Journal of Surgery Concepts & Practice ›› 2023, Vol. 28 ›› Issue (06): 512-519.doi: 10.16139/j.1007-9610.2023.06.05
• Experts forum • Previous Articles Next Articles
XU Bojin, PENG Wenfang, HUANG Shan( )
)
Received:2023-11-20
Online:2023-11-25
Published:2024-03-04
CLC Number:
XU Bojin, PENG Wenfang, HUANG Shan. Interpretation of the 2022 edition of “guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis in China”[J]. Journal of Surgery Concepts & Practice, 2023, 28(06): 512-519.
Tab 1
Causes of thyrotoxicosis
| 甲状腺毒症类别 | 甲状腺毒症病因 |
|---|---|
| 甲亢 | 弥漫性毒性甲状腺肿,即GD |
| 毒性多结节性甲状腺肿(toxic multinodular goiter, TMNG) | |
| 毒性甲状腺腺瘤(toxic adenoma, TA) | |
| 碘致甲亢 | |
| 自身免疫性新生儿甲亢 | |
| 家族性非自身免疫性甲亢 | |
| 散发性非自身免疫性甲亢 | |
| 功能性甲状腺癌转移 | |
| 分泌促甲状腺激素(thyroid stimulating hormone, TSH)的垂体腺瘤 | |
| 甲状腺激素抵抗(T3受体β突变) | |
| 人绒毛膜促性腺激素(human chorionic gonadotrophin, hCG)相关甲亢 | |
| 妊娠一过性甲状腺毒症(gestational transient thyrotoxicosis, GTT) | |
| 妊娠滋养细胞肿瘤:葡萄胎、绒毛膜癌 | |
| 卵巢甲状腺肿 | |
| 非甲亢 | 亚急性甲状腺炎 |
| 桥本甲状腺炎 | |
| 无痛性甲状腺炎,产后甲状腺炎 | |
| 急性甲状腺炎 | |
| 人为甲状腺毒症 |
Tab 2
Indicators for thyrotoxicosis examination and application recommendations
| 检查指标 | 应用建议 |
|---|---|
