Journal of Surgery Concepts & Practice ›› 2025, Vol. 30 ›› Issue (01): 54-60.doi: 10.16139/j.1007-9610.2025.01.10
• Original article • Previous Articles Next Articles
ZHANG Nannan1a, GUO Jinxing1a( ), WU Gang2, YI Hui1b, ZHOU Yuanhang1b, LIAO Zhiwei1b, HUANG Qi1b, DONG Jian1b
), WU Gang2, YI Hui1b, ZHOU Yuanhang1b, LIAO Zhiwei1b, HUANG Qi1b, DONG Jian1b
Received:2024-08-16
Online:2025-01-25
Published:2025-04-25
Contact:
GUO Jinxing
E-mail:guojinxing@hotmail.com
CLC Number:
ZHANG Nannan, GUO Jinxing, WU Gang, YI Hui, ZHOU Yuanhang, LIAO Zhiwei, HUANG Qi, DONG Jian. Establishment of an evaluation system for conversion to laparotomy in laparoscopic cholecystectomy and exploration of surgical grading management[J]. Journal of Surgery Concepts & Practice, 2025, 30(01): 54-60.
Tab 1
Univariate analysis between LC group and transfer laparotomy group [n(%)/ $\bar{x}±s$]
| Characteristic | LC group (n=9 246) | Transfer laparotomy group(n=168) | χ2 value | P value | |
|---|---|---|---|---|---|
| Gender: male | 4 186(45.3) | 69(41.1) | 1.176 | 0.278 | |
| Age ≥ 65 years | 2 192(23.7) | 41(24.4) | 0.044 | 0.833 | |
| BMI≥ 28 kg/m2 | 280(3.0) | 6(3.6) | 0.165 | 0.684 | |
| Diabetes | 325(3.5) | 10(6.0) | 2.856 | 0.091 | |
| History of upper abdominal surgery | 564(6.1) | 15(8.9) | 2.287 | 0.130 | |
| Body temperature≥38.5℃ | 1 524(16.5) | 105(62.5) | 244.173 | <0.001 | |
| Murphy sign positive | 2 775(30.0) | 110(65.5) | 97.634 | <0.001 | |
| Frequency of acute cholecystitis ≥3 times | 3 246(35.1) | 96(57.1) | 34.991 | <0.001 | |
| Duration of acute cholecystitis ≤72 h | 3 452(37.3) | 68(40.5) | 0.695 | 0.404 | |
| Total bilirubin ≥23 μmolL | 1 235(13.4) | 58(34.5) | 62.393 | <0.001 | |
| Maximum cross-section of gallbladder ≥5 cm×10 cm or ≤ 3 cm×4 cm | 1 975(21.4) | 32(19.0) | 0.526 | 0.468 | |
| Maximum thickness of gallbladder wall ≥5 mm | 1 885(20.4) | 72(42.9) | 50.593 | <0.001 | |
| Gallbladder neck stone incarceration | 1 025(11.1) | 60(35.7) | 98.149 | <0.001 | |
| Diameter of common bile duct ≥8 mm | 725(7.8) | 62(36.9) | 181.928 | <0.001 | |
| Surgical experience | ≤50 cases | 835(9.0) | 78(46.4) | 280.787 | <0.001 |
