诊断学理论与实践 ›› 2019, Vol. 18 ›› Issue (1): 44-50.doi: 10.16150/j.1671-2870.2019.01.009
侯亚楠1, 禤立平1, 赵志云1, 李勉1, 陈宇红1, 戴蒙1, 徐敏1, 毕宇芳1, 王卫庆1, 高金丽2( )
)
收稿日期:2018-09-30
出版日期:2019-02-25
发布日期:2019-02-25
通讯作者:
高金丽
E-mail:390795950@qq.com
基金资助:
HOU Yanan1, XUAN Liping1, ZHAO Zhiyun1, LI Mian1, CHEN Yuhong1, DAI Meng1, XU Min1, BI Yufang1, WANG Weiqing1, GAO Jinli2()
Received:2018-09-30
Online:2019-02-25
Published:2019-02-25
Contact:
GAO Jinli
E-mail:390795950@qq.com
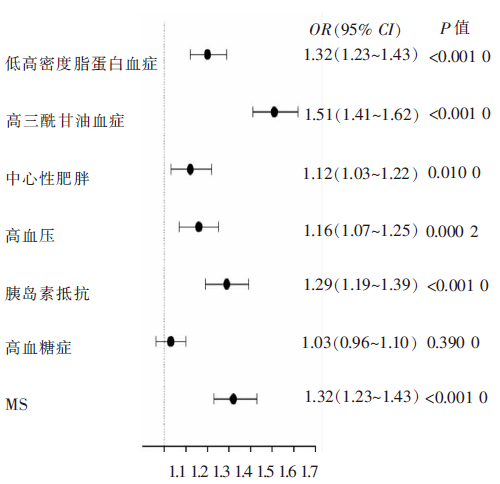
摘要: 目的 探讨上海市嘉定区中老年人群血尿酸/肌酐比值(uric acid to creatinine ratio, UA/Cr)与代谢综合征(metabolic syndrome,MS)间关联性的流行病学趋势。方法 采取整群抽样的方法,对2014年上海市嘉定区6 570名40岁以上居民进行标准化问卷调查、体格检查、生化检测等。根据国际糖尿病联盟的标准定义MS。按照UA/Cr四分位数分组,采用多因素logistic回归模型,分析UA/Cr与MS间相关性,以明确UA/Cr是否可作为MS的独立风险因素。结果 本研究纳入6 414 名研究对象,其中MS患者3 313例(52.7%)。血Cr水平为77(70~87) mmol/L,血UA水平为314(267~372) mmol/L,UA/Cr水平为4.01(3.46~4.65)。根据UA/Cr四分位数将研究人群分为4组,第1组UA/Cr <1.0,第2组1.0≤UA/Cr<1.5,第3组1.5≤UA/Cr<2.0,第4组UA/Cr≥2.0。从第1组到第4组,随着UA/Cr水平的增加,受试者的体质量指数(body mass index, BMI)、腰围、血压、三酰甘油、低密度脂蛋白胆固醇、总胆固醇、C反应蛋白及胰岛素抵抗水平逐渐增加(P<0.01);MS及其组分的患病率也呈现显著增加的趋势(P<0.01)。logistic回归分析显示,UA/Cr水平与MS、高血压病、中心性肥胖、高三酰甘油血症、低高密度脂蛋白血症及胰岛素抵抗呈正相关性,以第1组作为参照,第2、3、4组MS患病风险OR值及95%CI分别为1.15(0.96~1.38)、1.36(1.14~1.64)、1.96(1.62~2.37);高血压病为1.04(0.86~1.25)、1.22(1.01~1.48)、1.33(1.09~1.62);中心性肥胖为1.06(0.86~1.31)、1.26(1.02~1.56)、1.33(1.09~1.62);高三酰甘油血症为1.29(1.08~1.54)、1.74(1.46~2.07)、2.81(2.35~3.36);低高密度脂蛋白血症为0.93(0.77~1.13)、1.35(1.12~1.61)、1.50(1.25~1.80);胰岛素抵抗为0.96(0.77~1.19)、1.14(0.92~1.40)、1.81(1.48~2.22)(均P趋势<0.01)。结论 社区中老年人群UA/Cr 与MS患病间呈独立正相关,UA/Cr可作为MS的早期生物标志物,为MS的早期发现、高危人群的干预及心血管疾病的逆转提供新的科学依据。
中图分类号:
侯亚楠, 禤立平, 赵志云, 李勉, 陈宇红, 戴蒙, 徐敏, 毕宇芳, 王卫庆, 高金丽. 上海社区中老年人群血尿酸/肌酐比值与代谢综合征关联性的流行病学调查[J]. 诊断学理论与实践, 2019, 18(1): 44-50.