| FT3和FT4 | 诊断甲状腺毒症的主要指标 需注意生理(如年龄、妊娠、季节等)、病理、药物等因素的干扰 |
| TSH | 诊断甲状腺毒症最敏感的指标 需排除影响TSH测定的相关因素 需对TSH水平降低原因进行鉴别 |
| TRAb | 有助于甲状腺毒症的病因鉴别和GD的诊断 |
| TPOAb和TgAb | 用于甲状腺相关自身免疫病因诊断 不能根据高滴度血清水平诊断GD |
| 131I摄取率 | 辅助甲状腺毒症的病因鉴别 |
| 甲状腺静态显像 | 可用于甲状腺毒症病因鉴别,还有助于鉴别结节功能和发现异位甲状腺 |
| 甲状腺超声 | 鉴别甲状腺毒症病因的重要影像学手段 |
Tab 3
Diagnostic criteria for thyrotoxicosis and GD
| 甲状腺毒症诊断 | GD诊断 | |
|---|---|---|
| 病史 临床表现 FT3、FT4和TSH水平 | 必备 条件 | ① 甲亢诊断成立 |
| ② 甲状腺弥漫性肿大,少数病例可无甲状腺肿大 | ||
| 具备 其一 | ③ 眼睑退缩和其他提示Graves眼病(Graves' orbitopathy, GO)的眼征 | |
| ④ 皮肤黏液性病变如胫前黏液性水肿或指端粗厚 | ||
| ⑤ 第三代方法检测的TRAb阳性 | ||
Tab 4
Burch-Wartofsky point scale[1]
| 指标类别 | 标准 | 分数 | |
|---|---|---|---|
| 体温调节 障碍 | 体温(℃) | 37.2~37.7 | 5 |
| 37.8~38.3 | 10 | ||
| 38.4~38.8 | 15 | ||
| 38.9~39.3 | 20 | ||
| 39.4~39.9 | 25 | ||
| ≥40 | 30 | ||
| 心血管 系统 | 心动过速 (次/min) | 100~109 | 5 |
| 110~119 | 10 | ||
| 120~129 | 15 | ||
| 130~139 | 20 | ||
| ≥140 | 25 | ||
| 心房颤动 | 无 | 0 | |
| 有 | 10 | ||
| 充血性心力 衰竭 | 无 | 0 | |
| 轻度 | 5 | ||
| 中度 | 10 | ||
| 重度 | 20 | ||
| 消化系统症状 | 无 | 0 | |
| 中度(腹泻/腹痛/恶心/呕吐) | 10 | ||
| 重度(黄疸) | 20 | ||
| 中枢神经系统症状 | 无 | 0 | |
| 轻度(烦躁不安) | 10 | ||
| 中度(谵妄/精神错乱/昏睡) | 20 | ||
