外科理论与实践 ›› 2025, Vol. 30 ›› Issue (01): 54-60.doi: 10.16139/j.1007-9610.2025.01.10
张男男1a, 郭金星1a( ), 吴钢2, 易辉1b, 周远航1b, 廖芝伟1b, 黄琦1b, 董建1b
), 吴钢2, 易辉1b, 周远航1b, 廖芝伟1b, 黄琦1b, 董建1b
收稿日期:2024-08-16
出版日期:2025-01-25
发布日期:2025-04-25
通讯作者:
郭金星,E-mail: guojinxing@hotmail.com基金资助:
ZHANG Nannan1a, GUO Jinxing1a(), WU Gang2, YI Hui1b, ZHOU Yuanhang1b, LIAO Zhiwei1b, HUANG Qi1b, DONG Jian1b
Received:2024-08-16
Online:2025-01-25
Published:2025-04-25
摘要:
目的: 探讨并建立一个根据术前临床资料预测腹腔镜胆囊切除术(LC)中转开腹可能性的评分体系并以此建立手术分级管理模式。方法: 回顾性研究仁和医院及华山医院2013年6月至2018年6月9 414例行LC病人的临床资料,分为LC组(9 246例)和中转开腹组(168例),将两组资料进行比较,用卡方检验单因素分析筛选出影响中转开腹的危险因素,再对危险因素行Logistic多元回归分析,并根据所建中转开腹可能性函数对危险因素各变量前系数进行赋值,计算每个病例的得分后,比较各得分组的实际中转开腹率的差异。计算受试者工作特征(ROC)曲线下面积评价该评分系统的效能。根据评分体系同时创建LC手术分级管理模式并进行验证。结果: 体温≥38.5℃、急性胆囊炎发作次数≥3次、胆囊壁最大厚度≥5 mm、胆囊颈部结石嵌顿、胆总管直径≥8 mm、术者经验≤50例是中转开腹的危险因素(P<0.001)。评分系统>3分,中转开腹风险高。结论: 该LC评分体系及手术分级管理可靠有效,可降低LC中转开腹率。
中图分类号:
张男男, 郭金星, 吴钢, 易辉, 周远航, 廖芝伟, 黄琦, 董建. 腹腔镜胆囊切除术中转开腹评估体系的建立及手术分级管理探索[J]. 外科理论与实践, 2025, 30(01): 54-60.
ZHANG Nannan, GUO Jinxing, WU Gang, YI Hui, ZHOU Yuanhang, LIAO Zhiwei, HUANG Qi, DONG Jian. Establishment of an evaluation system for conversion to laparotomy in laparoscopic cholecystectomy and exploration of surgical grading management[J]. Journal of Surgery Concepts & Practice, 2025, 30(01): 54-60.
表1
LC组与中转开腹组单因素对比分析 [n(%)/ $\bar{x}±s$]
| Characteristic | LC group (n=9 246) | Transfer laparotomy group(n=168) | χ2 value | P value | |
|---|---|---|---|---|---|
| Gender: male | 4 186(45.3) | 69(41.1) | 1.176 | 0.278 | |
| Age ≥ 65 years | 2 192(23.7) | 41(24.4) | 0.044 | 0.833 | |
| BMI≥ 28 kg/m2 | 280(3.0) | 6(3.6) | 0.165 | 0.684 | |
| Diabetes | 325(3.5) | 10(6.0) | 2.856 | 0.091 | |
| History of upper abdominal surgery | 564(6.1) | 15(8.9) | 2.287 | 0.130 | |
| Body temperature≥38.5℃ | 1 524(16.5) | 105(62.5) | 244.173 | <0.001 | |
| Murphy sign positive | 2 775(30.0) | 110(65.5) | 97.634 | <0.001 | |
| Frequency of acute cholecystitis ≥3 times | 3 246(35.1) | 96(57.1) | 34.991 | <0.001 | |
| Duration of acute cholecystitis ≤72 h | 3 452(37.3) | 68(40.5) | 0.695 | 0.404 | |
