内科理论与实践 ›› 2025, Vol. 20 ›› Issue (03): 191-197.doi: 10.16138/j.1673-6087.2025.03.02
田小芳1,2, 刘丽萍2, 袁立英1,2, 任红1, 王朝晖1( ), 史浩1()
), 史浩1()
收稿日期:2025-03-24
出版日期:2025-06-28
发布日期:2025-09-01
通讯作者:
王朝晖,史浩
E-mail:wzhaohui2001@163.com;shihaohp@163.com
基金资助:
TIAN Xiaofang1,2, LIU Liping2, YUAN Liying1,2, REN Hong1, WANG Zhaohui1(), SHI Hao1()
Received:2025-03-24
Online:2025-06-28
Published:2025-09-01
Contact:
WANG Zhaohui, SHI Hao
E-mail:wzhaohui2001@163.com;shihaohp@163.com
摘要:
目的:通过分析1例伴双克隆副蛋白血症的轻重链型肾淀粉样变患者诊疗情况,结合文献复习,探讨非传统免疫球蛋白相关肾淀粉样变的诊疗思路。 方法:收集和回顾1例在上海交通大学医学院附属瑞金医院肾脏科诊断为双克隆副蛋白血症的肾淀粉样变患者2021年至2024年间长期诊治随访的临床资料,并复习国内外相关文献。 结果:72岁男性,以泡沫尿、颜面及双下肢水肿为主要症状,血清中检出M蛋白为IgM-λ型和IgA-λ型,肾活检为轻重链型肾淀粉样变(IgA-λ),心脏无明显受累,骨髓中致病克隆为CD38+的B淋巴细胞,骨髓病理未检出MYD88基因L265P突变,无淋巴结肿大或结外病灶累及,考虑血液基础疾病为B淋巴细胞增殖性疾病。在前期利妥昔单抗为基础的方案治疗后,调整为靶向CD38的达雷妥尤单抗联合来那度胺,患者快速获得血液学完全缓解和肾脏反应,并在后续治疗中达到肾脏完全缓解。文献复习显示,双克隆副蛋白血症伴肾淀粉样变见于少数个案报道,伴轻重链型肾淀粉样变仅1例。B细胞或淋巴浆细胞克隆致病的淀粉样变中,基于利妥昔单抗的方案是主要治疗手段,但血液学和器官反应均不理想,达雷妥尤单抗联合用药方案可能对CD38+的克隆性B细胞致病者有效。 结论:目前双克隆副蛋白淀粉样变尚无诊疗共识或指南,准确判断致病性单克隆细胞、确定治疗靶点、制定个体化联合用药方案,有助于快速获得血液和器官的更深度缓解。
中图分类号:
田小芳, 刘丽萍, 袁立英, 任红, 王朝晖, 史浩. 双克隆副蛋白血症与轻重链型肾淀粉样变1例及文献复习[J]. 内科理论与实践, 2025, 20(03): 191-197.
