诊断学理论与实践 ›› 2023, Vol. 22 ›› Issue (02): 147-153.doi: 10.16150/j.1671-2870.2023.02.007
林瀚1, 祖拜热古丽·麦麦提阿卜拉2, 苏同轩1( )
)
收稿日期:2022-06-24
出版日期:2023-04-25
发布日期:2023-08-31
通讯作者:
苏同轩 E-mail: wysstx@yeah.net
LIN Han1, ZUBAIREGULI Maimaitiabula2, SU Tongxuan1()
Received:2022-06-24
Online:2023-04-25
Published:2023-08-31
摘要:
目的:研究肝素结合蛋白(heparin-binding protein,HBP)检测在辅助诊断血流感染中的价值。方法:选取上海交通大学医学院附属瑞金医院2021年1月至2022年1月期间收治的207例血培养阳性住院患者及94例血培养阴性住院患者。检测血培养标本采集当日患者的HBP、降钙素原(procalcitonin, PCT)、C反应蛋白(C-reactive protein, CRP)水平及白细胞计数(white blood cell count, WBC)、中性粒细胞计数(absolute neutrophil count, ANC)、中性粒细胞/淋巴细胞计数比值(neutrophil-lymphocyte count ratio, NLCR)。比较血培养阳性组与阴性组间各指标水平的差异,并比较不同病原菌血流感染患者的HBP水平差异,用受试者操作特征曲线(receiver operator characteristic curve, ROC曲线)评估上述指标单独及联合检测对血流感染的辅助诊断价值。结果:血培养阳性患者的所有指标水平均显著高于血培养阴性患者。革兰阳性菌组血流感染患者的HBP水平与革兰阴性菌组患者相比,差异无统计学意义(中位数,70.26 ng/mL比89.15 ng/mL),但二者均显著高于真菌感染患者(中位数22.90 ng/mL)(P<0.05)。诊断血流感染的ROC曲线显示,HBP的曲线下面积最大(0.742),灵敏度为66.80%,特异度为74.40%,诊断效能显著优于WBC(0.622,灵敏度64.70%,特异度59.80%)、ANC(0.651,灵敏度51.60%,特异度75.60%)和NLCR(0.618,灵敏度72.10%,特异度48.80%)(P<0.05),且在排除恶性肿瘤或造血系统疾病患者后,HBP仍有相近的诊断效能(0.708,灵敏度60.50%,特异度78.70%)。HBP联合PCT检测是辅助诊断血流感染的最优组合,曲线下面积达0.751。结论:HBP检测对血流感染诊断有较好的参考价值。PCT是HBP联合检测诊断血流感染的优选项。
中图分类号:
林瀚, 祖拜热古丽·麦麦提阿卜拉, 苏同轩. 肝素结合蛋白辅助临床血流感染诊断的价值[J]. 诊断学理论与实践, 2023, 22(02): 147-153.
LIN Han, ZUBAIREGULI Maimaitiabula, SU Tongxuan. Value of heparin-binding protein in diagnosis of bloodstream infection[J]. Journal of Diagnostics Concepts & Practice, 2023, 22(02): 147-153.
表1
各指标在血流感染和非血流感染中的血清水平差异[中位数(P25,P75)]
| Biomarkers | Patients with blood culture positive (n=207) | Patients with blood culture negative (n=94) | P |
|---|---|---|---|
| HBP(ng/mL) | 76.13(22.90, 148.27) | 15.29(7.15, 44.46) | <0.001 |
| PCT(ng/mL) | 1.01(0.33, 4.92) | 0.27(0.11, 1.33) | <0.001 |
| CRP(ng/mL) | 120.80(52.00, 178.1) | 52.50(13.95, 120.45) | <0.001 |
| WBC(109/L) | 10.28(5.80, 14.36) | 7.40(3.69, 12.43) | 0.001 |
| ANC(109/L) | 8.99(4.78, 12.39) | 5.65(2.50, 8.96) | <0.001 |
| NLCR | 11.30(6.27, 19.04) | 7.45(3.98, 13.19) | 0.001 |
表2
不同类型病原菌感染患者血清标志物水平差异[中位数(P25,P75)]
| Biomarkers | Gram-negative Bacteria(n=136) | Gram-positive Bacteria(n=53) | Fungi(n=18) |
|---|---|---|---|
| HBP(ng/mL) | 89.15(37.85, 168.46)* | 70.26(17.37, 141.87)Δ | 22.90(11.10, 34.64)*Δ |
| PCT(ng/mL) | 1.47(0.45, 7.12)*# | 0.40(0.19, 1.36)# | 0.66(0.29, 1.82)* |
