诊断学理论与实践 ›› 2020, Vol. 19 ›› Issue (02): 115-121.doi: 10.16150/j.1671-2870.2020.02.004
肖超, 陶英, 宋陆茜, 赵佑山, 吴凌云, 常春康( )
)
收稿日期:2019-02-27
出版日期:2020-04-25
发布日期:2020-04-25
通讯作者:
常春康
E-mail:changchunkang@sina.com
XIAO Chao, TAO Ying, SONG Luxi, ZHAO Youshan, WU Lingyun, CHANG Chunkang()
Received:2019-02-27
Online:2020-04-25
Published:2020-04-25
Contact:
CHANG Chunkang
E-mail:changchunkang@sina.com
摘要:
目的:分析88例骨髓增殖性疾病(myeloproliferative neoplasm,MPN)患者的临床资料,比较原发性骨髓纤维化前期(prefibrotic primary myelofibrosis,pre-PMF)与明显的原发性骨髓纤维化(overt-primary myelofibrosis,overt-PMF)、原发性血小板增多症(essential thrombocythemia,ET)患者的临床表现区别。方法:收集我院2015年1月至2018年1月连续诊断的88例MPN患者的临床相关参数(包括诊断分型、血常规检测结果、脾肿大状况、骨髓巨核细胞数和纤维化程度、相关基因突变等),进行比较分析。结果:连续纳入88例MPN患者的中位年龄为61岁(20~88岁),有32例(36%)为≥65岁的老年人, 46例(52%)为男性,22例(25%)出现脾肿大;检出JAK2 V617F突变者为51例(58%),CALR突变者为5例(6%),MPL突变者为2例(2%),三阴性者为30例(34%)。88例患者分型诊断为真性红细胞增多症(polycythemia vera,PV)者共20例;ET为23例;PMF共45例,其中pre-PMF为23例(占PMF的51%),overt-PMF为22例(占49%)。在overt-PMF患者中,CALR基因突变阳性率高达18%(4/22)。pre-PMF患者的临床症状比overt-PMF患者轻,其出现血红蛋白含量和血小板计数低下的比例及平均乳酸脱氢酶水平均比overt-PMF患者低(P 值分别为0.048、0.034、0.037)。pre-PMF患者与ET患者的临床表现相似,而pre-PMF患者中出现脾肿大的百分比及白细胞增多的百分比高于ET患者(26%比4%,61%比17%,P值为0.043和0.007),且随访发现,ET患者的中位生存时间比pre-PMF患者长(前者未达,后者为94个月,P=0.038)。在pre-PMF中,三阴性患者又比JAK2突变患者的中位年龄小(59岁比62岁,P=0.030)、发生脾肿大例数多(4例比2例,P=0.017)。结论:MPN是一组异质性克隆性血液系统疾病。pre-PMF与overt-PMF患者呈现出不同的临床表现和预后,区分两者很有必要。pre-PMF与ET的临床表现相似,但预后不同,ET预后较好,通过组织形态学诊断结合次要临床标准来区分两者极为重要。
中图分类号:
肖超, 陶英, 宋陆茜, 赵佑山, 吴凌云, 常春康. 88例骨髓增殖性疾病患者的临床资料分析[J]. 诊断学理论与实践, 2020, 19(02): 115-121.
XIAO Chao, TAO Ying, SONG Luxi, ZHAO Youshan, WU Lingyun, CHANG Chunkang. Clinical analysis of 88 patients with myeloproliferative neoplasm[J]. Journal of Diagnostics Concepts & Practice, 2020, 19(02): 115-121.