TIAN Xiaofang, LIU Liping, YUAN Liying, REN Hong, WANG Zhaohui, SHI Hao. Heavy and light chain renal amyloidosis with biclonal paraproteinemia: a case study and literature review[J]. Journal of Internal Medicine Concepts & Practice, 2025, 20(03): 191-197.

图1
肾活检病理图谱 A:光镜,刚果红染色阳性(系膜区、肾小管基底膜);B:IgA石蜡荧光,系膜区及肾小球基底膜IgA++(×400,标尺20 μm);C:IgM石蜡荧光,IgM-(×400,标尺20 μm);D:轻链κ石蜡荧光:κ-(×400,标尺20 μm);E:轻链λ石蜡荧光,λ++(×400,标尺20 μm);F:电镜,无序排列的纤维状物质在系膜区沉积,直径7~12 nm(×25 000,标尺500 nm)。
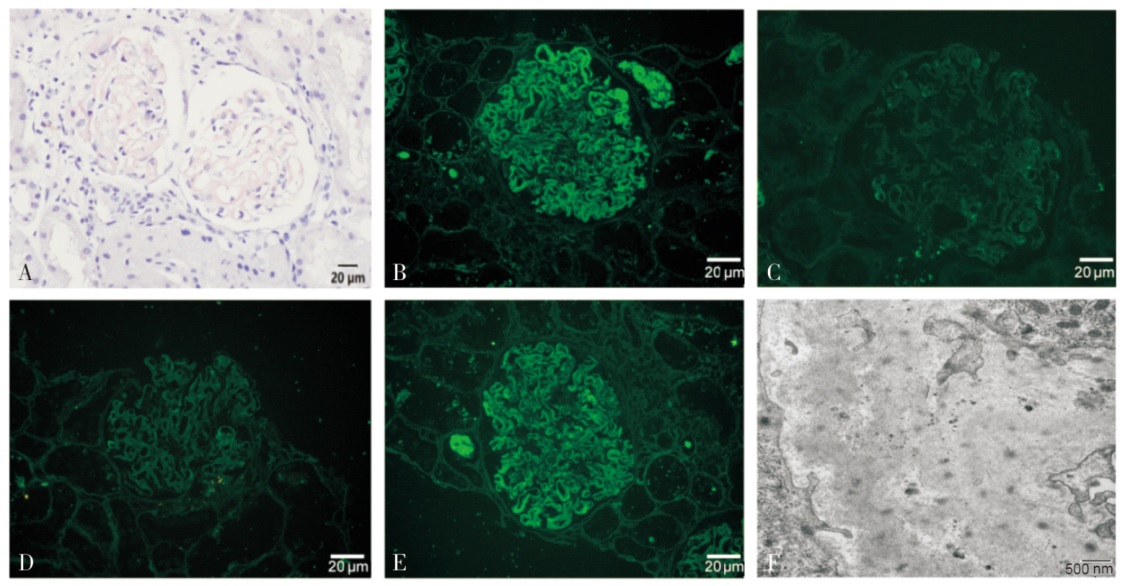
图2
诊疗过程中患者血FLC λ、κ/λ及dFLC变化
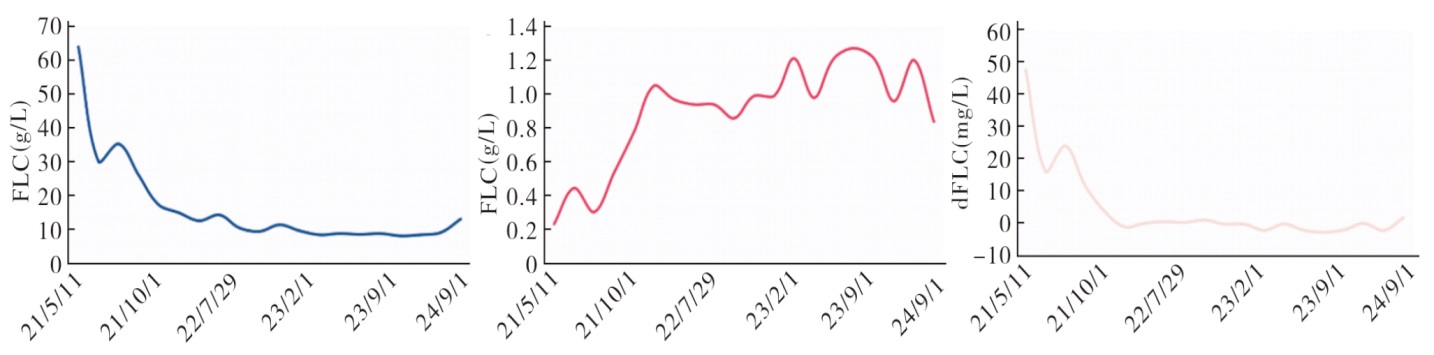

图3
诊疗过程中患者24 h尿蛋白定量、血白蛋白及Scr变化
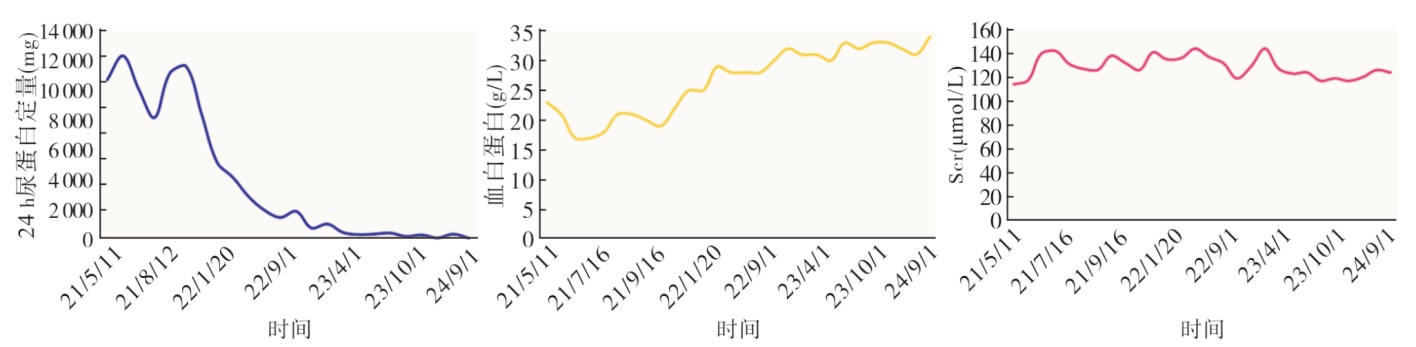
表1
双克隆副蛋白血症的AL淀粉样变(不合并MM)患者临床特征及治疗
| 项目 | Julien等[ | Bouvet等[ | Pace等[ | Yan等[ | Dhaliwal等[ |
|---|---|---|---|---|---|
| 年龄(岁) | 59 | 51 | 80 | 46 | 68 |
| 性别 | 男性 | 男性 | 男性 | 男性 | 男性 |
| 血M蛋白类型 | IgM κ/IgG λ | IgG κ/IgA λ | IgG κ/IgA λ | IgA κ/IgG κ | IgM κ/IgM λ |
| 骨髓涂片或流式细胞检测 | 未报道 | 浆细胞3.60% | 浆细胞4.80% | 流式:克隆浆细胞0.86% | 流式:克隆B细胞13.00% |
| 累及器官 | 肾脏、周围神经 | 肾、肠道 | 心脏、肾脏、周围神经、肠道 | 支气管黏膜 | 肾脏、心脏 |
| 治疗 | 未报道 | MP方案 | MP方案 | CyBorD方案 | BDR方案后调整为Dara |
| [1] |
Wechalekar AD, Gillmore JD, Hawkins PN. Systemic amyloidosis[J]. Lancet, 2016, 387(10038):2641-2654.