HOU Yanan, XUAN Liping, ZHAO Zhiyun, LI Mian, CHEN Yuhong, DAI Meng, XU Min, BI Yufang, WANG Weiqing, GAO Jinli. Epidemiological study on association of uric acid to creatinine ratio with metabolic syndrome in middle-aged and elderly populationin Shanghai[J]. Journal of Diagnostics Concepts & Practice, 2019, 18(1): 44-50.
表1
按UA/Cr比值四分位分组人群基本特征
| 参数 | 组分1 | 组分2 | 组分3 | 组分4 | P值 |
|---|---|---|---|---|---|
| 例数 | 1 603 | 1 604 | 1 604 | 1 603 | / |
| 年龄(岁) | 62.6±9.2 | 62.2±8.7 | 62.2±8.6 | 62.1±8.6 | 0.230 0 |
| BMI(kg/m2) | 23.9±3.5 | 24.6±3.3 | 25.2±3.4 | 26.0±3.6 | <0.000 1 |
| 腰围(cm) | 81.1±10.2 | 82.6±10.1 | 84.3±9.6 | 86.5±10.3 | <0.000 1 |
| 收缩压(mmHg) | 133.9±18.1 | 139.9±17.7 | 135.0±16.5 | 136.2±16.8 | 0.000 3 |
| 舒张压(mmHg) | 75.6±9.7 | 75.8±9.7 | 76.7±9.3 | 77.1±9.6 | <0.000 1 |
| 空腹血糖(mmol/L) | 6.21±1.71 | 6.10±1.43 | 6.08±1.37 | 6.17±1.33 | 0.040 0 |
| 胰岛素抵抗指数 | 1.60(1.10~2.40) | 1.74(1.21~2.58) | 1.93(1.32~2.81) | 2.32(1.57~3.43) | <0.000 1 |
| TG(mmol/L) | 1.27(0.96~1.76) | 1.44(1.08~1.96) | 1.55 1.14~2.16) | 1.87(1.31~2.69) | <0.000 1 |
| LDL-C(mmol/L) | 3.51±0.79 | 3.60±0.76 | 3.60±0.77 | 3.69±0.84 | <0.000 1 |
| HDL-C(mmol/L) | 1.39±0.33 | 1.35±0.30 | 1.32±0.30 | 1.29±0.28 | <0.000 1 |
| TC(mmol/L) | 5.17±0.99 | 5.25±0.95 | 5.27±0.98 | 5.41±1.12 | <0.000 1 |
| C反应蛋白(mg/L) | 0.19(0.14~0.28) | 0.21(0.16~0.30) | 0.23(0.17~0.34) | 0.26(0.19~0.40) | <0.000 1 |
| 饮食因素(食用频率×食用量) | 32.3±17.6 | 33.3±19.6 | 32.6±16.8 | 32.5±16.5 | 0.450 0 |
| MS[n(%)] | 624(38.9) | 744(46.4) | 876(54.1) | 1069(66.7) | <0.000 1 |
| 高血压病[n(%)] | 1058(66.0) | 1082(67.5) | 1171(73.0) | 1228(76.6) | <0.000 1 |
| 高三酰甘油血症[n(%)] | 452(28.2) | 579(36.1) | 688(42.9) | 927(57.8) | <0.000 1 |
| 低高密度脂蛋白血症[n(%)] | 432(27.0) | 457(28.5) | 587(36.6) | 648(40.4) | <0.000 1 |
| 高血糖症[n(%)] | 938(58.5) | 951(59.3) | 954(59.5) | 1061(66.2) | <0.000 1 |
| 中心性肥胖[n(%)] | 622(38.8) | 725(45.2) | 881(54.9) | 993(62.0) | <0.000 1 |
| 体力活动(MET-h/wk) | 16.8(3.0~21.0) | 15.0(4.5~21.0) | 18.0(4.5~21.0) | 15.0(3.0~21.0) | 0.220 0 |
| 目前吸烟[n(%)] | 314(19.6) | 321(20.0) | 300(18.7) | 297(18.5) | 0.670 0 |
| 目前饮酒[n(%)] | 181(11.3) | 212(13.2) | 221(13.8) | 292(18.2) | <0.000 1 |
表2
UA/Cr比值与MS危险因素及代谢指标的相关性分析
| 参数 | β±SE② | P值 |
|---|---|---|
| 腰围(cm) | 2.15±0.15 | <0.000 1 |
| BMI(kg/m2) | 0.82±0.05 | <0.000 1 |
| 收缩压(mmHg) | 1.17±0.27 | <0.000 1 |
| 舒张压(mmHg) | 0.71±0.14 | <0.000 1 |
| 空腹血糖(mmol/L) | -0.006±0.02 | 0.790 0 |
| 胰岛素抵抗指数① | 0.06±0.004 | <0.000 1 |
| TG①(mmol/L) | 0.06±0.003 | <0.000 1 |
| HDL-C(mmol/L) | -0.04±0.004 | <0.000 1 |
| LDL-C(mmol/L) | 0.05±0.01 | <0.000 1 |
| TC(mmol/L) | 0.08±0.02 | <0.000 1 |
| C反应蛋白①(mg/L) | 0.05±0.004 | <0.000 1 |
表3
UA/Cr比值四分位数分组后与MS的相关性
| 模型 | OR(95% CI) | 趋势P值 | |||