| 重度(癫痫/昏迷) | 30 | ||
| 诱因状态 | 无 | 0 | |
| 有 | 10 | ||
| 总分 | ≥45:甲状腺危象 | ||
| 25~44:甲状腺危象前期 | |||
| <25:无甲状腺危象 | |||
Tab 5
Medications and dosages for the treatment of thyroid storm[1]
| 药物 | 剂量 | 评价 |
|---|---|---|
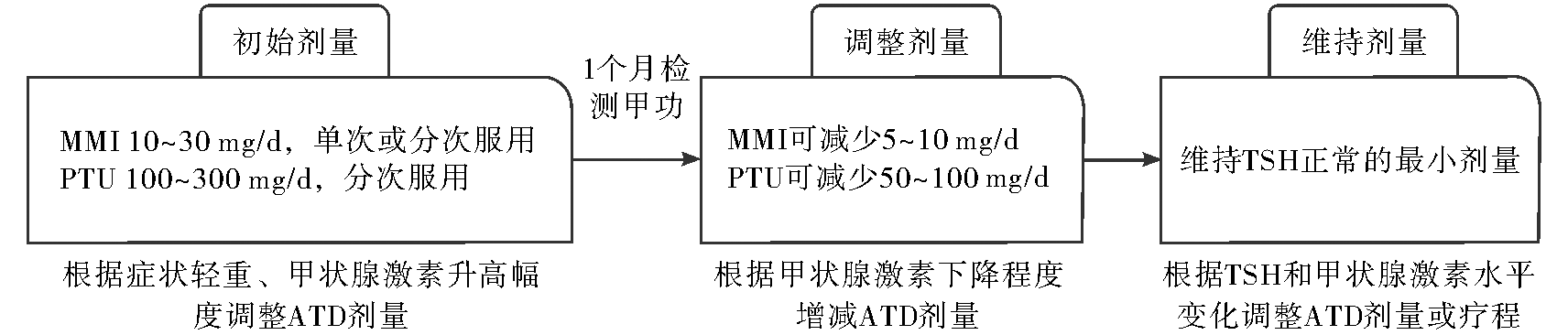
| 丙硫氧嘧啶 | 200~400 mg/6~8 h,口服 | 抑制激素合成 阻断外周T4向T3转换 |
| 甲巯咪唑 | 20~30 mg/6 h,口服 | 抑制新激素合成 |
| 普萘洛尔 | 60~80 mg/4~6 h, 口服 | 建议对充血性心力衰竭病人进行有创血流动力学监测 大剂量阻断外周T4向T3转化 替代药物:艾司洛尔静脉输注 |
| 碘[卢戈碘液(Lugol碘液)] | 4~8滴(20滴/mL, 8 mg碘/滴)/6~8 h,口服 | ATD应用1 h后开始服用 抑制新激素合成 抑制甲状腺激素释放 |
| 氢化可的松 | 500~100 mg/6~8 h,静脉滴注 | 可能阻断外周T4向T3转换 预防相对肾上腺功能不全 替代药物:地塞米松 |
| 地塞米松 | 2 mg/6~8 h,静脉 滴注 | 外周T4向T3转换 预防相对肾上腺功能不全 |

Fig 1
Principles of ATD administration and dose adjustment
Tab 6
Indications and contraindications for 131I treatment of GD
| 适应证 | 禁忌证 |
|---|---|
| ATD疗效差或多次复发 ATD过敏或出现其他治疗不良反应 有手术禁忌证或手术风险高 有颈部手术或外照射史 病程较长 老年病人(尤其伴发心血管疾病者) 合并肝功能损伤 合并白细胞或血小板减少 合并骨骼肌周期性瘫痪 合并心房颤动 计划半年后妊娠 | 妊娠期和哺乳期 确诊或可疑有甲状腺癌 |
Tab 7
Pre- and post-considerations for 131I treatment
| 阶段 | 注意事项 |
|---|---|
| 治疗前 | 131I治疗前1~2周应避免进食富碘食物和药物 |
| 治疗后 | 重症GD病人131I治疗3~7 d后可服用ATD以预防或减轻症状加重 |
| 辐射安全 | 行131I治疗的GD病人应遵循辐射安全注意事项,女性病人治疗后应避孕至少6个月,待甲状腺功能正常后再妊娠 |