表1
88例患者的临床特点[n(%),中位数(范围)]
| 参数 | PV(n=20) | ET(n=23) | pre-PMF(n=23) | overt-PMF(n=22) | P值 |
|---|---|---|---|---|---|
| 性别(男/女) | 14/6 | 7/16 | 12/11 | 13/9 | 0.062 |
| 年龄(岁) | 61(20~82) | 57(21~88) | 61(21~77) | 65(29~86) | 0.724 |
| ≥65岁 | 7(35%) | 7(30%) | 7(30%) | 11(50%) | 0.051 |
| 突变情况 | |||||
| JAK2 V617F突变 | 15(75%) | 14(61%) | 10(43%) | 12(55%) | 0.214 |
| CALR突变 | 0 | 1(4%) | 0 | 4(18%) | 0.027 |
| MPL突变 | 0 | 2(9%) | 0 | 0 | 0.125 |
| 三阴性 | 5(25%) | 6(26%) | 13(57%) | 6(27%) | 0.072 |
| 脾肿大 | 3(15%) | 1(4%) | 6(26%) | 12(55%) | 0.001 |
| 明显的骨髓纤维化 | 8(40%) | 7(30%) | 0 | 22(100%) | <0.001 |
| 白细胞增多[n(%)] | 3(15%) | 4(17%) | 14(61%) | 17(77%) | 0.008 |
| 血红蛋白含量降低 | 0 | 1(4%) | 5(22%) | 11(50%) | <0.001 |
| 血小板计数降低(n) | 1(5%) | 0 | 1(4%) | 6(27%) | 0.003 |
| LDH均值(U/L) | 254.0±150.8 | 316.0±271.3 | 328.0±255.8 | 668.0±388.9 | 0.010 |
| 骨髓巨核细胞中位数(个/mm2) | 42(3~120) | 51(1~93) | 23(6~107) | 127(11~273) | <0.001 |
表2
各基因分组患者的临床特点[n(%),中位数(范围)]
| 参数 | JAK2 V617F突变(n=51) | 三阴性(n=30) | CALR突变(n=5) | MPL突变(n=2) | P值 |
|---|---|---|---|---|---|
| 性别(男/女) | 23/28 | 20/10 | 3/2 | 0/2 | 0.057 |
| 年龄(岁) | 64(29~88) | 52(20~79) | 46(21~63) | 64(61~67) | 0.027 |
| ≥65岁 | 24(47%) | 7(23%) | 0 | 1(50%) | 0.281 |
| 脾肿大 | 12(24%) | 8(27%) | 2(40%) | 0 | 0.060 |
| 白细胞增多 | 24(47%) | 12(40%) | 4(80%) | 0 | 0.439 |
| 血红蛋白含量降低 | 8(16%) | 8(27%) | 1(20%) | 0 | 0.914 |
| 血小板计数降低 | 4(8%) | 4(13%) | 1(20%) | 0 | 0.015 |
| LDH均值(U/L) | 402±339 | 348±265 | 839±88 | 153±32 | 0.443 |
| 中重度骨髓纤维化 | 24(47%) | 8(27%) | 5(100%) | 0 | 0.001 |
| 骨髓巨核细胞中位数(个/mm2) | 52(6~273) | 28(3~82) | 111(70~120) | 88(85~91) | 0.234 |
表3
pre-PMF与overt-PMF、ET患者的临床特点比较[n(%),中位数(范围)]
| 参数 | ET组(n=23) | pre-PMF组(n=23) | overt-PMF组(n=22) | P1值 | P2值 |
|---|---|---|---|---|---|
| 性别(男/女) | 7/16 | 12/11 | 13/9 | 0.134 | 0.641 |
| 年龄(岁) | 57(21~88) | 61(21~77) | 65(29~86) | 0.969 | 0.313 |
| ≥65岁 | 7(30%) | 7(30%) | 11(50%) | 1.000 | 0.181 |
| 脾肿大 | 1(4%) | 6(26%) | 12(55%) | 0.043 | 0.051 |
| 白细胞增多 | 4(17%) | 14(61%) | 17(77%) | 0.007 | 0.235 |
