内科理论与实践 ›› 2023, Vol. 18 ›› Issue (03): 157-164.doi: 10.16138/j.1673-6087.2023.03.005
李花1,2*, 黄晓敏1*, 张春燕1, 杜路1,3, 任红1, 徐天1( )
)
收稿日期:2022-11-07
出版日期:2023-06-30
发布日期:2023-08-07
通讯作者:
徐 天 E-mail: 作者简介:*李花与黄晓敏为共同第一作者
基金资助:
LI Hua1,2*, HUANG Xiaomin1*, ZHANG Chunyan1, DU Lu1,3, REN Hong1, XU Tian1()
Received:2022-11-07
Online:2023-06-30
Published:2023-08-07
摘要:
目的: 探讨腹膜透析(peritoneal dialysis,PD)患者血清氨基末端脑钠肽前体(N-terminal pro-B natriuretic peptide,NT-proBNP)水平与患者水合状态、心功能指标的关系,并进一步分析影响PD患者NT-proBNP水平的因素。方法: 回顾性收集2019年5月—2022年1月在上海交通大学医学院附属瑞金医院PD中心随访的PD患者111例,根据多频生物电阻抗人体成分分析仪(body composition monitor,BCM)测定结果,按相对水合状态(relative hydration status,DHS),即超负荷水量(overhydration,OH)和细胞外水(extracellular water,ECW)比值,将其分为容量正常组(OH/ECW≤15%)与容量超负荷组(OH/ECW>15%)。比较2组患者血清NT-proBNP水平与水合状态关系,并进一步分析探讨影响NT-proBNP水平的相关因素。以BCM结果作为“金标准”,受试者操作特征曲线(receiver operator characteristic curve,ROC曲线)确定容量超负荷时NT-proBNP最佳阈值。并根据NT-proBNP进行分组,比较2组的临床资料。结果: 容量超负荷组和容量正常组在收缩压、尿量、总尿素清除指数(urea clearance index,Kt/V)、总肌酐清除率(creatinine clearance rate,CCr)、4 h透析液肌酐/血肌酐比值(dialysate to plasma ratio for urea at 4 hours,4hD/PCr)、降压药种类、利尿剂种类、血红蛋白、血清白蛋白、log2(NT-proBNP)、室间隔厚度(interventricular septal thickness,IVST)、左室后壁厚度(left ventricular posterior wall thickness,LVPWT)、左房内径(left atrial diameter,LAD)、OH、TBW、ECW、OH/TBW、ECW/TBW、ECW/ICW方面差异有统计学意义(均P<0.05)。log2(NT-proBNP)水平与收缩压、透析龄、超滤量、透析剂量、降压药分组、IVST、LVPWT、LAD、左心室收缩末期内径(left ventricular end-systolic dimension,LVESD)、左室舒张末期内径(left ventricular end-diastolic dimension,LVEDD)、OH、OH/ECW呈正相关(均P<0.05),与尿量、总Kt/V、总CCr、标准蛋白分解率(normalized protein catabolic rate,nPCR)、血红蛋白、血清白蛋白、左室射血分数(left ventricular ejection fraction,LVEF)呈负相关(均P<0.05)。NT-proBNP 4 896 ng/L可作为初筛容量超负荷的临界值,按此分组的2组患者收缩压、尿量、超滤量、总Kt/V、总CCr、IVST、LVPWT、OH/ECW指标差异有统计学意义(均P<0.05)。结论: PD患者NT-proBNP水平普遍升高,其大于4 896 ng/L提示容量超负荷,可作为初步判断PD患者容量超负荷的简易监测指标。
中图分类号:
李花, 黄晓敏, 张春燕, 杜路, 任红, 徐天. 血清氨基末端脑钠肽前体水平初筛腹膜透析患者容量超负荷的价值[J]. 内科理论与实践, 2023, 18(03): 157-164.
LI Hua, HUANG Xiaomin, ZHANG Chunyan, DU Lu, REN Hong, XU Tian. Value of serum N-terminal pro-brain natriuretic peptide levels in primary screening peritoneal dialysis patients with volume overload[J]. Journal of Internal Medicine Concepts & Practice, 2023, 18(03): 157-164.