| 复查 | 131I治疗后1~3个月复查。如病情较重,应根据需要密切随诊 |
| 再次治疗 | 131I治疗3个月后疗效不佳,或6个月后未完全缓解,可再次行131I治疗 |
| 转归 | GD自然转归或131I治疗后转归均可致甲状腺功能减退 |
Tab 8
Indications and contraindications for surgical treatment of GD
| 适应证 | 禁忌证 |
|---|---|
| 伴有压迫症状、胸骨后甲状腺肿、中度以上的原发性甲亢 内科规范治疗效果不佳 对ATD有严重不良反应 不愿或不宜行131I治疗或131I治疗效果不佳 合并甲状腺恶性肿瘤或原发性甲状旁腺功能亢进症 伴中重度GO,内科治疗效果不佳 病人有主观愿望要求手术以缩短疗程而迅速改善甲亢症状 | 全身情况差,如伴有严重心、肝、肾等器质性病变,或合并有恶性疾病终末期等消耗性疾病,不能耐受手术 妊娠早、晚期 |
Tab 9
Summary of recommendations in guidelines for surgical procedure selection, preoperative preparation, and postoperative management
| 阶段 | 处理意见 |
|---|---|
| 术式选择 | 首选全甲状腺切除或全甲状腺近全切除 |
| 手术应由具有丰富手术经验的外科医师实施 | |
| 术前准备 | 术前服用ATD,使甲状腺功能正常后再手术治疗 |
| 不耐受ATD或需短时间内手术时,可联合碘剂、β受体阻滞剂、地塞米松进行术前准备 | |
| 术前、术后常规口服补充钙剂、维生素D | |
| 术后管理 | 术后出血概率高于一般甲状腺手术,需立即积极处理 |
| 关注声带功能障碍的发生,及时请耳鼻喉科医师会诊 |
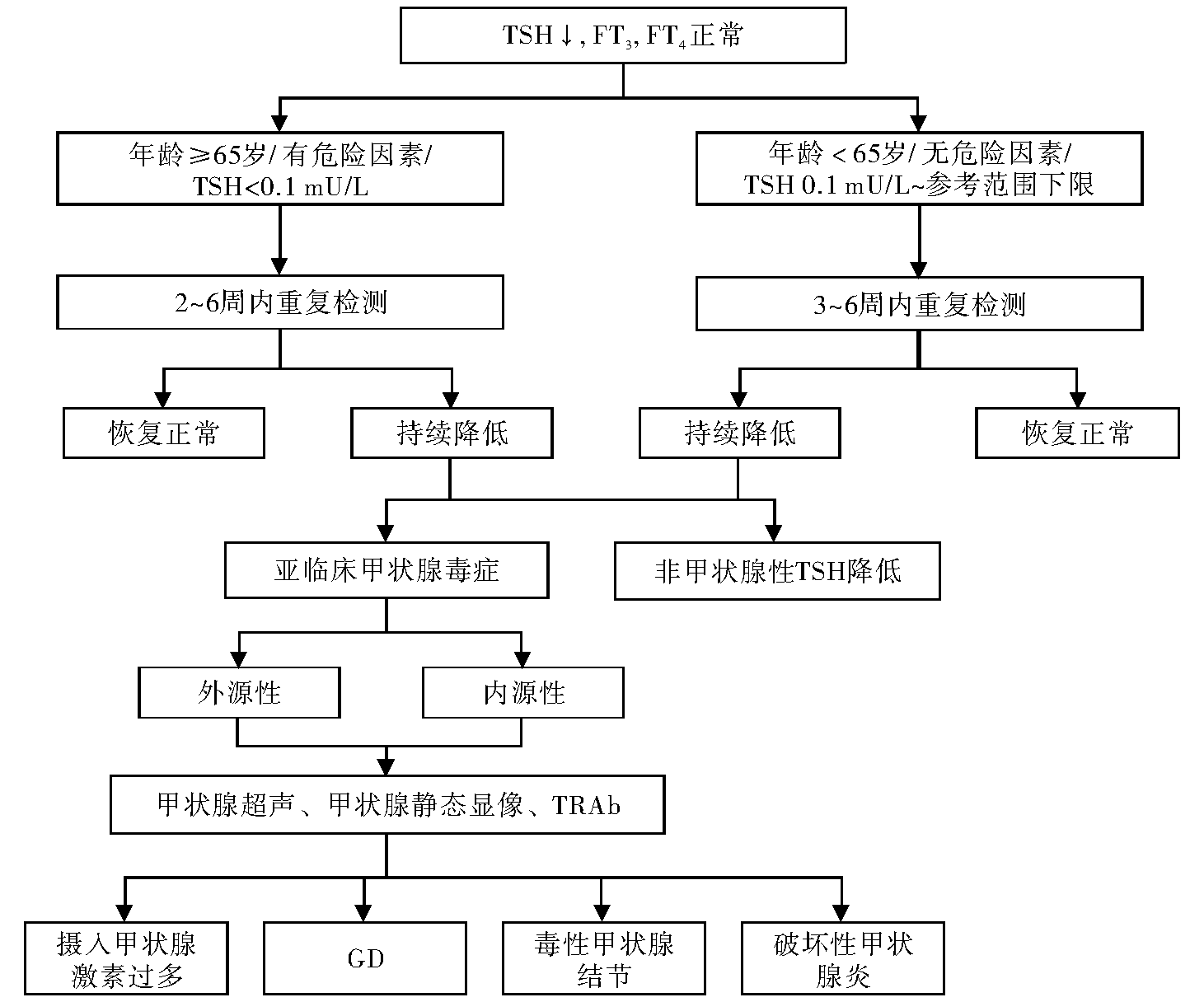
Fig 2
Flow chart of etiological diagnosis of subclinical thyrotoxicosis
Tab 10
Recommendations for the treatment of hyperthyroidism in GO patients
| GO分型 | 甲亢的治疗建议 |
|---|---|
| 轻度非活动性GO | 可选择ATD、手术或131I治疗 |
| 轻度活动性GO | 首选ATD或手术 如选择131I治疗,则应使用糖皮质激素预防GO进展 |
| 中、重度且长期非活动性GO | 可选择ATD、131I或手术治疗 选择131I治疗且存在危险因素(吸烟、高滴度TRAb),则应考虑糖皮质激素预防GO进展为活动性 |