| Total bilirubin ≥23 μmolL | 1 235(13.4) | 58(34.5) | 62.393 | <0.001 | |
| Maximum cross-section of gallbladder ≥5 cm×10 cm or ≤ 3 cm×4 cm | 1 975(21.4) | 32(19.0) | 0.526 | 0.468 | |
| Maximum thickness of gallbladder wall ≥5 mm | 1 885(20.4) | 72(42.9) | 50.593 | <0.001 | |
| Gallbladder neck stone incarceration | 1 025(11.1) | 60(35.7) | 98.149 | <0.001 | |
| Diameter of common bile duct ≥8 mm | 725(7.8) | 62(36.9) | 181.928 | <0.001 | |
| Surgical experience | ≤50 cases | 835(9.0) | 78(46.4) | 280.787 | <0.001 |
| 51-200 cases | 2 864(31.0) | 55(32.7) | |||
| >200 cases | 5 547(60.0) | 35(20.8) | |||
表2
Logistic回归模型各因素统计结果
| Characteristic | Regression coefficient | Wald χ2 | P value | OR | 95% CI | |
|---|---|---|---|---|---|---|
| Body temperature≥38.5℃ | 1.578 | 72.113 | <0.001 | 4.847 | 3.367-6.978 | |
| Frequency of acute cholecystitis ≥3 times | 0.754 | 19.266 | <0.001 | 2.125 | 1.518-2.976 | |
| Maximum thickness of gallbladder wall ≥5 mm | 1.195 | 46.175 | <0.001 | 3.305 | 2.341-4.666 | |
| Gallbladder neck stone incarceration | 1.667 | 76.388 | <0.001 | 5.297 | 3.645-7.698 | |
| Diameter of common bile duct ≥8 mm | 1.858 | 98.958 | <0.001 | 6.414 | 4.447-9.249 | |
| Surgical experience | ≤50 cases | 2.09 | 80.443 | <0.001 | 8.088 | 1.816-4.419 |
| 51-200 cases | 1.041 | 21.077 | <0.001 | 2.833 | 5.122-12.771 | |
表3
各风险因素赋值
| Evaluate project | Scores | |
|---|---|---|
| Body temperature≥38.5℃ | 1.5 | |
| Frequency of acute cholecystitis ≥3 times | 0.5 | |
| Maximum thickness of gallbladder wall ≥5 mm | 1 | |
| Gallbladder neck stone incarceration | 1.5 | |
| Diameter of common bile duct ≥8 mm | 2 | |
| Surgical experience | >200 cases | 0 |
| 51-200 cases | 1 | |
| ≤50 cases | 2 | |
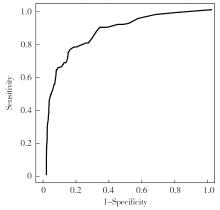
图1
Logistic回归模型ROC曲线
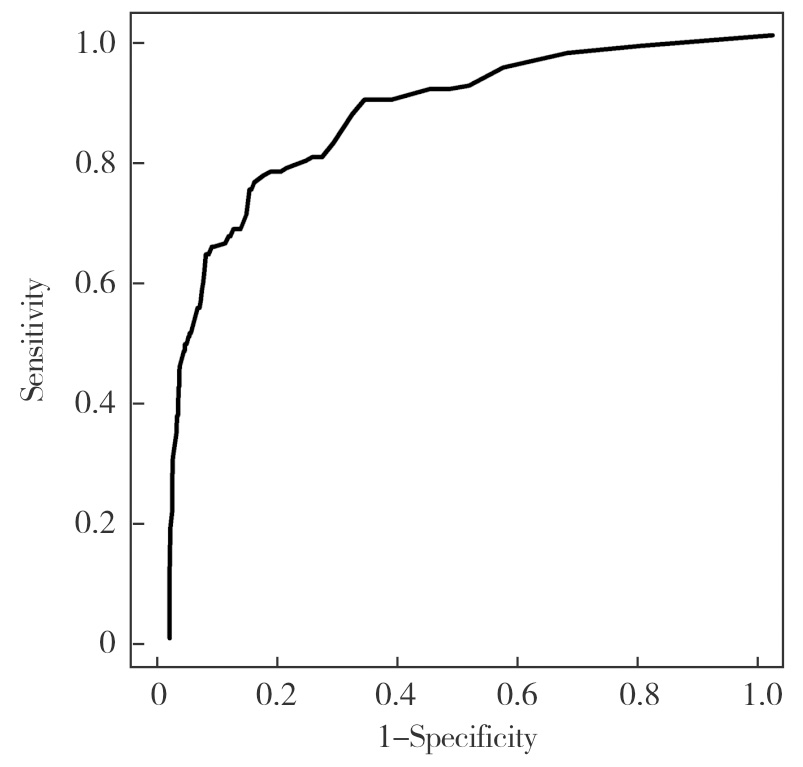
表4
LC手术分级管理量表
Surgical experience Objective factor scale evaluation score: X | X>3 | 2<X≤3 | 1<X≤2 | X≤1 |
|---|---|---|---|---|
| ≤50 cases | high-risk | high-risk | high-risk | LC |
| 51-200 cases | high-risk | high-risk | LC | LC |
| >200 cases | high-risk | LC | LC | LC |
表5
使用LC手术分级管理前后对比[n(%)]