| CRP(mg/L) | 134.40(69.18, 186.18)*# | 84.90(18.40, 150.00)# | 60.00(52.00,100.00)* |
| WBC(109/L) | 11.48(7.13, 15.28)*# | 8.76(5.56, 13.08)# | 5.97(3.55, 11.63)* |
| ANC(109/L) | 9.56(5.63, 13.08)*# | 7.08(4.02, 11.12)# | 4.60(2.69, 9.99)* |
| NLCR | 12.40(7.52, 20.91)*# | 8.79(4.50, 14.78)# | 5.34(3.80, 12.45)* |
表3
不同病原菌感染患者血清HBP水平差异
| Species | Number | Percent | HBP (ng/mL) [Median(P25, P75)] |
|---|---|---|---|
| Gram-negative bacteria | |||
| Klebsiella Pneumoniae | 66 | 31.89% | 100.77(49.09, 186.47) |
| Acinetobacter baumannii | 23 | 11.11% | 106.31(20.88, 149.04) |
| Pseudomonas aeruginosa | 17 | 8.21% | 112.07(46.35, 162.37) |
| Escherichia coli | 16 | 7.73% | 57.05(17.80, 113.95) |
| other | 14 | 6.76% | 70.99(22.92,142.62) |
| Gram-positive bacteria | |||
| Staphylococcus epidermidis | 14 | 6.76% | 125.04(43.53, 242.84) |
| Enterococcus faecalis | 10 | 4.83% | 102.44(16.45, 175.84) |
| Staphylococcus aureus | 7 | 3.38% | 24.59(17.00, 141.87) |
| Staphylococcus hominis | 4 | 1.93% | 40.79(12.94, 111.50) |
| other | 18 | 8.70% | 64;45(13.87, 112.43) |
| Fungi | |||
| Candida parapsilosis | 9 | 4.35% | 22.90(7.15, 62.23) |
| Candida tropicalis | 4 | 1.93% | 23.19(11.65, 156.98) |
| other | 5 | 2.42% | 22.90(<5.90, 45.11) |
表4
各指标在血流感染中的诊断价值
| Biomarkers | AUC | Asymptotic significance | 95% Confidence interval | Cut-off | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| HBP(ng/mL) | 0.742 | <0.001 | 0.676-0.808 | 38.30 | 66.80% | 74.40% |
| PCT(ng/mL) | 0.685 | <0.001 | 0.614-0.757 | 0.24 | 84.70% | 47.60% |
| CRP(mg/L) | 0.680 | <0.001 | 0.610-0.750 | 103.50 | 54.70% | 74.40% |
| WBC(109/L) | 0.622* | 0.001 | 0.548-0.697 | 8.25 | 64.70% | 59.80% |
| ANC | 0.651* | <0.001 | 0.578-0.723 | 8.61 | 51.60% | 75.60% |
| NLCR | 0.618* | 0.002 | 0.545-0.692 | 6.86 | 72.10% | 48.80% |
图1
各指标诊断血流感染中的ROC曲线
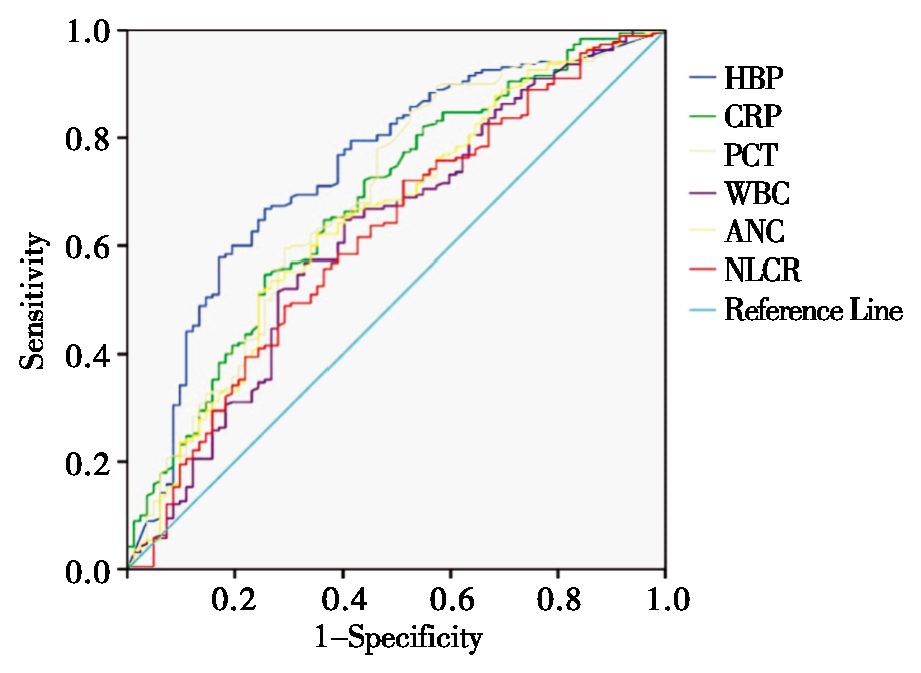
表5
各指标在非恶性肿瘤及造血疾病的血流感染患者中的诊断价值
| Biomarkers | AUC | Asymptotic significance | 95% Confidence interval | Cut-off | Sensitivity | Specificity |
|---|---|---|---|---|---|---|
| HBP | 0.708 | <0.001 | 0.622-0.794 | 59.03 | 60.50% | 78.70% |
| PCT | 0.598 | 0.039 | 0.503-0.694 | 0.24 | 85.50% | 33.40% |
| CRP | 0.602 | 0.033 | 0.511-0.692 | 103.50 | 55.80% | 66.00% |
| WBC | 0.527 | 0.57 | 0.433-0.621 | 10.16 | 53.50% | 61.70% |
