外科理论与实践 ›› 2024, Vol. 29 ›› Issue (06): 537-543.doi: 10.16139/j.1007-9610.2024.06.14
陈俊宗, 刘凯, 汤地( )
)
收稿日期:2023-09-15
出版日期:2024-11-25
发布日期:2025-03-17
通讯作者:
汤地,E-mail: tangdi@mail.sysu.edu.cn基金资助:
CHEN Junzong, LIU Kai, TANG Di()
Received:2023-09-15
Online:2024-11-25
Published:2025-03-17
摘要:
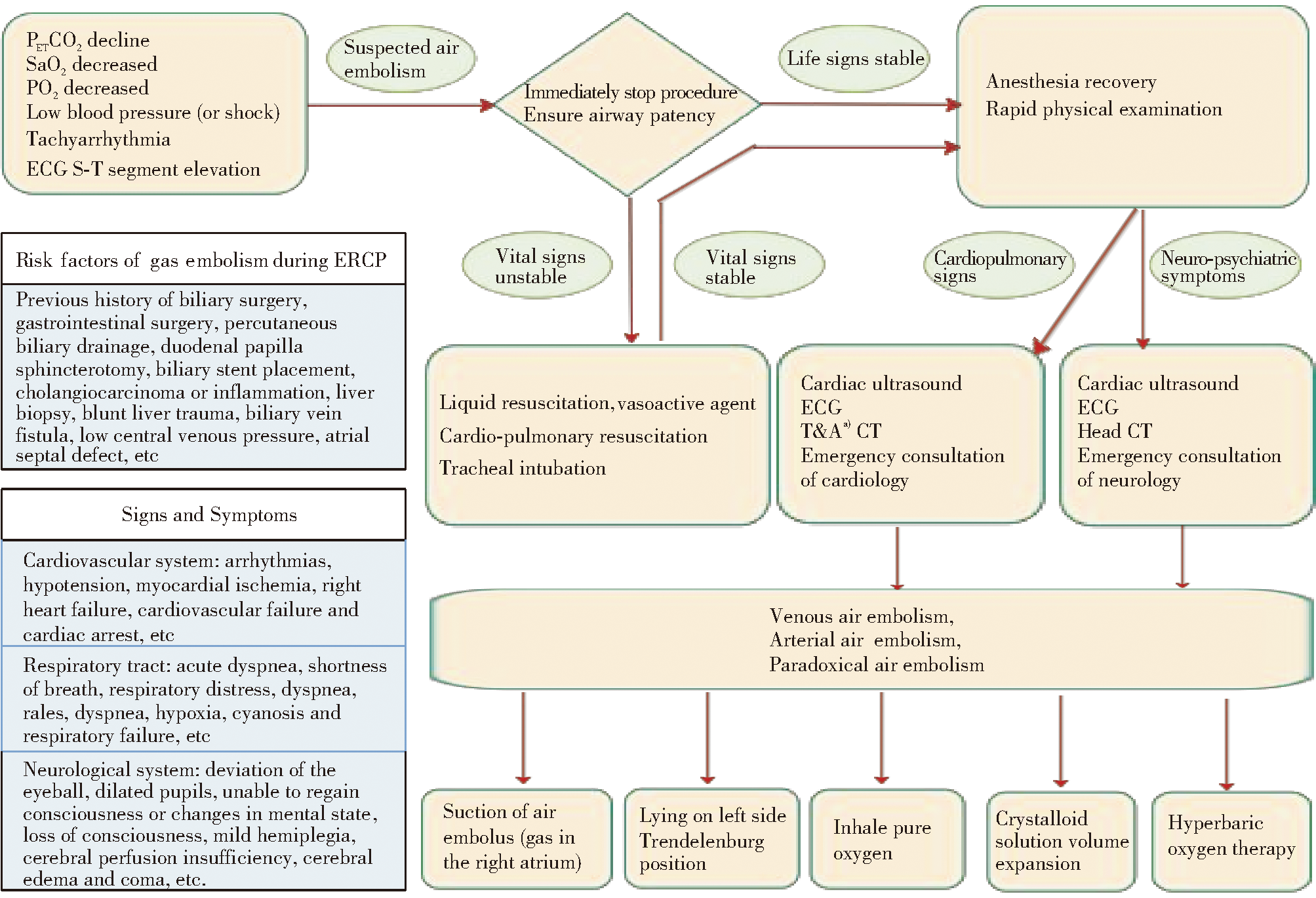
内镜逆行胰胆管造影术(ERCP)是诊治肝胆胰疾病的关键内镜技术。ERCP并发空气栓塞罕见,但具有致死、致残性高以及识别困难等特点,目前对其机制、临床表现及紧急应对策略仍存在不足。空气栓塞需要两个先决条件:开放的血管通路和异常的压力梯度。根据栓塞血管可分为静脉、动脉及反常空气栓塞。其临床表现多样且缺乏特异性,早期识别难度大,在镇静麻醉状态下易被掩盖,易导致延误诊断。主要危险因素包括胆道手术史、乳头括约肌切开、胆-静脉瘘形成、胆道支架植入等。诊断需综合术中生命体征监测、影像学检查以及循环、神经系统评估。治疗核心在于快速识别与干预,包括终止操作、100%氧气吸入、体位调整和保持血液动力学稳定。预防策略强调严格把握ERCP适应证、术前筛查高风险病人、使用CO₂替代空气注气以及加强术中实时监测等。临床医师需具备空气栓塞相关风险意识,通过优化操作流程、完善监测措施及制定应急预案,全面提升对这一危重并发症的防控能力。