表1
PD患者的临床、PD及血生化指标[$\bar{x}±s$/n/M(Q1,Q3)]
| 指标 | 容量正常组(n=59) | 容量超负荷组(n=52) | 统计量 | P |
|---|---|---|---|---|
| 年龄(岁) | 55.99±14.75 | 53.91±14.57 | 0.155 | >0.05 |
| 性别(男/女) | 29/31 | 34/18 | 2.967 | >0.05 |
| BMI(kg/m2) | 22.53±2.84 | 22.39±3.38 | 2.010 | >0.05 |
| 收缩压(mmHg) | 140.00±20.64 | 152.50±24.12 | 0.283 | 0.004 |
| 舒张压(mmHg) | 82.75±11.72 | 86.54±13.46 | 0.608 | >0.05 |
| 透析龄(月) | 62.3(46.5,81.2) | 65.8(42.8,92.5) | 3 134.0 | >0.05 |
| 透析剂量(L/24 h) | 7.84±1.80 | 8.46±1.75 | 0.391 | >0.05 |
| 尿量(mL/24 h) | 800(220,1 200) | 300(0,748) | 2 373.5 | 0.001 |
| 超滤量(mL/24 h) | 500(225,760) | 665(325,975) | 2 979.0 | >0.05 |
| Kt/V | 2.24±0.42 | 2.04±0.49 | 2.588 | 0.024 |
| CCr(L/周) | 70.75±25.99 | 58.72±19.22 | 7.145 | 0.007 |
| nPCR | 0.94±0.16 | 0.92±0.21 | 1.910 | >0.05 |
| 4hD/PCr(μmol/L) | 0.59±0.09 | 0.65±0.11 | 4.685 | 0.003 |
| 腹膜转运类型(低/高) | 44/15 | 24/28 | 9.409 | 0.002 |
| 降压药种类(<3种及≥3种) | 46/13 | 22/29 | 14.058 | 0.000 |
| 利尿剂种类(有/无) | 54/5 | 32/19 | 13.283 | 0.000 |
| CRP(mg/L) | 1.55(0.52,4.63) | 1.87(0.65,5.81) | 3 129.5 | >0.05 |
| 血红蛋白(g/L) | 112.22±16.07 | 105.25±17.27 | 0.555 | 0.030 |
| 血钠(mmol/L) | 141.28±2.86 | 140.92±2.75 | 0.348 | >0.05 |
| 血糖(mmol/L) | 5.25±1.78 | 4.98±1.13 | 1.370 | >0.05 |
| 血清白蛋白(mmol/L) | 36.71±4.34 | 33.81±4.83 | 0.535 | 0.001 |
| 血钙(mmol/L) | 2.34±0.16 | 2.28±0.17 | 0.632 | >0.05 |
| 血磷(mmol/L) | 1.69±0.45 | 1.73±0.53 | 1.749 | >0.05 |
| 总胆固醇(mmol/L) | 5.09±1.07 | 4.77±1.29 | 1.966 | >0.05 |