| Item | Before use | After use | χ2 value | P value |
|---|---|---|---|---|
| LC cases | 9 414 | 620 | ||
| Direct laparotomy | 0 | 15 | ||
| Conversion to laparotomy | 168(1.78) | 4(0.65) | 4.482 | <0.05 |
| [1] |
LE V H, SMITH D E, JOHNSON B L. Conversion of laparoscopic to open cholecystectomy in the current era of laparoscopic surgery[J]. Am Surg, 2012, 78(12):1392-1395.
pmid: 23265130 |
| [2] | PHILIP ROTHMAN J, BURCHARTH J, POMMERGAARD H C, et al. Preoperative risk factors for conversion of laparoscopic cholecystectomy to open surgery-a systematic review and meta-analysis of observational studies[J]. Dig Surg, 2016, 33(5):414-423. |
| [3] |
HUSSAIN A. Difficult laparoscopic cholecystectomy: current evidence and strategies of management[J]. Surg Laparosc Endosc Percutan Tech, 2011, 21(4):211-217.
doi: 10.1097/SLE.0b013e318220f1b1 pmid: 21857467 |
| [4] | BOURGOUIN S, MANCINI J, MONCHAL T, et al. How to predict difficult laparoscopic cholecystectomy proposal for a simple preoperative scoring system[J]. Am J Surg, 2016, 212(5):873-881. |
| [5] | 陆昌友, 徐勇, 薛瑞丰, 等. 预防腹腔镜胆囊切除术中胆管损伤的单中心经验[J]. 肝胆外科杂志, 2022, 30(1):48-51. |
| LU C Y, XU Y, XUE R F, et al. Pereventing bile duct injury in laparoscopic cholecystectomy: single-center experience[J]. J Hepatobiliary Surgery, 2022, 30(1):48-51. | |
| [6] | INOUE K, UENO T, DOUCHI D, et al. Risk factors for difficulty of laparoscopic cholecystectomy in grade Ⅱ acute cholecystitis according to the Tokyo guidelines 2013[J]. BMC Surg, 2017, 17(1):114. |
| [7] | ABELSON J S, AFANEH C, RICH B S, et al. Advanced laparoscopic fellowship training decreases conversion rates during laparoscopic cholecystectomy for acute biliary diseases: a retrospective cohort study[J]. Int J Surg, 2015,13:221-226. |
| [8] | 彭腊玲, 刘琳, 卜春花, 等. 急症腹腔镜胆囊切除术中转开腹的预警模型构建与验证[J]. 腹腔镜外科杂志, 2022, 27(6):447-453. |
| PENG L L, LIU L, PIAO C H, et al. Construction and verification of an early warning model for switching to laparotomy during emergency laparoscopic cholecystectomy[J]. J Laparosc Surg, 2022, 27(6):447-453. | |
| [9] | 胡国治, 蔡国英, 郭永忠, 等. 508例急性胆囊炎行腹腔镜胆囊切除术的量化手术指征探讨[J]. 中国内镜杂志, 2007, 13(7):735-737. |