中图分类号:
陈俊宗, 刘凯, 汤地. ERCP并发空气栓塞的机制、临床表现与防治措施[J]. 外科理论与实践, 2024, 29(06): 537-543.
CHEN Junzong, LIU Kai, TANG Di. Mechanism, clinical manifestations, prevention, and treatment of air embolism during ERCP[J]. Journal of Surgery Concepts & Practice, 2024, 29(06): 537-543.
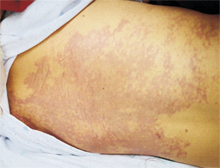
图1
腰背部皮肤大理石样斑纹
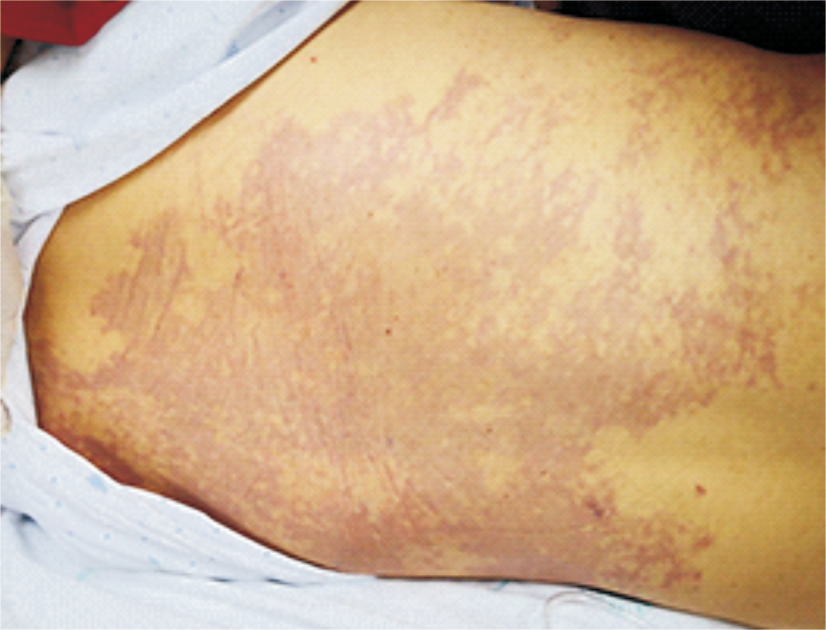
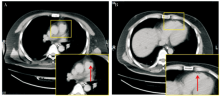
图2
CT显示肺动脉和右心室的少量气体密度影
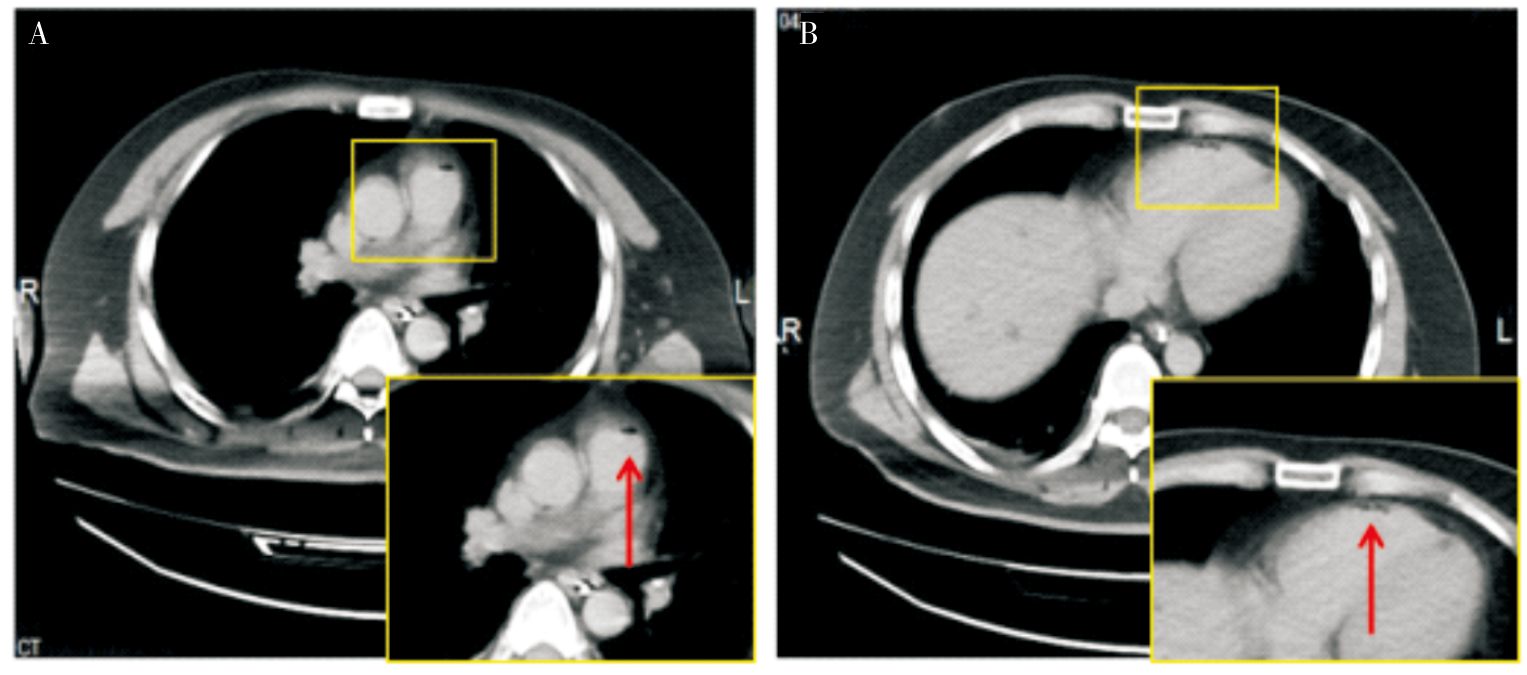

图3
ERCP并发空气栓塞的推荐处置流程图
| [1] |
中华医学会消化内镜学分会ERCP学组, 中国医师协会消化医师分会胆胰学组, 国家消化系统疾病临床医学研究中心. ERCP诊治指南(2018版)[J]. 中国实用内科杂志, 2018, 38(11):1041-1072.
doi: 10.19538/j.nk2018110167 |
| Chinese Society of Digestive Endoscopy, ERCP Group Biliary Pancreatology Group, Chinese Medical Doctor Association Branch of Gastroenterologists, National Clinical Medical Research Center for Digestive Diseases. Chinese guidelines for ERCP(2018)[J]. Chin J Pract Intern Med, 2018, 38(11):1041-1072. | |
| [2] | OLAIYA B, ADLER D G. Air embolism secondary to endoscopy in hospitalized patients: results from the national inpatient sample (1998-2013)[J]. Ann Gastroenterol, 2019, 32(5):476-481. |
| [3] | VOIGT P, SCHOB S, GOTTSCHLING S, et al. Systemic air embolism after endoscopy without vessel injury-a summary of reported cases[J]. J Neurol Sci, 2017,376:93-96. |
| [4] |
AFREEN L K, BRYANT A S, NAKAYAMA T, et al. Incidence of venous air embolism during endoscopic retrograde cholangiopancreatography[J]. Anesth Analg, 2018, 127(2):420-423.