| 甘油三酯(mmol/L) | 2.02±1.10 | 1.71±1.12 | 0.016 | >0.05 |
| 低密度脂蛋白(mmol/L) | 3.11±0.93 | 2.90±1.04 | 0.820 | >0.05 |
| Iog 2(NT-proBNP) | 10.93±2.22 | 12.60±1.95 | 1.171 | 0.000 |
表2
PD患者的超声心动图及生物电阻抗指标[$\bar{x}±s$/M(Q1,Q3)]
| 指标 | 容量正常组(n=59) | 容量超负荷组(n=52) | 统计量 | P |
|---|---|---|---|---|
| IVST(mm) | 9.90±1.50 | 11.04±2.10 | 1.375 | 0.002 |
| LVPWT(mm) | 9.65±1.57 | 10.51±2.43 | 2.408 | 0.037 |
| LAD(mm) | 38.50±5.20 | 41.12±4.68 | 0.455 | 0.009 |
| LVESD(mm) | 32.42±5.40 | 32.57±4.63 | 0.334 | >0.05 |
| LVEDD(mm) | 50.39±5.56 | 51.31±4.98 | 1.458 | >0.05 |
| LVESV(mL) | 44.50±20.12 | 44.33±15.93 | 0.354 | >0.05 |
| LVEDV(mL) | 122.56±32.64 | 128.10±29.53 | 1.126 | >0.05 |
| LVEF(%) | 64.65±6.69 | 65.82±5.03 | 0.546 | >0.05 |
| OH(L) | 1.4(0.8,2.3) | 3.9(3.2,5.28) | 1 847.0 | 0.000 |
| TBW(L) | 34.30±7.03 | 38.28±9.94 | 3.437 | 0.016 |
| ECW(L) | 15.65±2.90 | 18.78±4.83 | 5.361 | 0.000 |
| ICW(L) | 18.65±4.34 | 19.50±5.46 | 1.599 | >0.05 |
| OH/TBW | 0.46(0.24,0.62) | 0.11(0.84,0.14) | 1 778.0 | 0.000 |
| ECW/TBW | 0.460±0.027 | 0.493±0.029 | 0.347 | 0.000 |
| ECW/ICW | 0.855±0.092 | 0.978±0.116 | 2.363 | 0.000 |
表3
log2(NT-proBNP)水平与PD患者临床指标的相关性
| 指标 | r | P |
|---|---|---|
| 收缩压 | 0.320 | 0.001 |
| 透析龄 | 0.301 | 0.001 |
| 超滤量 | 0.435 | 0.000 |
| 透析剂量 | 0.469 | 0.000 |
| 降压药分组 | 0.404 | 0.000 |
| IVST | 0.534 | 0.000 |
| LVPWT | 0.543 | 0.000 |
| LAD | 0.547 | 0.000 |
| LVESD | 0.346 | 0.000 |
| LVEDD | 0.357 | 0.000 |