| 51-200 cases | 2 864(31.0) | 55(32.7) | |||
| >200 cases | 5 547(60.0) | 35(20.8) | |||
Tab 2
Statistical results of various factors in the Logistic regression model
| Characteristic | Regression coefficient | Wald χ2 | P value | OR | 95% CI | |
|---|---|---|---|---|---|---|
| Body temperature≥38.5℃ | 1.578 | 72.113 | <0.001 | 4.847 | 3.367-6.978 | |
| Frequency of acute cholecystitis ≥3 times | 0.754 | 19.266 | <0.001 | 2.125 | 1.518-2.976 | |
| Maximum thickness of gallbladder wall ≥5 mm | 1.195 | 46.175 | <0.001 | 3.305 | 2.341-4.666 | |
| Gallbladder neck stone incarceration | 1.667 | 76.388 | <0.001 | 5.297 | 3.645-7.698 | |
| Diameter of common bile duct ≥8 mm | 1.858 | 98.958 | <0.001 | 6.414 | 4.447-9.249 | |
| Surgical experience | ≤50 cases | 2.09 | 80.443 | <0.001 | 8.088 | 1.816-4.419 |
| 51-200 cases | 1.041 | 21.077 | <0.001 | 2.833 | 5.122-12.771 | |
Tab 3
Assigning values to each risk factor
| Evaluate project | Scores | |
|---|---|---|
| Body temperature≥38.5℃ | 1.5 | |
| Frequency of acute cholecystitis ≥3 times | 0.5 | |
| Maximum thickness of gallbladder wall ≥5 mm | 1 | |
| Gallbladder neck stone incarceration | 1.5 | |
| Diameter of common bile duct ≥8 mm | 2 | |
| Surgical experience | >200 cases | 0 |
| 51-200 cases | 1 | |
| ≤50 cases | 2 | |
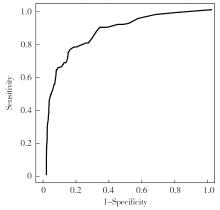
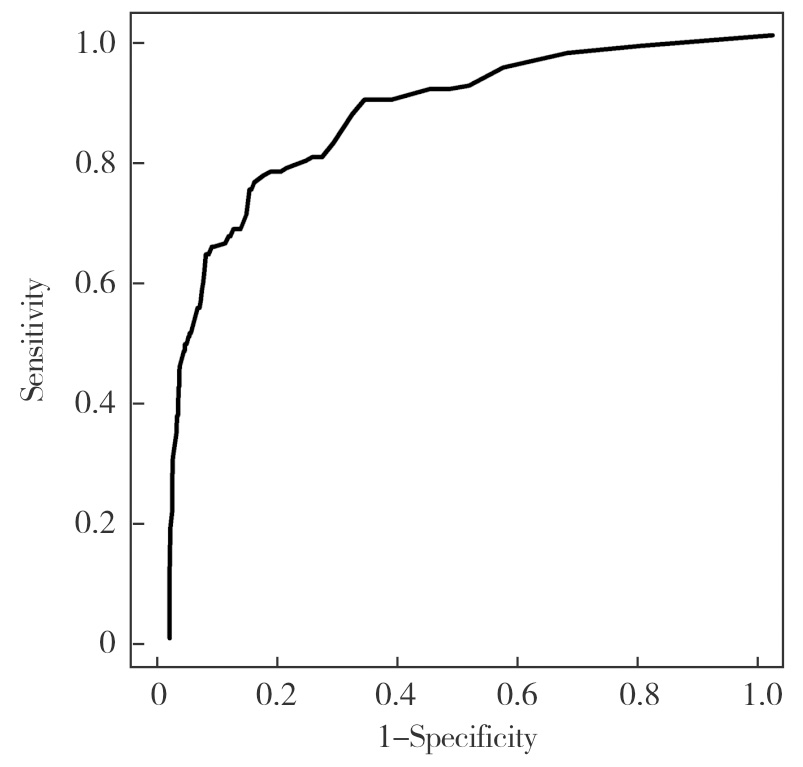
Fig 1
ROC curve of Logistic regression model
Tab 4
LC surgical grading management scale
Surgical experience Objective factor scale evaluation score: X | X>3 | 2<X≤3 | 1<X≤2 | X≤1 |
|---|---|---|---|---|
| ≤50 cases | high-risk | high-risk | high-risk | LC |
| 51-200 cases | high-risk | high-risk | LC | LC |
| >200 cases | high-risk | LC | LC | LC |
Tab 5
Comparison before and after grading management of LC surgery[n(%)]
| Item | Before use | After use | χ2 value | P value |
|---|---|---|---|---|
| LC cases | 9 414 | 620 | ||
| Direct laparotomy | 0 | 15 | ||
| Conversion to laparotomy | 168(1.78) | 4(0.65) | 4.482 | <0.05 |
| [1] |
LE V H, SMITH D E, JOHNSON B L. Conversion of laparoscopic to open cholecystectomy in the current era of laparoscopic surgery[J]. Am Surg, 2012, 78(12):1392-1395.