| 中、重度活动性GO或GO威胁视力 | 使用ATD,必要时可手术,不建议131I治疗 |
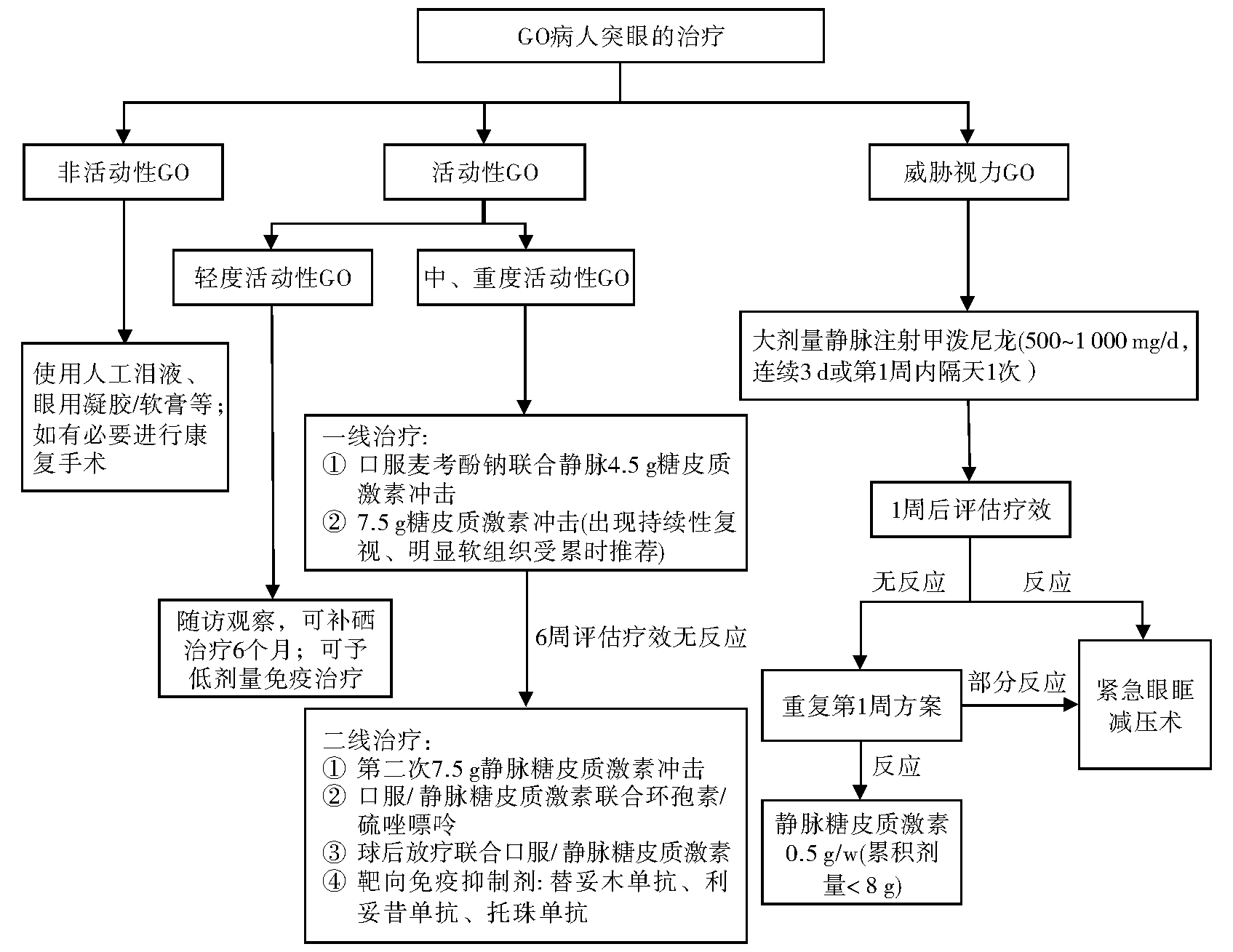
Fig 3
Flow chart of treatment for exophthalmia in GO patients
Tab 11
Recommendations for the management of thyrotoxicosis due to other causes
| 分类 | 处理建议 |
|---|---|
| 破坏性甲状腺炎 | 可使用β受体阻滞剂控制症状,不建议应用ATD 亚急性甲状腺炎根据病情可选择非甾体抗炎药(nonsteroidal antiinflammatory drug, NSAID)或糖皮质激素 |
| 分泌TSH的垂体腺瘤 | 需与甲状腺激素抵抗相鉴别 首选手术治疗 无法手术时,考虑放疗或药物治疗(生长抑素类似物和多巴胺受体激动剂) |
| 卵巢甲状腺肿 | 首选手术,疑似恶性肿瘤转移术后需131I治疗 |
| hCG相关甲状腺毒症 | ATD、β受体阻滞剂可有反应 葡萄胎首选清宫术,绒毛膜癌推荐化疗 |
| 人为甲状腺毒症 | 停用外源性甲状腺激素 严重者可能需血液净化或口服考来烯胺(消胆胺)治疗 |
| 功能性甲状腺癌转移 | 首选ATD控制后手术切除 不可切除时,序贯辅助131I治疗亦有效 疗效不佳时,可考虑分子靶向治疗 |
| 药源性甲状腺毒症 | 碘源性:避免继续碘暴露,使用β受体阻滞剂和(或)ATD 胺碘酮所致:1型应用ATD治疗;2型应用糖皮质激素治疗;分型不明确或单药治疗效果不佳者联合治疗 ICI:结合症状严重程度和免疫相关不良反应(immune-related adverse event, irAE)等级决定是否停药及给予干预药物 TKI、干扰素α、白细胞介素2和锂制剂:治疗前、后,监测甲状腺功能。如出现甲状腺毒症,应明确病因并行针对性治疗 |
| [1] | 中华医学会内分泌学分会, 中国医师协会内分泌代谢科医师分会, 中华医学会核医学分会, 等. 中国甲状腺功能亢进症和其他原因所致甲状腺毒症诊治指南[J]. 中华内分泌代谢杂志, 2022, 38(8):700-748. |
| Chinese Society of Endocrinology, Chinese Endocrinologist Association, Chinese Society of Nuclear Medicine, et al. Guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis[J]. Chin J Endocrinol Metab, 2022, 38(8):700-748. | |