| OH | 0.496 | 0.000 |
| OH/ECW | 0.516 | 0.000 |
| 尿量 | -0.589 | 0.000 |
| 总Kt/V | -0.352 | 0.000 |
| 总CCr | -0.538 | 0.000 |
| nPCR | -0.192 | 0.043 |
| 血红蛋白 | -0.382 | 0.000 |
| 血清白蛋白 | -0.228 | 0.016 |
| LVEF | -0.213 | 0.032 |
图1
log2(NT-proBNP)水平与PD患者临床指标的相关性分析散点图
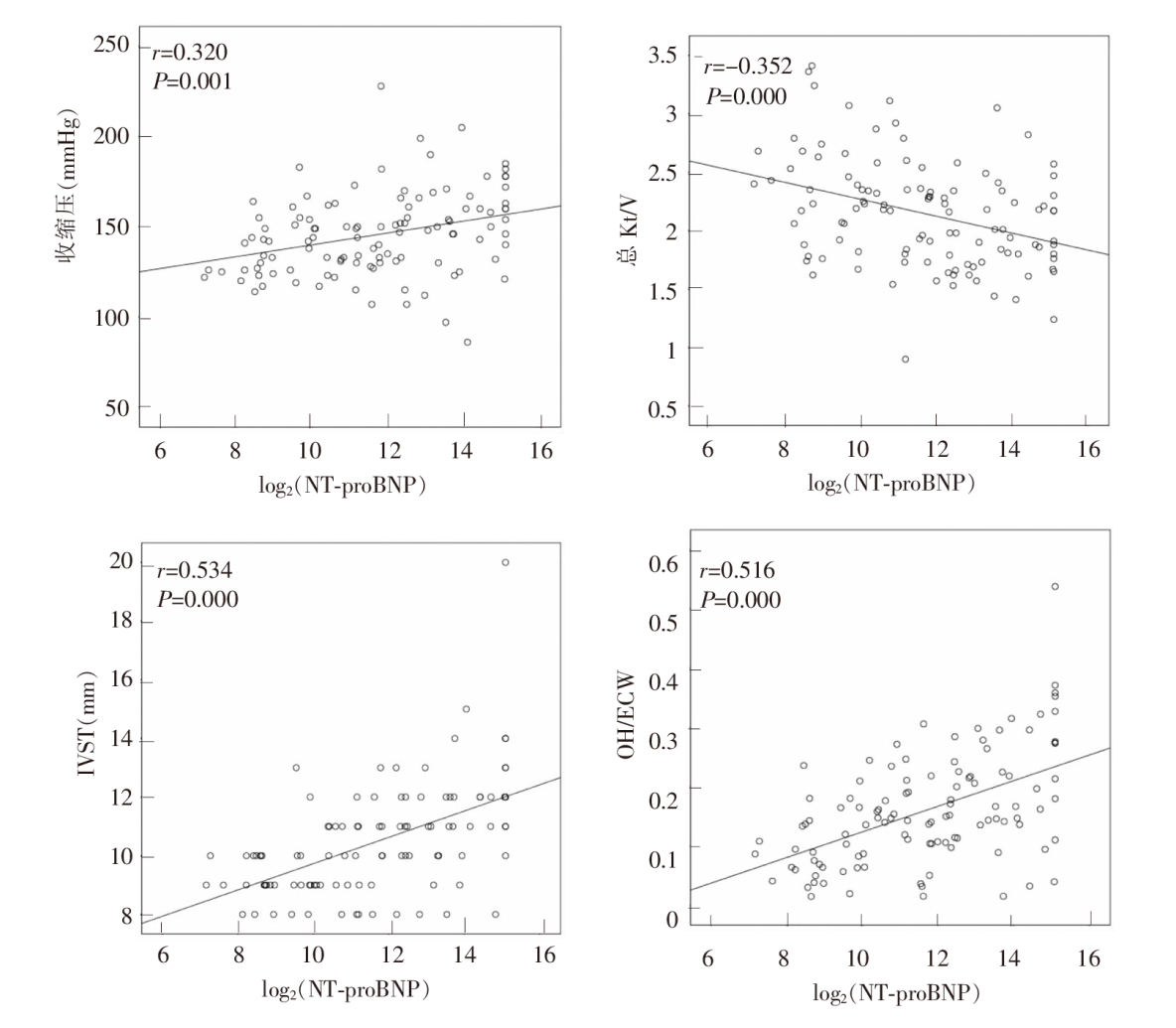
图2
PD患者NT-proBNP水平与容量负荷ROC曲线图
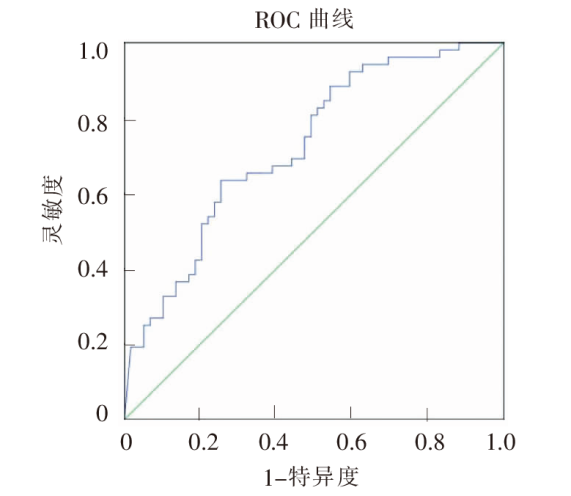
表4
以NT-proBNP 4 896 ng/L为临界值比较PD患者主要临床指标[$\bar{x}±s$/M(Q1,Q3)]
| 指标 | NT-proBNP≥4 896 ng/L(n=48) | NT-proBNP<4 896 ng/L(n=63) | 统计量 | P |
|---|---|---|---|---|
| BMI(kg/m2) | 22.85±2.91 | 22.15±3.23 | 0.227 | >0.05 |
| 收缩压(mmHg) | 152.40±25.06 | 140.29±19.95 | 2.032 | 0.005 |
| 尿量(mL/24 h) | 135.0(0,437.5) | 800(500,1 200) | 1 792.5 | 0.000 |
| 超滤量(mL/24 h) | 767.0(500.0,1 022.5) | 480(224,698) | 2 896.0 | 0.000 |
| Kt/V | 1.97±0.38 | 2.28±0.47 | 1.033 | 0.000 |
| CCr(L/周) | 51.7(45.8,56.9) | 69.3(52.8,90.3) | 1 886.0 | 0.000 |
| IVST(mm) | 11.47±2.07 | 9.71±1.34 | 2 261.5 | 0.000 |
| LVPWT(mm) | 11.16±2.49 | 9.26±1.18 | 2 248 | 0.000 |
| LVEF(%) | 63.84±7.48 | 66.24±7.48 | 1 996.5 | 0.044 |
| OH/ECW | 0.21±0.10 | 0.12±0.07 | 5.593 | 0.000 |
| [4] | Mair J. Biochemistry of B-type natriuretic peptide—where are we now?[J]. Clin Chem Lab Med, 2008, 46(11): 1507-1514. |
| [5] |
Breidthardt T, Kalbermatter S, Socrates T, et al. Increasing B-type natriuretic peptide levels predict mortality in unselected haemodialysis patients[J]. Eur J Heart Fail, 2011, 13: 860-867.
