value of risk factors for delayed bleeding after ESD surgery in patients with early gastric cancer[J]. Pract J Cancer, 2023, 38(5):815-819. | |
| [20] | 黎嘉妍, 刘倩怡, 刘智尚, 等. 早期结直肠癌内镜黏膜下剥离术后迟发性出血的影响因素分析及预测模型的构建[J]. 结直肠肛门外科, 2022, 28(4):362-365. |
| LI J Y, LIU Q Y, LIU Z S, et al. Analysis of delayed post-polypectomy bleeding after endoscopic submucosal dissection for early colorectal cancer and predictive model construction[J]. J Colorectal & Anal Surg, 2022, 28(4):362-365. | |
| [21] | 王佳旭, 武珊珊, 吕富靖, 等. 止血夹预防早期胃癌内镜黏膜下剥离术后迟发性出血的疗效分析[J]. 中华消化内镜杂志, 2023, 40(2):104-108. |
| WANG J X, WU S S, LÜ F J, et al. Efficacy analysis of hemostatic clips in preventing delayed bleeding after endoscopic submucosal dissection for early gastric cancer[J]. Chin J Dig Endosc, 2023, 40(2):104-108. | |
| [22] | 杨桂凤, 虞敏亚, 杨雪兰. 个体化预测早期消化道肿瘤ESD术后迟发性出血风险的列线图模型的建立[J]. 中华现代护理杂志, 2021, 27(2):164-170. |
| YANG G F, YU M Y, YANG X L. Establishment of a nomogram model for individualized prediction of delayed bleeding risk after ESD surgery for early digestive tract tumors[J]. Chin J Mod Nurs, 2021, 27(2):164-170. | |
| [23] | 张永强. 内镜黏膜下剥离术治疗早期胃癌及癌前病变术后迟发性出血危险因素的meta分析[D]. 山西: 山西医科大学, 2022. |
| ZHANG Y Q. Meta-analysis of risk factors for delayed postoperative bleeding after endoscopic submucosal dissection for early gastric cancer and precancerous lesions[D]. Shanxi: Shanxi Med Univ, 2022. |
| [1] | 程健珊, 张弢, 吴珺玮, 高惠峰, 陈敬贤, 孟志强. 华蟾素片联合肝动脉化疗栓塞术治疗原发性肝细胞癌的临床疗效及其影响因素分析[J]. 外科理论与实践, 2024, 29(04): 351-357. |
| [2] | 林起柱, 刘红枝, 黄霆峰, 范瑞林, 周伟平, 郑树国, 楼健颖, 曾永毅. 基于肝内胆管癌预后模型筛选辅助化疗受益人群[J]. 外科理论与实践, 2024, 29(02): 170-178. |
| [3] | 陆忠晓, 汤杰, 黄文海. 以SEER为基础的列线图构建和胰腺癌病人生存预测[J]. 外科理论与实践, 2024, 29(01): 46-53. |
| [4] | 莫建涛, 曹瑞奇, 任加强, 耿智敏, 仵正, 程亚丽. 意外胆囊癌病人预后列线图模型的构建[J]. 外科理论与实践, 2024, 29(01): 40-45. |
| [5] | 于素悦, 陆爱国. 保留幽门的胃切除术在早期胃癌外科治疗中的应用及相关指南共识解读[J]. 外科理论与实践, 2024, 29(01): 81-86. |
| [6] | 韩华中, 徐春华, 范文阶, 齐志鹏, 李冰, 周平红, 姚礼庆, 钟芸诗, 陆品相. 内镜切除结肠直肠巨大息肉术后留置肛管减压的研究[J]. 外科理论与实践, 2022, 27(04): 351-356. |
| [7] | 程威, 黄雨桦, 王剑, 李幼生. 影响癌性肠梗阻病人预后的多因素分析[J]. 外科理论与实践, 2022, 27(04): 340-345. |
| [8] | 郭良奇, 严志龙, 张谋成. 腹腔镜经胃腔手术治疗胃黏膜下肿瘤和早期胃癌[J]. 外科理论与实践, 2022, 27(04): 380-383. |
| [9] | 於平, 王越, 翟述昱, 王晓彦, 黄梁, 毛恩强. 急诊手术腹部正中切口术后切口并发症的相关危险因素分析[J]. 外科理论与实践, 2020, 25(03): 239-244. |
| [10] | 杨潇, 李琛. 早期胃癌近端胃切除术后消化道重建方式的比较[J]. 外科理论与实践, 2019, 24(06): 560-564. |
| [11] | 陈小松, 吴佳毅, 黄欧, 何建蓉, 朱丽, 李亚芬, 陈伟国, 沈坤炜. 乳腺癌病人前哨淋巴结1~2枚转移、未行腋窝淋巴结清扫:影响因素和预后[J]. 外科理论与实践, 2019, 24(05): 428-433. |
| [12] | 孙迪, 钟芸诗. 内镜黏膜下剥离术治疗早期胃癌的现状及发展[J]. 外科理论与实践, 2019, 24(01): 27-32. |
| [13] | 陈秦俊杰, 项红军, 夏勇, 李俊, 沈锋,. 乙型肝炎相关肝内胆管癌病人术后生存列线图[J]. 外科理论与实践, 2017, 22(02): 151-156. |
| [14] | 李梦娇, 朱正纲,. 近端胃癌根治术消化道重建方式的比较[J]. 外科理论与实践, 2016, 21(03): 269-272. |
| [15] | 毕建威, 郑瑞,. 早期胃癌手术治疗新进展[J]. 外科理论与实践, 2013, 18(01): 7-9. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||