doi: S0140-6736(15)01274-X pmid: 26719234 |
| [2] | Fotiou D, Dimopoulos MA, Kastritis E. Systemic AL amyloidosis: current approaches to diagnosis and management[J]. Hemasphere, 2020, 4(4):e454. |
| [3] |
Palladini G, Dispenzieri A, Gertz MA, et al. New criteria for response to treatment in immunoglobulin light chain amyloidosis based on free light chain measurement and cardiac biomarkers: impact on survival outcomes[J]. J Clin Oncol, 2012, 30(36):4541-4549.
doi: 10.1200/JCO.2011.37.7614 pmid: 23091105 |
| [4] | 中国系统性轻链型淀粉样变性协作组, 国家肾脏疾病临床医学研究中心, 国家血液系统疾病临床医学研究中心. 系统性轻链型淀粉样变性诊断和治疗指南(2021年修订)[J]. 中华医学杂志, 2021, 101(22):1646-1656. |
| [5] |
Palladini G, Hegenbart U, Milani P, et al. A staging system for renal outcome and early markers of renal response to chemotherapy in AL amyloidosis[J]. Blood, 2014, 124(15):2325-2332.
doi: 10.1182/blood-2014-04-570010 pmid: 25115890 |
| [6] |
Lolin YI, Chow J, Wickham NW. Monoclonal gammopathy of unknown significance and malignant paraproteinemia in Hong Kong[J]. Am J Clin Pathol, 1996, 106(4):449-456.
pmid: 8853031 |
| [7] |
Mullikin TC, Rajkumar SV, Dispenzieri A, et al. Clinical characteristics and outcomes in biclonal gammopathies[J]. Am J Hematol, 2016, 91(5):473-475.
doi: 10.1002/ajh.24319 pmid: 26840395 |
| [8] |
Spicka I, Merta M, Cieslar P, et al. [Renal impairment in monoclonal gammapathies. clinical study][J]. Cas Lek Cesk, 1995, 134(15):478-481.
pmid: 7585865 |
| [9] | Yan W, Li P, Wu C, et al. Case Report: Management of primary tracheobronchial light chain amyloidosis in a patient with biclonal cammopathy using a systemic bortezomib-based regimen[J]. Front Med (Lausanne), 2021, 8:728561. |
| [10] |
Coen M, Bornand A, Samii K, et al. Gastrointestinal amyloidosis in biclonal gammopathy[J]. Clin Lymphoma Myeloma Leuk, 2021, 21(7):e606-e610.
doi: 10.1016/j.clml.2021.02.015 pmid: 33785295 |
| [11] | Stammler F. Haemorrhagic diathesis as an early symptom of systemic amyloidosis[J]. Dtsch Med Wochenschr, 2006, 131(1-2):17-21. |
| [12] |
Julien J, Vital C, Vallat JM, et al. IgM demyelinative neuropathy with amyloidosis and biclonal gammopathy[J]. Ann Neurol, 1984, 15(4):395-399.
pmid: 6430211 |
| [13] |
Bouvet JP, Delrieu F. Polyarteritis nodosa associated with biclonal gammopathy of two-cell line origin and amyloidosis[J]. J Rheumatol, 1985, 12(1):168-170.
pmid: 2858589 |
| [14] |
Silver MM, Hearn SA, Walton JC et al. Immunogold quantitation of immunoglobulin light chains in renal amyloidosis and kappa light chain nephropathy[J]. Am J Pathol, 1990, 136(5):997-1007.
pmid: 1693473 |
| [15] |
Pace F, Gubitosi G, Giorgi A, et al. Idiopathic AL amyloidosis and biclonal paraproteinemia: a case report and review of the literature[J]. Amyloid, 2001, 8(3):215-219.