pmid: 23265130 |
| [2] | PHILIP ROTHMAN J, BURCHARTH J, POMMERGAARD H C, et al. Preoperative risk factors for conversion of laparoscopic cholecystectomy to open surgery-a systematic review and meta-analysis of observational studies[J]. Dig Surg, 2016, 33(5):414-423. |
| [3] |
HUSSAIN A. Difficult laparoscopic cholecystectomy: current evidence and strategies of management[J]. Surg Laparosc Endosc Percutan Tech, 2011, 21(4):211-217.
doi: 10.1097/SLE.0b013e318220f1b1 pmid: 21857467 |
| [4] | BOURGOUIN S, MANCINI J, MONCHAL T, et al. How to predict difficult laparoscopic cholecystectomy proposal for a simple preoperative scoring system[J]. Am J Surg, 2016, 212(5):873-881. |
| [5] | 陆昌友, 徐勇, 薛瑞丰, 等. 预防腹腔镜胆囊切除术中胆管损伤的单中心经验[J]. 肝胆外科杂志, 2022, 30(1):48-51. |
| LU C Y, XU Y, XUE R F, et al. Pereventing bile duct injury in laparoscopic cholecystectomy: single-center experience[J]. J Hepatobiliary Surgery, 2022, 30(1):48-51. | |
| [6] | INOUE K, UENO T, DOUCHI D, et al. Risk factors for difficulty of laparoscopic cholecystectomy in grade Ⅱ acute cholecystitis according to the Tokyo guidelines 2013[J]. BMC Surg, 2017, 17(1):114. |
| [7] | ABELSON J S, AFANEH C, RICH B S, et al. Advanced laparoscopic fellowship training decreases conversion rates during laparoscopic cholecystectomy for acute biliary diseases: a retrospective cohort study[J]. Int J Surg, 2015,13:221-226. |
| [8] | 彭腊玲, 刘琳, 卜春花, 等. 急症腹腔镜胆囊切除术中转开腹的预警模型构建与验证[J]. 腹腔镜外科杂志, 2022, 27(6):447-453. |
| PENG L L, LIU L, PIAO C H, et al. Construction and verification of an early warning model for switching to laparotomy during emergency laparoscopic cholecystectomy[J]. J Laparosc Surg, 2022, 27(6):447-453. | |
| [9] | 胡国治, 蔡国英, 郭永忠, 等. 508例急性胆囊炎行腹腔镜胆囊切除术的量化手术指征探讨[J]. 中国内镜杂志, 2007, 13(7):735-737. |
| HU G Z, CAI G Y, GUO Y Z, et al. Study in the quan-tiatative operative indication of laparoscopic cholesystectomy in acute cholesystitis[J]. China J Endosc, 2007, 13(7):735-737. | |
| [10] | JOSHI M R, BOHARA T P, RUPAKHETI S, et al. Pre-operative prediction of difficult laparoscopic cholecystectomy[J]. J Nepal Med Assoc, 2015, 53(200):221-226. |
| [11] | RAMAN J D, LIN Y K, SHARIAT S F, et al. Preoperative nomogram to predict the likelihood of complications after radical nephroureterectomy[J]. BJU Intern, 2017, 119(2):268-275. |
| [12] | 吴品飞, 刘杰凡, 顾勇劲, 等. 腹腔镜胆囊切除术中转开腹200例危险因素分析[J]. 肝胆胰外科杂志, 2016, 28(4):329-331. |
| WU P F, LIU J F, GU Y J, et al. Analysis of risk factors in 200 cases of laparoscopic cholecystectomy switching to laparotomy[J]. J Hepatopancreatobiliary Surg, 2016, 28(4):329-331. | |
| [13] | 仝仲凯, 郝志强, 王志斌. 急性结石性胆囊炎患者腹腔镜胆囊切除术中转开腹手术的影响因素分析[J]. 中国临床医生杂志, 2022, 50(12):1474-1476. |
| TONG Z K, HAO Z Q, WANG Z B. Analysis of factors influencing conversion to open surgery in laparoscopic cholecystectomy of patients with acute calculous cholecystitis[J]. Chin J Clin, 2022, 50(12):1474-1476. | |
| [14] |
AL MASRI S, SHAIB Y, EDELBI M, et al. Predicting conversion from laparoscopic to open cholecystectomy: a single institution retrospective study[J]. World J Surg, 2018, 42(8):2373-2382.