doi: 10.1093/eurjhf/hfr057 pmid: 21628312 |
| [6] |
Winkler K, Wanner C, Drechsler C, et al. Change in N-terminal-pro-B-type-natriuretic-peptide and the risk of sudden death, stroke, myocardial infarction, and all-cause mortality in diabetic dialysis patients[J]. Eur Heart J, 2008, 29: 2092-2099.
doi: 10.1093/eurheartj/ehn278 pmid: 18617483 |
| [7] |
Gutiérrez OM, Tamez H, Bhan I, et al. N-terminal pro-B-type natriuretic peptide (NT-proBNP) concentrations in hemodialysis patients: prognostic value of baseline and follow-up measurements[J]. Clin Chem, 2008, 54(8): 1339-1348.
doi: 10.1373/clinchem.2007.101691 pmid: 18539645 |
| [8] |
Paniagua R, Amato D, Mujais S, et al. Predictive value of brain natriuretic peptides in patients on peritoneal dialysis[J]. Clin J Am Soc Nephrol, 2008, 3(2): 407-415.
doi: 10.2215/CJN.03820907 URL |
| [9] |
Plum J, Schoenicke G, Kleophas W, et al. Comparison of body fluid distribution between chronic haemodialysis and peritoneal dialysis patients as assessed by biophysical and biochemical methods[J]. Nephrol Dial Transplant, 2001, 16(12):2378-2385.
doi: 10.1093/ndt/16.12.2378 URL |
| [10] | van den Wall Bake AW, Kooman JP, Lange JM, et al. Adequacy of peritoneal dialysis and the importance of preserving residual renal function[J]. Nephrol Dial Transplant, 2006, 21 Suppl 2: ii34-ii37. |
| [11] |
Cheng LT, Chen W, Tang W, et al. Residual renal function and volume control in peritoneal dialysis patients[J]. Nephron Clin Pract, 2006, 104(1): c47-c54.
doi: 10.1159/000093670 URL |
| [12] |
Devolder I, Verleysen A, Vijt D, et al. Body composition, hydration, and related parameters in hemodialysis versus peritoneal dialysis patients[J]. Perit Dial Int, 2010, 30(2): 208-214.
doi: 10.3747/pdi.2008.00284 URL |
| [13] |
Wizemann V, Wabel P, Chamney P, et al. The mortality risk of overhydration in haemodialysis patients[J]. Nephrol Dial Transplant, 2009, 24(5): 1574-1579.
doi: 10.1093/ndt/gfn707 URL |
| [14] |
Passauer J, Petrov H, Schleser A, et al. Evaluation of clinical dry weight assessment in haemodialysis patients using bioimpedance spectroscopy[J]. Nephrol Dial Transplant, 2010, 25(2): 545-551.
doi: 10.1093/ndt/gfp517 URL |
| [15] |
Lopot F, Nejedly B, Novotná H, et al. Age-related extracellular to total body water volume ratio (Ecv/TBW)—can it be used for "dry weight" determination in dialysis patients?[J]. Int J Artif Organs, 2002, 25(8): 762-769.