|---|---|---|---|---|---|
| 组分 1 | 组分2 | 组分3 | 组分4 | ||
| MS | |||||
| 模型1 | 1.00 | 1.36(1.18~1.56) | 1.89(1.64~2.17) | 3.14(2.72~3.63) | <0.000 1 |
| 模型2 | 1.00 | 1.18(0.98~1.41) | 1.44(1.20~1.73) | 2.11(1.75~2.54) | <0.000 1 |
| 模型3 | 1.00 | 1.15(0.96~1.38) | 1.36(1.14~1.64) | 1.96(1.62~2.37) | <0.000 1 |
| 高血压病 | |||||
| 模型1 | 1.00 | 1.07(0.92~1.24) | 1.39(1.20~1.62) | 1.69(1.44~1.97) | <0.000 1 |
| 模型2 | 1.00 | 1.04(0.87~1.25) | 1.24(1.03~1.50) | 1.36(1.12~1.65) | <0.000 1 |
| 模型3 | 1.00 | 1.04(0.86~1.25) | 1.22(1.01~1.48) | 1.33(1.09~1.62) | <0.000 1 |
| 高血糖症 | |||||
| 模型1 | 1.00 | 1.03(0.90~1.19) | 1.04(0.90~1.20) | 1.39(1.20~1.60) | <0.000 1 |
| 模型2 | 1.00 | 1.05(0.89~1.24) | 0.94(0.80~1.12) | 1.22(1.02~1.45) | 0.100 0 |
| 模型3 | 1.00 | 1.03(0.87~1.22) | 0.90(0.76~1.07) | 1.15(0.96~1.37) | 0.360 0 |
| 中心性肥胖 | |||||
| 模型1 | 1.00 | 1.30(1.13~1.50) | 1.92(1.67~2.21) | 2.57(2.23~2.96) | <0.000 1 |
| 模型2 | 1.00 | 1.08(0.88~1.38) | 1.32(1.06~1.63) | 1.40(1.12~1.74) | 0.006 0 |
| 模型3 | 1.00 | 1.06(0.86~1.31) | 1.26(1.02~1.56) | 1.32(1.06~1.65) | 0.004 0 |
| 低高密度脂蛋白血症 | |||||
| 模型1 | 1.00 | 1.08(0.93~1.26) | 1.56(1.35~1.82) | 1.84(1.59~2.13) | <0.000 1 |
| 模型2 | 1.00 | 1.08(0.88~1.34) | 1.32(1.06~1.63) | 1.40(1.12~1.74) | <0.000 1 |
| 模型3 | 1.00 | 0.93(0.77~1.13) | 1.35(1.12~1.61) | 1.50(1.25~1.80) | <0.000 1 |
| 高三酰甘油血症 | |||||
| 模型1 | 1.00 | 1.44(1.24~1.67) | 1.91(1.65~2.22) | 3.49(3.01~4.05) | <0.000 1 |
| 模型2 | 1.00 | 1.31(1.10~1.56) | 1.80(1.51~2.14) | 2.95(2.48~3.53) | <0.000 1 |
| 模型3 | 1.00 | 1.29(1.08~1.54) | 1.74(1.46~2.07) | 2.81(2.35~3.36) | <0.000 1 |
| 胰岛素抵抗 | |||||
| 模型1 | 1.00 | 1.08(0.91~1.29) | 1.46(1.23~1.73) | 2.70(2.30~3.17) | <0.000 1 |
| 模型2 | 1.00 | 0.98(0.79~1.21) | 1.19(0.97~1.47) | 1.95(1.59~2.39) | <0.000 1 |
| 模型3 | 1.00 | 0.96(0.77~1.19) | 1.14(0.92~1.40) | 1.81(1.48~2.22) | <0.000 1 |
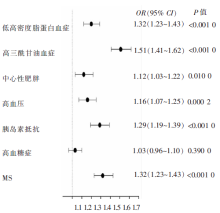
图1
UA/Cr比值与MS的相关性
| [1] | Grundy SM, Cleeman JI, Daniels SR, et al. Diagnosis and management of the metabolic syndrome: an American Heart Association/National Heart, Lung, and Blood Institute scientific statement: Executive Summary[J]. Crit Pathw Cardiol, 2005, 4(4):198-203. |
| [2] | Nejatinamini S, Ataie-Jafari A, Qorbani M, et al. Asso-ciation between serum uric acid level and metabolic syndrome components[J]. J Diabetes Metab Disord, 2015, 14:70. |
| [3] | Fu CC, Wu DA, Wang JH, et al. Association of C-reactive protein and hyperuricemia with diabetic nephropathy in Chinese type 2 diabetic patients[J]. Acta Diabetol, 2009, 46(2):127-134. |
| [4] | Guo L, Cheng Y, Wang X, et al. Association between microalbuminuria and cardiovascular disease in type 2 diabetes mellitus of the Beijing Han nationality[J]. Acta Diabetol, 2012, 49(Suppl 1):S65-S71. |