doi: 10.1007/s00268-018-4513-1 pmid: 29417247 |
| [15] | 邹细光, 朱芬如, 袁亚敏, 等. 急性结石性胆囊炎LC中转开腹影响因素分析[J]. 江西医药, 2022, 57(11):1832-1834. |
| ZOU X G, ZHU F R, YUAN Y M, et al. Analysis of inf-luencing factors of LC transition to laparotomy in acute calculous cholecystitis[J]. Jiangxi Med J, 2022, 57(11):1832-1834. | |
| [16] |
TOSUN A, HANCERLIOGULLARI K O, SERIFOGLU I, et al. Role of preoperative sonography in predicting conversion from laparoscopic cholecystectomy to open surgery[J]. Eur J Radiol, 2015, 84(3):346-349.
doi: S0720-048X(14)00574-9 pmid: 25579475 |
| [17] |
BEKSAC K, TURHAN N, KARAAGAOGLU E, et al. Risk factors for conversion of laparoscopic cholecystectomy to open surgery: a new predictive statistical model[J]. J Laparoendosc Adv Surg Tech A, 2016, 26(9):693-696.
doi: 10.1089/lap.2016.0008 pmid: 27385483 |
| [18] | JAMEEL S M, BAHADDIN M M, MOHAMMED A A. Grading operative findings at laparoscopic cholecystectomy following the new scoring system in Duhok governorate: cross sectional study[J]. Ann Med Surg (Lond), 2020, 23(60):266-270. |
| [19] | 董汉华, 武齐齐, 陈孝平. 急性胆道感染东京指南(2018版)更新解读[J]. 临床外科杂志, 2019, 27(1):5-9. |
| DONG H H, WU Q Q, CHEN X P. Tokyo guidelines for acute biliary tract infections (2018) updated interpretation[J]. J Clin Surg,2019, 27(1):5-9. | |
| [20] | 满高亚, 党同科, 吴清松. Rouviere沟引导胆囊后隧道解剖用于困难腹腔镜胆囊切除术[J]. 外科理论与实践, 2022, 27(3):239-243. |
| MAN G Y, DANG T K, WU Q S. Rouviere’s sulcus guided retro-gallbladder tunnel dissection in difficult laparoscopic cholecystectomy[J]. J Surg Concepts Pract, 2022, 27(3):239-243. |
| [1] | SONG Chunlin, LUO Chengjun, ZHU Yu. Risk factors analysis and predictive model construction for the failure of free flap transplantation in patients with traumatic soft tissue injury of limbs [J]. Journal of Tissue Engineering and Reconstructive Surgery, 2024, 20(3): 305-. |
| [2] | HUANG Junxian, CHEN Chun, CAO Yijia, QUAN Shaoli, WANG Yi. Distribution Network Fault Risk Assessment Method Considering Difference in Entropy Value of Rare Factors [J]. Journal of Shanghai Jiao Tong University, 2024, 58(12): 1857-1867. |
| [3] | WU Xinwan, LI Xiang, ZHENG Minjia, YAO Junyan. Risk factors of postoperative delirium in elderly patients undergoing noncardiac surgery under general anesthesia [J]. Journal of Surgery Concepts & Practice, 2024, 29(06): 510-517. |
| [4] | XU Huimin, GAO Hongxia. Management of in-stent restenosis after iliofemoral venous stenting [J]. Journal of Surgery Concepts & Practice, 2024, 29(06): 481-486. |