| HU G Z, CAI G Y, GUO Y Z, et al. Study in the quan-tiatative operative indication of laparoscopic cholesystectomy in acute cholesystitis[J]. China J Endosc, 2007, 13(7):735-737. | |
| [10] | JOSHI M R, BOHARA T P, RUPAKHETI S, et al. Pre-operative prediction of difficult laparoscopic cholecystectomy[J]. J Nepal Med Assoc, 2015, 53(200):221-226. |
| [11] | RAMAN J D, LIN Y K, SHARIAT S F, et al. Preoperative nomogram to predict the likelihood of complications after radical nephroureterectomy[J]. BJU Intern, 2017, 119(2):268-275. |
| [12] | 吴品飞, 刘杰凡, 顾勇劲, 等. 腹腔镜胆囊切除术中转开腹200例危险因素分析[J]. 肝胆胰外科杂志, 2016, 28(4):329-331. |
| WU P F, LIU J F, GU Y J, et al. Analysis of risk factors in 200 cases of laparoscopic cholecystectomy switching to laparotomy[J]. J Hepatopancreatobiliary Surg, 2016, 28(4):329-331. | |
| [13] | 仝仲凯, 郝志强, 王志斌. 急性结石性胆囊炎患者腹腔镜胆囊切除术中转开腹手术的影响因素分析[J]. 中国临床医生杂志, 2022, 50(12):1474-1476. |
| TONG Z K, HAO Z Q, WANG Z B. Analysis of factors influencing conversion to open surgery in laparoscopic cholecystectomy of patients with acute calculous cholecystitis[J]. Chin J Clin, 2022, 50(12):1474-1476. | |
| [14] |
AL MASRI S, SHAIB Y, EDELBI M, et al. Predicting conversion from laparoscopic to open cholecystectomy: a single institution retrospective study[J]. World J Surg, 2018, 42(8):2373-2382.
doi: 10.1007/s00268-018-4513-1 pmid: 29417247 |
| [15] | 邹细光, 朱芬如, 袁亚敏, 等. 急性结石性胆囊炎LC中转开腹影响因素分析[J]. 江西医药, 2022, 57(11):1832-1834. |
| ZOU X G, ZHU F R, YUAN Y M, et al. Analysis of inf-luencing factors of LC transition to laparotomy in acute calculous cholecystitis[J]. Jiangxi Med J, 2022, 57(11):1832-1834. | |
| [16] |
TOSUN A, HANCERLIOGULLARI K O, SERIFOGLU I, et al. Role of preoperative sonography in predicting conversion from laparoscopic cholecystectomy to open surgery[J]. Eur J Radiol, 2015, 84(3):346-349.
doi: S0720-048X(14)00574-9 pmid: 25579475 |
| [17] |
BEKSAC K, TURHAN N, KARAAGAOGLU E, et al. Risk factors for conversion of laparoscopic cholecystectomy to open surgery: a new predictive statistical model[J]. J Laparoendosc Adv Surg Tech A, 2016, 26(9):693-696.