| [5] | Mankovsky B, Kurashvili R, Sadikot. Is serum uric acid a risk factor for atherosclerotic cardiovascular disease? A review of theclinical evidence. Part 1. Diabetes & Metabolic Syndrome: Clinical Research & Reviews 4, 2010:176-184. |
| [6] | Gersch C, Palii SP, Kim KM, et al. Inactivation of nitric oxide by uric acid[J]. Nucleosides Nucleotides Nucleic Acids, 2008, 27(8):967-978. |
| [7] | Norvik JV, Storhaug HM, Ytrehus K, et al. Overweight modifies the longitudinal association between uric acid and some components of the metabolic syndrome: The Tromsø Study[J]. BMC Cardiovasc Disord, 2016, 16:85. |
| [8] | Culleton BF, Larson MG, Evans JC, et al. Prevalence and correlates of elevated serum creatinine levels: the Framin-gham Heart Study[J]. Arch Intern Med, 1999, 159(15):1785-1790. |
| [9] | Coresh J, Wei GL, McQuillan G, et al. Prevalence of high blood pressure and elevated serum creatinine level in the United States: findings from the third National Health and Nutrition Examination Survey(1988-1994)[J]. Arch Intern Med, 2001, 161(9):1207-1216. |
| [10] | Muntner P, He J, Hamm L, et al. Renal insufficiency and subsequent death resulting from cardiovascular disease in the United States[J]. J Am Soc Nephrol, 2002, 13(3):745-753. |
| [11] | Al-Daghri NM, Al-Attas OS, Wani K, et al. Serum Uric Acid to Creatinine Ratio and Risk of Metabolic Syndrome in Saudi Type 2 Diabetic Patients[J]. Sci Rep, 2017, 7(1):12104. |
| [12] | Kim ES, Kwon HS, Ahn CW, et al. Serum uric acid level is associated with metabolic syndrome and microalbumi-nuria in Korean patients with type 2 diabetes mellitus[J]. J Diabetes Complications, 2011, 25(5):309-313. |
| [13] | Sah SK, Khatiwada S, Pandey S, et al. Association of high-sensitivity C-reactive protein and uric acid with the metabolic syndrome components[J]. Springerplus, 2016, 5:269. |
| [14] | Gu L, Huang L, Wu H, et al, R. Serum uric acid to creatinine ratio: A predictor of incident chronic kidney disea-se in type 2 diabetes mellitus patients with preserved kidney function[J]. Diab Vasc Dis Res, 2017, 14(3):221-225. |
| [15] | Vincent MA, Barrett EJ, Lindner JR, et al. Inhibiting NOS blocks microvascular recruitment and blunts muscle glucose uptake in response to insulin[J]. Am J Physiol Endocrinol Metab, 2003, 285(1):E123-E129. |
| [16] | Heinig M, Johnson RJ. Role of uric acid in hypertension, renal disease, and metabolic syndrome[J]. Cleve Clin J Med, 2006, 73(12):1059-1064. |
| [17] | Kaur J. A comprehensive review on metabolic syndrome[J]. Cardiol Res Pract, 2014, 2014:943162. |