| 血红蛋白含量降低 | 1(4%) | 5(22%) | 11(50%) | 0.189 | 0.048 |
| 血小板计数降低 | 0 | 1(4%) | 6(27%) | 1.000 | 0.034 |
| LDH均值(U/L) | 316.0±271.3 | 328.0±255.8 | 668.0±388.9 | 0.922 | 0.037 |
图1
ET患者与pre-PMF患者的生存曲线
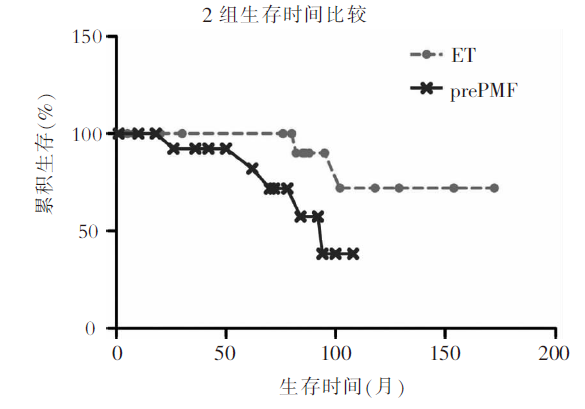
表4
PMF中JAK2突变患者与三阴性患者的临床特点比较[n(%),中位数(范围)]
| 项目 | pre-PMF | overt-PMF | |||||
|---|---|---|---|---|---|---|---|
| JAK2 V617F突变(n=10) | 三阴性(n=13) | P值 | JAK2 V617F突变(n=12) | 三阴性(n=6) | P值 | ||
| 性别(男/女) | 3/7 | 9/4 | 0.463 | 9/3 | 3/3 | 0.294 | |
| 年龄(岁) | 65(35~77) | 50(21~75) | 0.030 | 63(29~71) | 71(43~79) | 0.982 | |
| ≥65岁 | 5(50%) | 2(15%) | 0.092 | 4(33%) | 4(67%) | 0.201 | |
| 脾肿大 | 0 | 6(46%) | 0.017 | 8(67%) | 2(33%) | 0.321 | |
| 白细胞增多 | 7(70%) | 7(54%) | 0.363 | 9(75%) | 4(67%) | 0.561 | |
| 血红蛋白含量降低 | 1(10%) | 4(31%) | 0.251 | 4(33%) | 4(67%) | 0.201 | |
| 血小板计数降低 | 0 | 1(8%) | 0.565 | 5(42%) | 1(17%) | 0.306 | |
| LDH均值(U/L) | 472±343 | 257±198 | 0.260 | 682±443 | 448±414 | 0.527 | |
| [1] |
Tefferi A, Vardiman JW. Classification and diagnosis of myeloproliferative neoplasms: the 2008 World Health Organization criteria and point-of-care diagnostic algorithms[J]. Leukemia, 2008, 22(1):14-22.
pmid: 17882280 |
| [2] |
Arber DA, Orazi A, Hasserjian R, et al. The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia[J]. Blood,2016, 127(20):2391-2405.
doi: 10.1182/blood-2016-03-643544 URL |
| [3] | Vardiman JW, Thiele J, Arber DA, et al. The 2008 revision of the World Health Organization (WHO) classification of myeloid neoplasms and acute leukemia: rationale and important changes[J]. Blood,2009, 114(5):937-951. |
| [4] |
Tefferi A, Guglielmelli P, Larson DR, et al. Long-term survival and blast transformation in molecularly annotated essential thrombocythemia, polycythemia vera, and myelofibrosis[J]. Blood, 2014, 124(16):2507-2513.
doi: 10.1182/blood-2014-05-579136 pmid: 25037629 |
| [5] |
Tefferi A, Barbui T. Polycythemia vera and essential thrombocythemia: 2017 update on diagnosis, risk-stratification, and management[J]. Am J Hematol, 2017, 92(1):94-108.