| ANC | 0.559 | 0.212 | 0.467-0.651 | 8.61 | 52.90% | 66.00% |
| NLCR | 0.554 | 0.257 | 0.461-0.647 | 9.93 | 58.70% | 55.30% |
表6
HBP联合各炎性指标检测在血流感染中的诊断价值
| Combined biomarkers | AUC | Asymptotic significance | 95% Confidence interval | Sensitivity | Specificity |
|---|---|---|---|---|---|
| HBP+PCT | 0.751 | <0.001 | 0.686-0.817 | 63.70% | 78.00% |
| HBP+CRP | 0.734 | <0.001 | 0.668-0.800 | 70.50% | 68.30% |
| HBP+WBC | 0.727 | <0.001 | 0.660-0.794 | 70.50% | 69.50% |
| HBP+ANC | 0.732 | <0.001 | 0.665-0.800 | 79.50% | 62.20% |
| HBP+NLCR | 0.743 | <0.001 | 0.677-0.809 | 67.40% | 74.40% |
| ALL biomarkers combined | 0.737 | <0.001 | 0.670-0.805 | 79.50% | 64.60% |
| [1] |
XIE J, WANG H, KANG Y, et al. The Epidemiology of Sepsis in Chinese ICUs: A National Cross-Sectional Survey[J]. Crit Care Med, 2020, 48(3):e209-e218.
doi: 10.1097/CCM.0000000000004155 URL |
| [2] |
BAUER M, GERLACH H, VOGELMANN T, et al. Mortality in sepsis and septic shock in Europe, North America and Australia between 2009 and 2019- results from a systematic review and meta-analysis[J]. Crit Care, 2020, 24(1):239.
doi: 10.1186/s13054-020-02950-2 |
| [3] |
GOTO M, AL-HASAN M N. Overall burden of bloodstream infection and nosocomial bloodstream infection in North America and Europe[J]. Clin Microbiol Infect, 2013, 19(6):501-509.
doi: 10.1111/1469-0691.12195 URL |
| [4] |
PAOLI C J, REYNOLDS M A, SINHA M, et al. Epidemio-logy and Costs of Sepsis in the United States-An Analysis Based on Timing of Diagnosis and Severity Level[J]. Crit Care Med, 2018, 46(12):1889-1897.
doi: 10.1097/CCM.0000000000003342 URL |
| [5] |
PIERRAKOS C, VINCENT J L. Sepsis biomarkers: a review[J]. Crit Care, 2010, 14(1):R15.
doi: 10.1186/cc8872 URL |
| [6] |
SHAFER W M, MARTIN L E, SPITZNAGEL J K. Catio-nic antimicrobial proteins isolated from human neutrophil granulocytes in the presence of diisopropyl fluorophosphate[J]. Infect Immun, 1984, 45(1):29-35.
doi: 10.1128/iai.45.1.29-35.1984 URL |
| [7] |
GAUTAM N, OLOFSSON A M, HERWALD H, et al. Heparin-binding protein (HBP/CAP37): a missing link in neutrophil-evoked alteration of vascular permeability[J]. Nat Med, 2001, 7(10):1123-1127.
doi: 10.1038/nm1001-1123 pmid: 11590435 |
| [8] |
FISHER J, LINDER A. Heparin-binding protein: a key player in the pathophysiology of organ dysfunction in sepsis[J]. J Intern Med, 2017, 281(6):562-574.