doi: 10.1213/ANE.0000000000003566 pmid: 29933275 |
| [5] | 王晓慧, 陈虹. 空气栓塞的诊治[J]. 临床荟萃, 2016, 31(4):355-358. |
| WANG X H, CHEN H. Advances in diagnosis and treatment of air embolism[J]. Clin Focus, 2016, 31(4):355-358. | |
| [6] |
GORDY S, ROWELL S. Vascular air embolism[J]. Int J Crit Illn Inj Sci, 2013, 3(1):73-76.
doi: 10.4103/2229-5151.109428 pmid: 23724390 |
| [7] | MUTH C M, SHANK E S. Gas embolism[J]. N Engl J Med, 2000, 342(7):476-482. |
| [8] | BRULL S J, PRIELIPP R C. Vascular air embolism: a silent hazard to patient safety[J]. J Crit Care, 2017,42:255-263. |
| [9] | VAN HULST R A, KLEIN J, LACHMANN B. Gas embolism: pathophysiology and treatment[J]. Clin Physiol Funct Imaging, 2003, 23(5):237-246. |
| [10] | LANKE G, ADLER D G. Gas embolism during endoscopic retrograde cholangiopancreatography: diagnosis and management[J]. Ann Gastroenterol, 2019, 32(2):156-167. |
| [11] |
PALMON S C, MOORE L E, LUNDBERG J, et al. Venous air embolism: a review[J]. J Clin Anesth, 1997, 9(3):251-257.
doi: 10.1016/s0952-8180(97)00024-x pmid: 9172037 |
| [12] |
MIRSKI M A, LELE A V, FITZSIMMONS L, et al. Diagnosis and treatment of vascular air embolism[J]. Anesthesiology, 2007, 106(1):164-177.
doi: 10.1097/00000542-200701000-00026 pmid: 17197859 |
| [13] | GHANNAM M, BERAN A, GHAZALEH D, et al. Cerebral air embolism after esophagogastroduodenoscopy: insight on pathophysiology, epidemiology, prevention and treatment[J]. J Stroke Cerebrovasc Dis, 2019, 28(12):104403. |
| [14] | COOPER J S, THOMAS J, SINGH S, et al. Endoscopic bubble trouble: hyperbaric oxygen therapy for cerebral gas embolism during upper endoscopy[J]. J Clin Gastroenterol, 2017, 51(6):e48-e51. |
| [15] |
LOWDON J D, TIDMORE T L JR. Fatal air embolism after gastrointestinal endoscopy[J]. Anesthesiology, 1988, 69(4):622-623.
doi: 10.1097/00000542-198810000-00032 pmid: 3177925 |
| [16] |
SCHLUNDT J, TZANOVA I, WERNER C. A case of intrapulmonary transmission of air while transitioning a patient from a sitting to a supine position after venous air embolism during a craniotomy[J]. Can J Anaesth, 2012, 59(5):478-482.
doi: 10.1007/s12630-012-9680-1 pmid: 22383084 |
| [17] | CEREDA C, STAEDLER C, MOSCHOVITIS G, et al. ‘Bubbles in the brain’: systemic air embolism syndrome from an atrial-oesophageal fistula[J]. Emerg Med J, 2011, 28(5):455. |
| [18] | TRABANCO S, PARDO S, WILLIAMS M, et al. Cerebral air embolism after ERCP[J]. J Clin Anesth, 2017,36:133-135. |
| [19] |
MURPHY B P, HARFORD F J, CRAMER F S. Cerebral air embolism resulting from invasive medical procedures. treatment with hyperbaric oxygen[J]. Ann Surg, 1985, 201(2):242-245.
doi: 10.1097/00000658-198502000-00019 pmid: 3918516 |
| [20] |
DONEPUDI S, CHAVALITDHAMRONG D, PU L, et al. Air embolism complicating gastrointestinal endoscopy: a systematic review[J]. World J Gastrointest Endosc, 2013, 5(8):359-365.