| [18] | Kawamoto R, Tabara Y, Kohara K, et al. Usefulness of combining serum uric acid and high-sensitivity C-reactive protein for risk stratification of patients with metabolic syndrome in community-dwelling women[J]. Endocrine, 2013, 44(1):132-139. |
| [19] | Krishnan E, Kwoh CK, Schumacher HR, et al. Hyperu-ricemia and incidence of hypertension among men without metabolic syndrome[J]. Hypertension, 2007, 49(2):298-303. |
| [20] | Matsuura F, Yamashita S, Nakamura T, et al. Effect of visceral fat accumulation on uric acid metabolism in male obese subjects: visceral fat obesity is linked more closely to overproduction of uric acid than subcutaneous fat obesity[J]. Metabolism, 1998, 47(8):929-933. |
| [21] | Schmidt MI, Watson RL, Duncan BB, et al. Clustering of dyslipidemia, hyperuricemia, diabetes, and hypertension and its association with fasting insulin and central and overall obesity in a general population. Atherosclerosis Risk in Communities Study Investigators[J]. Metabolism, 1996, 45(6):699-706. |
| [22] | Eräranta A, Kurra V, Tahvanainen AM, et al. Oxonic acid-induced hyperuricemia elevates plasma aldosterone in experimental renal insufficiency[J]. J Hypertens, 2008, 26(8):1661-1668. |
| [23] | Feig DI, Kang DH, Johnson RJ. Uric acid and cardiovascular risk[J]. N Engl J Med, 2008, 359(17):1811-1821. |
| [24] | Facchini F, Chen YD, Hollenbeck CB, et al. Relationship between resistance to insulin-mediated glucose uptake, urinary uric acid clearance, and plasma uric acid concentration[J]. JAMA, 1991, 266(21):3008-3011. |
| [1] | 吴雪妍, 马丽娜, 程棣, 杜瑞, 徐瑜, 徐敏, 陆洁莉, 陈宇红, 毕宇芳, 王卫庆, 高金丽, 钱晓忠. 上海市宝山区淞南社区中老年人群静息心率与糖尿病相关性的流行病学调查[J]. 诊断学理论与实践, 2018, 17(01): 45-50. |
| [2] | 施琰, 高金丽, 黄小琳, 彭魁, 徐敏, 毕宇芳, 倪衡如,. 上海市社区中老年人代谢综合征与糖尿病发病风险相关性的研究[J]. 诊断学理论与实践, 2016, 15(04): 354-359. |
| [3] | 周嘉, 罗悦玲, 李励, 冼晶, 梁杏欢, 黄振兴, 秦映芬, 罗佐杰,. 广西40岁以上人群代谢综合征及其危险因素调查[J]. 诊断学理论与实践, 2016, 15(04): 364-370. |
| [4] | 谷晓岚, 魏雪, 牛敏, 罗兰, 李欣宇, 高政南,. 大连地区中老年人群中颈围与高血压的相关性研究[J]. 诊断学理论与实践, 2016, 15(04): 371-375. |
| [5] | 毕夫景, 赵咏桔,. 老年人群高尿酸血症相关因素分析及其与代谢综合征的关系[J]. 诊断学理论与实践, 2010, 9(03): 255-259. |
| [6] | 曲伸, 刘蒙, 高鑫,. 胰岛素抵抗与非酒精性脂肪性肝病关系的认识[J]. 诊断学理论与实践, 2009, 8(03): 240-243. |
| [7] | 祝之明,. 胰岛素抵抗综合征与代谢综合征的异同及临床意义[J]. 诊断学理论与实践, 2009, 8(03): 244-247. |
| [8] | 沈琳辉, 崔斌, 赵咏桔, 颜美珠, 林云, 巩云霞, 吴方,. 老年男性雄激素受体基因CAG重复序列长度多态性与代谢综合征的关系[J]. 诊断学理论与实践, 2007, 6(05): 412-416. |
| [9] | 蔡晓波, 范建高, 朱军, 李新建, 李锐, 戴菲,. 成人不明原因丙氨酸转氨酶升高危险因素分析[J]. 诊断学理论与实践, 2007, 6(04): 331-334. |
| [10] | 祝之明,. 代谢综合征心血管损害标志的临床评估[J]. 诊断学理论与实践, 2007, 6(02): 93-96. |
| [11] | 张丽霞,. 代谢综合征与糖尿病和心血管疾病[J]. 诊断学理论与实践, 2007, 6(02): 172-174. |
| [12] | 蒋利, 周林, 钟健, 闫振成, 倪银星, 陈静, 祝之明,. 糖脂代谢紊乱对女性代谢综合征患者左室结构与功能的影响[J]. 诊断学理论与实践, 2007, 6(02): 119-122. |
| [13] | 范建高,. 脂肪肝促发代谢紊乱和动脉硬化的机制[J]. 诊断学理论与实践, 2007, 6(02): 108-110. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||