pmid: 12296460 |
| [16] |
Yilmaz Z, Yildirim Y, Oto F, et al. Evaluation of volume overload by bioelectrical impedance analysis, NT-proBNP and inferior vena cava diameter in patients with stage 3&4 and 5 chronic kidney disease[J]. Ren Fail, 2014, 36(4): 495-501.
doi: 10.3109/0886022X.2013.875815 URL |
| [17] |
Park WY, Park S, Kim YW, et al. Clinical efficacy of biomarkers for evaluation of volume status in dialysis patients[J]. Medicine (Baltimore), 2020, 99(31): e21460.
doi: 10.1097/MD.0000000000021460 URL |
| [18] |
Vickery S, Price CP, John RI, et al. B-type natriuretic peptide(BNP) and amino-terminal proBNP in patients with CKD: relationship to renal function and left ventricular hypertrophy[J]. Am J Kidney Dis, 2005, 46(4): 610-620.
doi: 10.1053/j.ajkd.2005.06.017 pmid: 16183415 |
| [19] |
Palmer SC, Yandle TG, Nicholls MG, et al. Regional clearance of amino-terminal pro-brain natriuretic peptide from human plasma[J]. Eur J Heart Fail, 2009, 11(9): 832-839.
doi: 10.1093/eurjhf/hfp099 pmid: 19605456 |
| [20] |
Jacobs LH, van de Kerkhof JJ, Mingels AM, et al. Inflammation, overhydration and cardiac biomarkers in haemodialysis patients: a longitudinal study[J]. Nephrol Dial Transplant, 2010, 25(1): 243-248.
doi: 10.1093/ndt/gfp417 URL |
| [21] |
Booth J, Pinney J, Davenport A. N-terminal proBNP—marker of cardiac dysfunction, fluid overload, or malnutrition in hemodialysis patients?[J]. Clin J Am Soc Nephrol, 2010, 5(6): 1036-1040.
doi: 10.2215/CJN.09001209 URL |
| [22] | Ridao N, Luño J, García de Vinuesa S, et al. Prevalence of hypertension in renal disease[J]. Nephrol Dial Transplant, 2001, 16 Suppl 1: 70-73. |
| [23] | Alvarez-Lara MA, Martín-Malo A, Espinosa M, et al. Blood pressure and body water distribution in chronic renal failure patients[J]. Nephrol Dial Transplant, 2001, 16 Suppl 1: 94-97. |
| [24] |
Celik G, Kara I, Yilmaz M, et al. The relationship between bioimpedance analysis, haemodynamic parameters of haemodialysis, biochemical parameters and dry weight[J]. J Int Med Res, 2011, 39(6): 2421-2428.
pmid: 22289562 |
| [25] |
Jang M, Kim WH, Lee JH, et al. Numerical expression of volume status using the bioimpedance ratio in continuous ambulatory peritoneal dialysis patients[J]. Kidney Res Clin Pract, 2017, 36(3): 290-295.
doi: 10.23876/j.krcp.2017.36.3.290 pmid: 28904881 |
| [26] |
Flythe JE, Chang TI, Gallagher MP, et al. Blood pressure and volume management in dialysis[J]. Kidney Int, 2020, 97(5): 861-876.
doi: 10.1016/j.kint.2020.01.046 URL |
| [27] |
DeFilippi C, van Kimmenade RR, Pinto YM. Amino-terminal pro-B-type natriuretic peptide testing in renal disease[J]. Am J Cardiol, 2008, 101(3A): 82-88.
doi: 10.1016/j.amjcard.2007.11.029 pmid: 18243865 |
| [1] |
Zoccali C, Moissl U, Chazot C, et al. Chronic fluid overload and mortality in ESRD[J]. J Am Soc Nephrol, 2017, 28: 2491-2497.
doi: 10.1681/ASN.2016121341 pmid: 28473637 |
| [2] |
Wang AY, Brimble KS, Brunier G, et al. ISPD cardiovascular and metabolic guidelines in adult peritoneal dialysis patients part Ⅰ-assessment and management of various cardiovascular risk factors[J]. Perit Dial Int, 2015, 35: 379-387.
doi: 10.3747/pdi.2014.00279 URL |
| [3] |
Wizemann V, Wabel P, Chamney P, et al. The mortality risk of overhydration in haemodialysis patients[J]. Nephrol Dial Transplant, 2009, 24(5): 1574-1579.