doi: 10.1002/ajh.24607 pmid: 27991718 |
| [6] |
Tefferi A, Lasho TL, Jimma T, et al. One thousand patients with primary myelofibrosis: the mayo clinic experie-nce[J]. Mayo Clin Proc, 2012, 87(1):25-33.
doi: 10.1016/j.mayocp.2011.11.001 pmid: 22212965 |
| [7] |
Takenaka K, Shimoda K, Uchida N, et al. Clinical features and outcomes of patients with primary myelofibrosis in Japan: report of a 17-year nationwide survey by the Idiopathic Disorders of Hematopoietic Organs Research Committee of Japan[J]. Int J Hematol, 2017, 105(1):59-69.
doi: 10.1007/s12185-016-2102-3 pmid: 27761702 |
| [8] |
Gisslinger H. Pre-PMF emerging as important subgroup of MPN[J]. Blood, 2017, 129(24):3142-3144.
doi: 10.1182/blood-2017-04-777805 pmid: 28620103 |
| [9] |
Barosi G. Essential thrombocythemia vs. early/prefibrotic myelofibrosis: why does it matter[J]. Best Pract Res Clin Haematol, 2014, 27(2):129-140.
doi: 10.1016/j.beha.2014.07.004 URL |
| [10] |
Michiels JJ, Kutti J, Stark P, et al. Diagnosis, pathogenesis and treatment of the myeloproliferative disorders essential thrombocythemia, polycythemia vera and essential megakaryocytic granulocytic metaplasia and myelofibrosis[J]. Neth J Med, 1999, 54(2):46-62.
pmid: 10079679 |
| [11] |
Jeryczynski G, Thiele J, Gisslinger B, et al. Pre-fibrotic/early primary myelofibrosis vs. WHO-defined essential thrombocythemia: The impact of minor clinical diagnostic criteria on the outcome of the disease[J]. Am J Hematol, 2017, 92(9):885-891.
doi: 10.1002/ajh.24788 pmid: 28543356 |
| [12] |
Verstovsek S, Kantarjian H, Mesa RA, et al. Safety and efficacy of INCB018424, a JAK1 and JAK2 inhibitor, in myelofibrosis[J]. N Engl J Med, 2010, 363(12):1117-1127.
doi: 10.1056/NEJMoa1002028 URL |
| [13] |
Mesa RA, Kiladjian JJ, Verstovsek S, et al. Comparison of placebo and best available therapy for the treatment of myelofibrosis in the phase 3 COMFORT studies[J]. Haematologica, 2014, 99(2):292-298.
doi: 10.3324/haematol.2013.087650 URL |
| [14] |
Passamonti F, Cervantes F, Vannucchi AM, et al. A dynamic prognostic model to predict survival in primary myelofibrosis: a study by the IWG-MRT (International Working Group for Myeloproliferative Neoplasms Research and Treatment)[J]. Blood, 2010, 115(9):1703-1708.
doi: 10.1182/blood-2009-09-245837 pmid: 20008785 |
| [15] |
Verstovsek S, Mesa RA, Gotlib J, et al. A double-blind, placebo-controlled trial of ruxolitinib for myelofibrosis[J]. N Engl J Med, 2012, 366(9):799-807.
doi: 10.1056/NEJMoa1110557 URL |
| [16] |
Ghoreschi K, Laurence A, O'Shea JJ. Janus kinases in immune cell signaling[J]. Immunol Rev, 2009, 228(1):273-287.
doi: 10.1111/j.1600-065X.2008.00754.x pmid: 19290934 |
| [17] |
Tefferi A, Lasho TL, Finke CM, et al. CALR vs JAK2 vs MPL-mutated or triple-negative myelofibrosis: clinical, cytogenetic and molecular comparisons[J]. Leukemia, 2014, 28(7):1472-1477.
doi: 10.1038/leu.2014.3 pmid: 24402162 |
| [18] |
Levine RL, Pardanani A, Tefferi A, et al. Role of JAK2 in the pathogenesis and therapy of myeloproliferative disor-ders[J]. Nat Rev Cancer, 2007, 7(9):673-683.