| [5] | LI Jianwen, ZHANG Yun, YUE Fei. Abdominal wall functional reconstruction in laparoscopic ventral and incisional hernia repair [J]. Journal of Surgery Concepts & Practice, 2024, 29(04): 285-291. |
| [6] | HAN Haifeng, LU Jinghui. Treatment of primary abdominal wall tumors via minimally invasive surgery [J]. Journal of Surgery Concepts & Practice, 2024, 29(04): 311-315. |
| [7] | ZHANG Yizhong, TANG Rui, WANG Tingfeng, SI Xianke, YE Lebin, LIU Nan, XIANG Shijun, WU Weidong. Lateral approach single-incision laparoscopic totally extraperitoneal inguinal hernia repair: a report of 110 cases [J]. Journal of Surgery Concepts & Practice, 2024, 29(04): 323-328. |
| [8] | LU Zhiyu, SUN Ji, DU Jialu, MENG Xuan, LUO Man, LIU Yue, WANG Hongguang. Research on the management of the Glissonean pedicle in laparoscopic anatomical hemihepatectomy and the influence of indocyanine green dose on the fluorescence staining effect [J]. Journal of Surgery Concepts & Practice, 2024, 29(02): 138-142. |
| [9] | SHAO Xinlin, ZHU Xuemei, CAO Hua. Advances in research on the risk factors and pathogenesis of connective tissue disease-associated interstitial lung disease [J]. Journal of Diagnostics Concepts & Practice, 2024, 23(02): 202-209. |
| [10] | ZHAN Chongwen, SHEN Qiwei, SHAO Yikai, XU Bo, HUA Rong, YAO Qiyuan. Efficacy of three-port laparoscopic sleeve gastrectomy in treatment of obesity [J]. Journal of Surgery Concepts & Practice, 2023, 28(05): 463-468. |
| [11] | NIE Haihang, WANG Fan, WANG Hongling, ZHAO Qiu. Risk factors and prevention methods for post-ERCP pancreatitis [J]. Journal of Surgery Concepts & Practice, 2023, 28(04): 310-315. |
| [12] | LI Lei, WU Xi, DAI Jing, WU Wenman, DING Qiulan, WANG Xuefeng. Clinical characteristics and risk factor analysis of 118 patients with cerebral venous sinus thrombosis [J]. Journal of Diagnostics Concepts & Practice, 2023, 22(03): 261-269. |
| [13] | LUO Yang, ZHONG Ming. Prevention and treatment of anastomotic leakage after laparoscopic anterior resection of low rectal cancer [J]. Journal of Surgery Concepts & Practice, 2023, 28(03): 220-225. |
| [14] | ZHENG Minhua, MA Junjun. Laparoscopic colorectal surgery 30 years in China: what we learned [J]. Journal of Surgery Concepts & Practice, 2023, 28(03): 181-185. |
| [15] | LUO Yang, YU Minhao, YE Guangyao, LIN Haiping, GONG Tingyue, LI Hao, ZHONG Ming. Efficacy of intraoperative indocyanine green fluorescence imaging evaluation for preventing anastomotic leakage after laparoscopic rectal cancer surgery [J]. Journal of Surgery Concepts & Practice, 2023, 28(03): 249-253. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||