doi: 10.1111/joim.12604 pmid: 28370601 |
| [9] | 刘珍, 王峰, 高晖, 等. 血浆肝素结合蛋白联合降钙素原及C-反应蛋白对脓毒症及脓毒性休克患者诊断价值的研究[J]. 中国卫生检验杂志, 2021, 31(22):2696-2701. |
| LIU Z, WANG F, GAO H, et al. A study on the diagnostic value of plasma heparin binding protein combined with procalcitonin and C-reactive protein for patients with sepsis and septic shock[J]. Chin J Health Lab Technol, 2021, 31(22):2696-2701. | |
| [10] | 李磊, 郑传明, 夏群, 等. 肝素结合蛋白联合降钙素原在评估急性胰腺炎合并感染中的预测价值[J]. 中华全科医学, 2020, 18(6):927-929,1068. |
| LI L, ZHENG C M, XIA Q, et al. Predictive value of heparin-binding protein combined with procalcitonin in the assessment of acute pancreatitis co-infection[J]. Chin J Gen Pract, 2020, 18(6):927-929,1068. | |
| [11] | 张晓彤, 国世星, 邵青, 等. 多因子联合检测在诊断血流感染和指导抗菌药物早期合理使用中的应用价值[J]. 实用检验医师杂志, 2020, 12(1):37-41. |
| ZHANG X T, GUO S X, SHAO Q, et al. Application value of multi-factor combined detection in diagnosis of bloodstream infection and guidance for early rational use of antibacterial drugs[J]. Chin J Clin Pathol, 2020, 12(1):37-41. | |
| [12] | 潘晓微, 李克诚. 血浆肝素结合蛋白和降钙素原对血流感染的诊断价值[J]. 检验医学, 2017, 32(11):999-1003. |
| PAN X W, LI K C. Plasma heparin binding protein and procalcitonin in the diagnosis of bloodstream infection[J]. Lab Med, 2017, 32(11):999-1003. | |
| [13] |
MELLHAMMAR L, THELAUS L, ELÉN S, et al. Heparin binding protein in severe COVID-19-A prospective observational cohort study[J]. PLoS One, 2021, 16(4):e0249570.
doi: 10.1371/journal.pone.0249570 URL |
| [14] |
LINDER A, ÅKESSON P, INGHAMMAR M, et al. Ele-vated plasma levels of heparin-binding protein in intensive care unit patients with severe sepsis and septic shock[J]. Crit Care, 2012, 16(3):R90.
doi: 10.1186/cc11353 URL |
| [15] |
WU Y L, YO C H, HSU W T, et al. Accuracy of Heparin-Binding Protein in Diagnosing Sepsis: A Systematic Review and Meta-Analysis[J]. Crit Care Med, 2021, 49(1):e80-e90.
doi: 10.1097/CCM.0000000000004738 URL |
| [16] |
ANSAR W, GHOSH S. C-reactive protein and the bio-logy of disease[J]. Immunol Res, 2013, 56(1):131-142.
doi: 10.1007/s12026-013-8384-0 URL |
| [17] |
LI S, RONG H, GUO Q, et al. Serum procalcitonin levels distinguish Gram-negative bacterial sepsis from Gram-positive bacterial and fungal sepsis[J]. J Res Med Sci, 2016, 21:39.
pmid: 27904585 |
| [18] |
WACKER C, PRKNO A, BRUNKHORST F M, et al. Procalcitonin as a diagnostic marker for sepsis: a systematic review and meta-analysis[J]. Lancet Infect Dis, 2013, 13(5):426-435.
doi: 10.1016/S1473-3099(12)70323-7 pmid: 23375419 |
| [19] |
KERN W V, RIEG S. Burden of bacterial bloodstream infection-a brief update on epidemiology and significance of multidrug-resistant pathogens[J]. Clin Microbiol Infect, 2020, 26(2):151-157.
doi: 10.1016/j.cmi.2019.10.031 URL |
| [20] | 万会林, 孔德华, 周万青, 等. 降钙素原、C-反应蛋白、白细胞和中性粒细胞在鉴别血流感染中的应用价值[J]. 世界复合医学, 2019, 5(12):41-43. |
| WAN H L, KONG D H, ZHOU W Q, et al. The Application Value of Procalcitonin, C-reactive Protein, Leukocytes and Neutrophils in Differential Bloodstream Infection[J]. World J Complex Med, 2019, 5(12):41-43. | |
| [21] |
OBERHOFFER M, STONANS I, RUSSWURM S, et al. Procalcitonin expression in human peripheral blood mononuclear cells and its modulation by lipopolysaccharides and sepsis-related cytokines in vitro[J]. J Lab Clin Med, 1999, 134(1):49-55.