doi: 10.1038/nrc2210 pmid: 17721432 |
| [19] |
Harrison C, Kiladjian JJ, Al-Ali HK, et al. JAK inhibition with ruxolitinib versus best available therapy for myelofibrosis[J]. N Engl J Med, 2012, 366(9):787-798.
doi: 10.1056/NEJMoa1110556 URL |
| [1] | 何亲羽, 王伟, 陈立芬, 张雪蕾, 董治亚. LHCGR基因突变致家族性男性性早熟2例报告及文献复习[J]. 诊断学理论与实践, 2022, 21(05): 598-605. |
| [2] | 陈志敏, 何浩岚. 艾滋病合并马尔尼菲篮状菌病的诊治现状[J]. 诊断学理论与实践, 2022, 21(04): 425-430. |
| [3] | 沈银忠. 《人类免疫缺陷病毒感染/艾滋病合并结核分枝杆菌感染诊治专家共识》解读[J]. 诊断学理论与实践, 2022, 21(04): 431-436. |
| [4] | 陈宏, 沈银忠. 人类免疫缺陷病毒感染/艾滋病合并结核病的诊治进展[J]. 诊断学理论与实践, 2022, 21(04): 530-534. |
| [5] | 何新, 陈慧, 冯炜炜. 机器学习算法在辅助超声诊断附件肿块良恶性中的应用研究进展[J]. 诊断学理论与实践, 2022, 21(04): 541-546. |
| [6] | 徐子真, 李擎天, 刘湘帆, 李莉, 李惠, 王也飞, 吴洁敏, 陈宁, 梁璆荔, 陈松立, 戴健敏, 宋珍, 丁磊. 实验诊断学在线课程的建立和实践[J]. 诊断学理论与实践, 2022, 21(04): 547-550. |
| [7] | 赵然, 詹维伟, 侯怡卿. 计算机辅助诊断系统辅助超声诊断甲状腺弥漫性病变合并结节良恶性的应用价值[J]. 诊断学理论与实践, 2022, 21(03): 390-394. |
| [8] | 郭业兵, 郑金峰. 阴道壁胃肠道外间质瘤一例报道并文献复习[J]. 诊断学理论与实践, 2022, 21(03): 405-407. |
| [9] | 王刚, 陈生弟. 神经病学的诊断:起源、发展及挑战[J]. 诊断学理论与实践, 2022, 21(01): 1-4. |
| [10] | 唐静仪, 余群, 刘军. 结合人工智能的结构影像分析对阿尔茨海默病的早期预测及精准诊断研究进展[J]. 诊断学理论与实践, 2022, 21(01): 12-17. |
| [11] | 魏文石. 直面我国阿尔茨海默病诊治的挑战——《中国阿尔茨海默病报告2021》解读[J]. 诊断学理论与实践, 2022, 21(01): 5-7. |
| [12] | 王蔚, 王小钦. 缺铁性贫血的病因诊断[J]. 诊断学理论与实践, 2021, 20(06): 529-532. |
| [13] | 岳婧婧, 宋琦, 江旭峰, 王黎, 赵维莅, 严福华. 磁共振全身扩散加权成像结合T2WI抑脂序列与FDG-PET/CT在初发淋巴瘤分期及病灶检出的对比研究[J]. 诊断学理论与实践, 2021, 20(06): 540-546. |
| [14] | 王昭晖, 吴海波. 胃神经鞘瘤31例临床病理学分析[J]. 诊断学理论与实践, 2021, 20(06): 552-556. |
| [15] | 王广宇, 杨昕, 张立娟, 谭姣容. 住院新诊断2型糖尿病男性患者血浆总睾酮水平与骨钙素的相关性研究[J]. 诊断学理论与实践, 2021, 20(06): 573-578. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||