doi: 10.1089/lap.2016.0008 pmid: 27385483 |
| [18] | JAMEEL S M, BAHADDIN M M, MOHAMMED A A. Grading operative findings at laparoscopic cholecystectomy following the new scoring system in Duhok governorate: cross sectional study[J]. Ann Med Surg (Lond), 2020, 23(60):266-270. |
| [19] | 董汉华, 武齐齐, 陈孝平. 急性胆道感染东京指南(2018版)更新解读[J]. 临床外科杂志, 2019, 27(1):5-9. |
| DONG H H, WU Q Q, CHEN X P. Tokyo guidelines for acute biliary tract infections (2018) updated interpretation[J]. J Clin Surg,2019, 27(1):5-9. | |
| [20] | 满高亚, 党同科, 吴清松. Rouviere沟引导胆囊后隧道解剖用于困难腹腔镜胆囊切除术[J]. 外科理论与实践, 2022, 27(3):239-243. |
| MAN G Y, DANG T K, WU Q S. Rouviere’s sulcus guided retro-gallbladder tunnel dissection in difficult laparoscopic cholecystectomy[J]. J Surg Concepts Pract, 2022, 27(3):239-243. |
| [1] | 宋春林, 罗成军, 朱雨. 四肢创伤性软组织缺损患者游离皮瓣移植失败的危险因素及预测模型构建 [J]. 组织工程与重建外科杂志, 2024, 20(3): 305-. |
| [2] | 续慧民, 高红霞. 髂股静脉术后支架内再狭窄因素的分析及处理[J]. 外科理论与实践, 2024, 29(06): 481-486. |
| [3] | 吴昕菀, 李响, 郑旻嘉, 姚俊岩. 影响老年病人全身麻醉非心脏手术术后谵妄发生的因素[J]. 外科理论与实践, 2024, 29(06): 510-517. |
| [4] | 李健文, 张云, 乐飞. 腹腔镜腹壁切口疝修复术中腹壁功能重建[J]. 外科理论与实践, 2024, 29(04): 285-291. |
| [5] | 韩海峰, 逯景辉. 原发性腹壁肿瘤的微创手术治疗[J]. 外科理论与实践, 2024, 29(04): 311-315. |
| [6] | 张一忠, 汤睿, 王廷峰, 司仙科, 叶乐斌, 柳楠, 项世骏, 吴卫东. 侧方入路单孔腹腔镜完全腹膜外腹股沟疝修补术(附110例报告)[J]. 外科理论与实践, 2024, 29(04): 323-328. |
| [7] | 姚宏伟, 魏鹏宇, 高加勒, 张忠涛. 腹腔镜结肠直肠癌手术的标准化操作、质量控制与疗效评价[J]. 外科理论与实践, 2024, 29(03): 187-191. |
| [8] | 张鲁阳, 鞠萍, 周雪亮, 邵岩飞, 吴超, 王佳玉, 孙晶, 潘睿俊, 蔡伟. 进阶整合二段式腹腔镜模拟培训课程在外科住院医师规范化培训中的应用探讨[J]. 外科理论与实践, 2024, 29(03): 249-253. |
| [9] | 邵新淋, 朱雪梅, 曹华. 结缔组织病相关间质性肺疾病危险因素及发病机制研究进展[J]. 诊断学理论与实践, 2024, 23(02): 202-209. |
| [10] | 李书乐, 陆录. 腹腔镜供肝获取手术的发展与展望[J]. 外科理论与实践, 2024, 29(02): 121-125. |
| [11] | 路志宇, 孙骥, 杜加录, 蒙轩, 罗漫, 刘玥, 王宏光. 腹腔镜解剖性半肝切除中肝蒂处理与吲哚菁绿剂量影响荧光染色效果的研究[J]. 外科理论与实践, 2024, 29(02): 138-142. |
| [12] | 张莹莹, 李华, 管佳琴, 等.
乳腺癌患者术后早期上肢淋巴水肿的发生率及影响因素分析
[J]. 组织工程与重建外科杂志, 2023, 19(3): 242-. |
| [13] | 詹崇文, 沈奇伟, 邵怡凯, 许博, 花荣, 姚琪远. 三孔法腹腔镜胃袖状切除术治疗肥胖症的疗效分析[J]. 外科理论与实践, 2023, 28(05): 463-468. |
| [14] | 聂海行, 王帆, 王红玲, 赵秋. ERCP术后胰腺炎的危险因素及预防方法[J]. 外科理论与实践, 2023, 28(04): 310-315. |
| [15] | 骆洋, 俞旻皓, 叶光耀, 林海萍, 贡婷月, 李浩, 钟鸣. 术中吲哚菁绿荧光显像评估在降低腹腔镜直肠癌术后吻合口漏的应用价值[J]. 外科理论与实践, 2023, 28(03): 249-253. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||