| [2] |
AKAMIZU T, SATOH T, ISOZAKI O, et al. Diagnostic criteria, clinical features, and incidence of thyroid storm based on nationwide surveys[J]. Thyroid, 2012, 22(7):661-679.
doi: 10.1089/thy.2011.0334 pmid: 22690898 |
| [3] |
ANGELL T E, LECHNER M G, NGUYEN C T, et al. Clinical features and hospital outcomes in thyroid storm: a retrospective cohort study[J]. J Clin Endocrinol Metab, 2015, 100(2):451-459.
doi: 10.1210/jc.2014-2850 pmid: 25343237 |
| [4] |
LIU X, QIANG W, LIU X, et al. A second course of antithyroid drug therapy for recurrent Graves’ disease: an experience in endocrine practice[J]. Eur J Endocrinol, 2015, 172(3):321-326.
doi: 10.1530/EJE-14-0704 URL |
| [5] |
ROSS D S, BURCH H B, COOPER D S, et al. 2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis[J]. Thyroid, 2016, 26(10):1343-1421.
pmid: 27521067 |
| [6] |
BURCH H B, COOPER D S. Management of Graves di-sease: a review[J]. JAMA, 2015, 314(23):2544-2554.
doi: 10.1001/jama.2015.16535 URL |
| [7] |
ROSS D S. Radioiodine therapy for hyperthyroidism[J]. N Engl J Med, 2011, 364(6):542-550.