doi: 10.1093/ndt/gfn707 URL |
| [28] |
Zoccali C, Mallamaci F, Benedetto FA, et al. Cardiac natriuretic peptides are related to left ventricular mass and function and predict mortality in dialysis patients[J]. J Am Soc Nephrol, 2001, 12(7): 1508-1515.
doi: 10.1681/ASN.V1271508 pmid: 11423580 |
| [1] | 王朝俊, 俞灵, 王恒杰, 任红, 史曼曼, 郑洪, 马毓华, 徐天. 超声引导下腹横肌平面联合腹直肌鞘神经阻滞在腹膜透析置管术中的应用研究[J]. 内科理论与实践, 2023, 18(03): 152-156. |
| [2] | 欧阳彦, 陈孜瑾, 章倩莹, 陈晓农, 谢静远, 任红, 张文, 王伟铭. 慢性肾脏病人群的新型冠状病毒感染临床诊治建议(瑞金医院2023版)[J]. 内科理论与实践, 2023, 18(01): 28-33. |
| [3] | 桂燕萍, 陈晔芬, 施仲伟, 许燕. 超声心动图右室面积变化分数筛查左心室射血分数降低的心力衰竭患者心脏同步性研究[J]. 诊断学理论与实践, 2022, 21(03): 331-335. |
| [4] | 王晨琛, 方跃华, 施仲伟, 屈雪蒸. 25例主动脉瓣成形术后一年的超声心动图评价[J]. 诊断学理论与实践, 2022, 21(03): 395-398. |
| [5] | 黄晓敏, 章倩莹, 杨俪, 崔岩, 徐天, 王子秋, 王朝晖, 任红, 张春燕. 腹膜透析患者跌倒发生的现况调查[J]. 内科理论与实践, 2022, 17(03): 248-252. |
| [6] | 陈涛, 徐煜, 付学良, 袁志青, 花荣. 持续性非卧床腹膜透析病人并发腹股沟疝的外科治疗[J]. 外科理论与实践, 2021, 26(5): 425-429. |
| [7] | 汤荟, 张春. 新型冠状病毒病与肾脏替代治疗[J]. 内科理论与实践, 2021, 16(01): 4-9. |
| [8] | 王晨琛, 杨文波, 华玮, 陈晔芬, 苏秀秀, 龚俊世, 方跃华. 左心耳解剖形态、功能与非瓣膜性心房颤动患者脑卒中发生风险的相关性研究[J]. 诊断学理论与实践, 2020, 19(02): 151-156. |
| [9] | 张玉奇, 鲍圣芳. 血管环的产前超声心动图诊断及预后评估[J]. 诊断学理论与实践, 2019, 18(05): 487-490. |
| [10] | 张春燕, 汪知玉, 杨俪, 黄晓敏, 施咏梅, 王朝晖, 任红, 陈晓农,. “学校式”磷教育在腹膜透析高磷患者中的运用[J]. 内科理论与实践, 2018, 13(04): 227-230. |
| [11] | 晏焕青, 王鹤定, 朱彤莹,. 腹膜透析相关性腹膜炎预后的危险因素研究[J]. 内科理论与实践, 2018, 13(03): 165-169. |
| [12] | 陈晔芬, 施仲伟. 单心动周期实时三维超声心动图评价扩张型心肌病左右心室收缩功能及左心室同步性[J]. 诊断学理论与实践, 2017, 16(03): 292-296. |
| [13] | 施仲伟. 2016年欧美《超声心动图评价左心室舒张功能建议》新指南极大简化超声心动图评价左心室舒张功能[J]. 诊断学理论与实践, 2017, 16(01): 38-41. |
| [14] | 王鸿珍, 徐文彬,. 慢性心力衰竭患者血清和肽素水平与心功能的关系[J]. 内科理论与实践, 2016, 11(04): 230-233. |
| [15] | 华玮, 许燕, 施仲伟,. 超声心动图诊断主动脉窦瘤破裂的准确性评价[J]. 诊断学理论与实践, 2016, 15(03): 244-247. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||