pmid: 10402059 |
| [22] |
BERAN O, POTMĚŠIL R, HOLUB M. Differences in Toll-like receptor expression and cytokine production after stimulation with heat-killed Gram-positive and Gram-negative bacteria[J]. Folia Microbiol (Praha), 2011, 56(3):283-287.
doi: 10.1007/s12223-011-0025-1 URL |
| [23] |
SNÄLL J, LINNÉR A, UHLMANN J, et al. Differential neutrophil responses to bacterial stimuli: Streptococcal strains are potent inducers of heparin-binding protein and resistin-release[J]. Sci Rep, 2016, 6:21288.
doi: 10.1038/srep21288 pmid: 26887258 |
| [1] | 刘婧娴, 陈峰, 刘瑛. 分离胶促凝管法联合基质辅助激光解吸电离飞行时间质谱鉴定1例蜡样芽胞杆菌血流感染[J]. 诊断学理论与实践, 2019, 18(1): 107-108. |
| [2] | 张舒, 王露露, 孙璟, 江石湖. 降钙素原和C反应蛋白在急性胆源性胰腺炎中的诊断及预后价值比较[J]. 诊断学理论与实践, 2019, 18(06): 668-671. |
| [3] | 王媛媛, 范秋灵. 血清降钙素原在慢性肾脏病合并细菌感染患者中的临床价值[J]. 诊断学理论与实践, 2019, 18(03): 353-359. |
| [4] | 杜坤, 杨喜, 卞炳贤, 任懿倩, 张广慧. 血清presepsin(sCD14-ST)、降钙素原、C反应蛋白和白介细胞素-6诊断血流细菌感染的诊断性能比较[J]. 诊断学理论与实践, 2018, 17(05): 581-585. |
| [5] | 陆世娟, 尚庆毅, 蒋志红, 陈同排, 张小庆. IP-10联合PCT和hs-CRP检测对新生儿感染性疾病的诊断价值[J]. 诊断学理论与实践, 2018, 17(03): 304-307. |
| [6] | 沈晓红, 陈慧芬, 张军, 叶剑波, 张贤华. 2014年至2017年上海地区新生儿血流感染病原菌分布及其耐药性分析[J]. 诊断学理论与实践, 2018, 17(03): 266-271. |
| [7] | 何晶晶, 张雁, 周玉珍, 刘景瑶, 赵冬梅, 郑遵荣. 降钙素原与C-反应蛋白的动态监测在人急性布鲁杆菌病诊疗中的应用[J]. 诊断学理论与实践, 2017, 16(06): 617-621. |
| [8] | 王琳琳, 祝程诚, 张庆五, 陈婷, 吴舜. 血清PCT、IL-6、CRP水平在老年社区获得性肺炎鉴别诊断中的价值[J]. 诊断学理论与实践, 2017, 16(05): 532-536. |
| [9] | 陆子贇, 彭怡倩, 应春妹,. 降钙素原和C反应蛋白联合检测在新生儿感染性疾病诊断中的应用评估[J]. 诊断学理论与实践, 2016, 15(02): 157-159. |
| [10] | 罗晓颖, 权薇薇, 许燕, 张风如, 吴立群, 戚文航,. C反应蛋白与房颤冷冻球囊导管消融术后房颤复发的相关性研究[J]. 诊断学理论与实践, 2015, 14(03): 219-222. |
| [11] | 万颖蕾, 李文静, 项明洁,. 血清淀粉样蛋白A在感染性疾病中的诊断价值[J]. 诊断学理论与实践, 2015, 14(02): 190-192. |
| [12] | 畅凌, 郭恒, 雷英, 吴倩, 张兰, 黄刚,. 老年轻度认知功能障碍IL-6、hs-CRP检测的临床意义[J]. 诊断学理论与实践, 2014, 13(04): 416-418. |
| [13] | 张群, 范立权, 胡晓波, 许洁,. 降钙素原和C反应蛋白在细菌和真菌感染中的辅助诊断价值[J]. 诊断学理论与实践, 2014, 13(02): 202-205. |
| [14] | 林青, 崔佩菁, 庞小芬,. 老年良性前列腺增生症与高敏C反应蛋白相关性研究[J]. 诊断学理论与实践, 2012, 11(05): 521-523. |
| [15] | 戴晓慧, 朱月潜,. 新诊断高血压患者颈动脉内中膜厚度和C反应蛋白的研究[J]. 诊断学理论与实践, 2011, 10(05): 471-474. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||