doi: 10.4253/wjge.v5.i8.359 pmid: 23951390 |
| [21] | MAQSOOD M H, MIRZA N, HANIF M A, et al. Clinical presentation, diagnosis, and management of air embolism during endoscopic retrograde cholangiopancreatography[J]. Gastroenterology Res, 2019, 12(6):283-287. |
| [22] |
SISK J M, CHOI M D, CASABIANCA A B, et al. Two cardiac arrests because of venous air embolism during endoscopic retrograde cholangiopancreatography: a case report[J]. A A Case Rep, 2017, 8(3):47-50.
doi: 10.1213/XAA.0000000000000420 pmid: 27898548 |
| [23] |
BECHI A, NUCERA M P, OLIVOTTO I, et al. Complete neurological recovery after systemic air embolism during endoscopic retrograde cholangiopancreatography[J]. Minerva Anestesiol, 2012, 78(5):622-625.
pmid: 22240610 |
| [24] |
GERMONPRE P, BALESTRA C, OBEID G, et al. Cutis marmorata skin decompression sickness is a manifestation of brainstem bubble embolization, not of local skin bubbles[J]. Med Hypotheses, 2015, 85(6):863-869.
doi: 10.1016/j.mehy.2015.09.022 pmid: 26432631 |
| [25] | LIU Y, CHEN J, WANG H, et al. Systemic air embolism during ERCP: a case report and focus on identification and management[J]. Jpn J Gastroenterol Hepatol, 2021, 18(6):1-4. |
| [26] |
PRIELIPP R C, BRULL S J. Vascular air embolism and endoscopy: every bubble matters[J]. Anesth Analg, 2018, 127(2):333-335.
doi: 10.1213/ANE.0000000000003329 pmid: 30028384 |
| [27] |
KATZGRABER F, GLENEWINKEL F, FISCHLER S, et al. Mechanism of fatal air embolism after gastrointestinal endoscopy[J]. Int J Legal Med, 1998, 111(3):154-156.
doi: 10.1007/s004140050137 pmid: 9587799 |
| [28] |
CHAVALITDHAMRONG D, DONEPUDI S, PU L, et al. Uncommon and rarely reported adverse events of endoscopic retrograde cholangiopancreatography[J]. Dig Endosc, 2014, 26(1):15-22.
doi: 10.1111/den.12178 pmid: 24118211 |
| [29] | MACCARONE G, SHAKOOR T, ELLIS B. Air embolism after percutaneous transhepatic biliary drainage and subsequent endoscopic retrograde cholangiopancreatography (ERCP)[J]. Endoscopy, 2011, 43(Suppl 2 UCTN):E399. |
| [30] | PANDIA M P, BITHAL P K, DASH H H, et al. Comparative incidence of cardiovascular changes during venous air embolism as detected by transesophageal echocardiography alone or in combination with end tidal carbon dio-xide tension monitoring[J]. J Clin Neurosci, 2011, 18(9):1206-1209. |
| [31] |
EKMEKTZOGLOU K, ALEXANDRAKIS G, DIMOPO-ULOS K, et al. When in trouble think of the bubble: paradoxical cerebral arterial gas embolism after endoscopic retrograde cholangiopancreatography[J]. Case Rep Gastroenterol, 2021, 15(1):456-469.
doi: 10.1159/000514706 pmid: 34054400 |
| [32] | 王志勇, 纪木火, 吴明浩, 等. 经内镜逆行性胰胆管造影术中空气栓塞抢救成功1例[J]. 中华麻醉学杂志, 2022, 42(9):1124-1125. |
| WANG Z Y, JI M H, WU M H, et al. Successful diagnosis and treatment of air embolism in endoscopic retrograde cholangiopancreatography: a case report[J]. Chin Anesthesiol, 2022, 42(9):1124-1125. | |
| [33] |
COOPER J. Treatment of endoscopy associated cerebral gas embolism[J]. Am J Gastroenterol, 2018, 113(12):1742-1744.