doi: 10.1056/NEJMct1007101 URL |
| [8] |
KANDIL E, MOHAMED S E, DENIWAR A, et al. Electrophysiologic identification and monitoring of the external branch of superior laryngeal nerve during thyroidectomy[J]. Laryngoscope, 2015, 125(8):1996-2000.
doi: 10.1002/lary.v125.8 URL |
| [9] |
GENCER B, COLLET T H, VIRGINI V, et al. Subclinical thyroid dysfunction and the risk of heart failure events: an individual participant data analysis from 6 prospective cohorts[J]. Circulation, 2012, 126(9):1040-1049.
pmid: 22821943 |
| [10] |
BLUM M R, BAUER D C, COLLET T H, et al. Subclinical thyroid dysfunction and fracture risk: a meta-analysis[J]. JAMA, 2015, 313(20):2055-2065.
doi: 10.1001/jama.2015.5161 pmid: 26010634 |
| [11] |
KALMIJN S, MEHTA K M, POLS H A, et al. Subclinical hyperthyroidism and the risk of dementia. The Rotterdam study[J]. Clin Endocrinol(Oxf), 2000, 53(6):733-737.
doi: 10.1046/j.1365-2265.2000.01146.x URL |
| [12] |
BARTLEY G B, GORMAN C A. Diagnostic criteria for Graves' ophthalmopathy[J]. Am J Ophthalmol, 1995, 119(6):792-795.
pmid: 7785696 |
| [13] |
BARTALENA L, KAHALY G J, BALDESCHI L, et al. The 2021 European Group on Graves' Orbitopathy (EUGOGO) clinical practice guidelines for the medical management of Graves' orbitopathy[J]. Eur J Endocrinol, 2021, 185(4):G43-G67.
doi: 10.1530/EJE-21-0479 pmid: 34297684 |
| [14] |
KAHALY G J. Imaging in thyroid-associated orbitopathy[J]. Eur J Endocrinol, 2001, 145(2):107-118.
doi: 10.1530/eje.0.1450107 pmid: 11454505 |
| [15] |
ANDERSEN S L, KNØSGAARD L. Management of thyrotoxicosis during pregnancy[J]. Best Pract Res Clin Endocrinol Metab, 2020, 34(4):101414.
doi: 10.1016/j.beem.2020.101414 URL |
| [16] |
DUNTAS L H. Thyroid function in aging: a discerning approach[J]. Rejuvenation Res, 2018, 21(1):22-28.
doi: 10.1089/rej.2017.1991 pmid: 28661207 |
| [1] | YAN Chao, LU Sheng, YAN Min, ZHU Zhenggang. Chinese interpretation of Japanese Gastric Cancer Treatment Guidelines 2021 (6th edition) and Ruijin clinical practice [J]. Journal of Surgery Concepts & Practice, 2023, 28(04): 326-354. |
| [2] | Chinese Society of Endocrinology,Chinese Medical Association , et al . Expert suggestions on the management of hyperthyroidism and hypothyroidism in the time of COVID-19 [J]. Journal of Diagnostics Concepts & Practice, 2022, 21(02): 128-129. |
| [3] | LI Fuxin, JIANG Ruoyu, LI Dongyang, CHEN Zuoyu, WEI Mingze, ZHANG Bai, HE Xianghui. Clinical analysis of primary hyperparathyroidism: a report of 138 cases [J]. Journal of Surgery Concepts & Practice, 2018, 23(02): 125-129. |
| [4] | . [J]. Journal of Internal Medicine Concepts & Practice, 2017, 12(04): 283-287. |
| [5] | . [J]. Journal of Internal Medicine Concepts & Practice, 2015, 10(06): 439-443. |
| [6] | . [J]. Journal of Surgery Concepts & Practice, 2005, 10(06): 519-521+524. |
| [7] | . [J]. Journal of Surgery Concepts & Practice, 2004, 9(06): 473-475. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||