doi: 10.1038/s41395-018-0139-z pmid: 29915395 |
| [34] | ALBIN M S. Venous air embolism: a warning not to be complacent-we should listen to the drumbeat of history[J]. Anesthesiology, 2011, 115(3):626-629. |
| [35] | PASSOS M L, RIBEIRO I B, DE MOURA D, et al. Efficacy and safety of carbon dioxide insufflation versus air insufflation during endoscopic retrograde cholangiopancreatography in randomized controlled trials: a systematic review and meta-analysis[J]. Endosc Int Open, 2019, 7(4):E487-E497. |
| [36] | ZHANG W Y, JIANG X P, MIAO L, et al. Efficacy and safety of carbon dioxide insufflation versus air insufflation for endoscopic retrograde cholangiopancreatography: a meta-analysis update[J]. Clin Res Hepatol Gastroenterol, 2017, 41(2):217-229. |
| [1] | 矫元君, 尹耀新, 李桂贤, 刘吉奎, 林泽伟. 鼻胆管改良胆道支架导致肝穿孔(附1例报告)[J]. 外科理论与实践, 2024, 29(05): 452-454. |
| [2] | 姚文飞, 祁洋, 李谦益, 吴宇权, 徐瑞云, 姚伟, 孔雷, 李能平. 胰管支架表面括约肌预切开与经胰管括约肌预切开在ERCP困难胆管插管中的应用效果比较[J]. 外科理论与实践, 2024, 29(05): 434-440. |
| [3] | 叶枫, 龚笑勇, 任家俊, 蔡强, 陈胜. ERCP在原发性肝癌围术期胆道并发症诊治中的应用[J]. 外科理论与实践, 2023, 28(04): 355-360. |
| [4] | 聂海行, 王帆, 王红玲, 赵秋. ERCP术后胰腺炎的危险因素及预防方法[J]. 外科理论与实践, 2023, 28(04): 310-315. |
| [5] | 董元航, 陈洁. 胰十二指肠切除术后胆胰疾病消化内镜介入策略[J]. 外科理论与实践, 2023, 28(04): 307-309. |
| [6] | 龚笑勇, 陈胜, 任家俊, 叶枫, 蔡强, 蔡琳燕, 刘远滨, 隋亮. SpyGlass内镜直视系统治疗内镜和外科手术治疗失败的困难胆管结石[J]. 外科理论与实践, 2022, 27(03): 215-220. |
| [7] | 翁昊, 翁明哲, 束翌俊, 顾钧, 张文杰, 王雪峰. 乳头球囊扩张及机械碎石先后顺序对ERCP治疗胆总管结石影响的前瞻性研究[J]. 外科理论与实践, 2022, 27(03): 210-214. |
| [8] | 翁昊, 王雪峰. 侧视镜治疗毕Ⅱ式胃切除术后胆管结石的要领与策略[J]. 外科理论与实践, 2022, 27(03): 203-209. |
| [9] | 张敏敏, 邹多武. 超声内镜在可疑胆总管结石诊治中的作用[J]. 外科理论与实践, 2022, 27(03): 193-197. |
| [10] | 胡冰. 困难胆管结石的ERCP诊治[J]. 外科理论与实践, 2022, 27(03): 189-192. |
| [11] | 石加利, 程思乐, 金杭斌, 张筱凤. ERCP联合SpyGlass DS直视下液电碎石治疗困难胆总管结石[J]. 外科理论与实践, 2022, 27(02): 165-168. |
| [12] | 杜重临, 李晓静, 范秋维, 夏一梦. 右美托咪定复合舒芬太尼麻醉在ERCP的效果分析[J]. 外科理论与实践, 2021, 26(03): 240-243. |
| [13] | 周海斌, 金杭斌, 黄海涛, 杨晶, 吕文, 张筱凤, 杨建锋. 内镜逆行胰胆管造影术诊治胰胆汇合异常[J]. 外科理论与实践, 2021, 26(02): 163-166. |
| [14] | 刘宇虹, 邓刚, 陈俊宗(综述), 汤地(审校). 胰胆管汇合异常的诊治进展[J]. 外科理论与实践, 2020, 25(06): 523-528. |
| [15] | 王宏光, 陶丽莹, 郭庆梅. 内镜逆行胰胆管造影联合SpyGlass DS胆道镜治疗胆囊颈结石和急性胆囊炎[J]. 外科理论与实践, 2020, 25(06): 481-485. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||