pmid: 11676298 |
| [16] | Dhaliwal A, Tripathi A, Ravi S. A case of μ heavy and λ light chain amyloidosis in a patient with bi-clonal (IgM κ and λ) gammopathy treated with daratumumab[J]. Cureus, 2024, 16(3):e56994. |
| [17] | Ravichandran S, Lachmann HJ, Wechalekar AD. Epidemiologic and survival trends in amyloidosis, 1987-2019[J]. N Engl J Med, 2020, 382(16):1567-1568. |
| [18] |
Leung N, Bridoux F, Hutchison CA, et al. Monoclonal gammopathy of renal significance: when MGUS is no longer undetermined or insignificant[J]. Blood, 2012, 120(22):4292-4295.
doi: 10.1182/blood-2012-07-445304 pmid: 23047823 |
| [19] |
Kyle RA, Robinson RA, Katzmann JA. The clinical aspects of biclonal gammopathies[J]. Am J Med, 1981, 71(6):999-1008.
pmid: 6797297 |
| [20] |
Palladini G, Russo P, Bosoni T, et al. Identification of amyloidogenic light chains requires the combination of serum-free light chain assay with immunofixation of serum and urine[J]. Clin Chem, 2009, 55(3):499-504.
doi: 10.1373/clinchem.2008.117143 pmid: 19131635 |
| [21] |
Clausen J, Christensen HE. Paraproteins and acid mucopolysaccharides in primary amyloidosis. biochemical and histologic studies of four human cases of primary amyloidosis[J]. Acta Pathol Microbiol Scand, 1964, 60:493-511.
pmid: 14154712 |
| [22] | Wechalekar AD, Cibeira MT, Gibbs SD, et al. Guidelines for non-transplant chemotherapy for treatment of systemic AL amyloidosis: EHA-ISA Working Group[J]. Amyloid, 2023, 30(1):3-17. |
| [23] |
Sachchithanantham S, Roussel M, Palladini G, et al. European collaborative study defining clinical profile outcomes and novel prognostic criteria in monoclonal immunoglobulin M-related light chain amyloidosis[J]. J Clin Oncol, 2016, 34(17):2037-2045.
doi: 10.1200/JCO.2015.63.3123 pmid: 27114592 |
| [24] | Paulus A, Manna A, Akhtar S, et al. Targeting CD38 with daratumumab is lethal to Waldenström macroglobulinaemia cells[J]. Br J Haematol, 2018, 183(2):196-211. |
| [25] |
Castillo JJ, Libby EN, Ansell SM, et al. Multicenter phase 2 study of daratumumab monotherapy in patients with previously treated Waldenström macroglobulinemia[J]. Blood Adv, 2020, 4(20):5089-5092.
doi: 10.1182/bloodadvances.2020003087 pmid: 33085756 |
| [26] | Kumar SK, Callander NS, Adekola K, et al. Systemic Light Chain Amyloidosis, Version 2.2023, NCCN Clinical Practice Guidelines in Oncology[J]. J Natl Compr Canc Netw, 2023, 21(1):67-81. |
| [1] | 徐丽梨, 胡晓帆, 李灏, 王伟铭. 利妥昔单抗治疗PLA2R阴性的原发性膜性肾病患者疗效预测相关指标的研究[J]. 诊断学理论与实践, 2025, 24(03): 279-285. |
| [2] | 阮怡霖, 徐天, 冯晓蓓, 徐静, 史浩, 任红. 肾病综合征患者免疫抑制治疗继发侵袭性肺曲霉病1例[J]. 内科理论与实践, 2024, 19(05): 318-321. |
| [3] | 周芮, 吴涛, 薛锋, 田红娟, 刘文慧, 毛东锋. 达雷妥尤单抗治疗复发/难治性多发性骨髓瘤疗效及安全性分析[J]. 内科理论与实践, 2023, 18(05): 348-351. |
| [4] | 潘萌, 王晶莹. 中国天疱疮的诊治现状及思考[J]. 诊断学理论与实践, 2023, 22(03): 209-214. |
| [5] | 程毅敏, 庄衍, 杭海芳, 窦红菊,. 探讨利妥昔单抗联合CHOP方案治疗弥漫大B细胞淋巴瘤的临床疗效[J]. 内科理论与实践, 2019, 14(05): 317-318. |
| [6] | 张薇, 冯俊,. 华氏巨球蛋白血症的诊断与治疗[J]. 内科理论与实践, 2017, 12(05): 309-313. |
| [7] | 魏玉珠, 吴涛, 毛军峰, 胡晓燕, 武慧敏, 白海, 王存邦. 以颈椎病变首诊的弥漫大B细胞淋巴瘤一例报道[J]. 诊断学理论与实践, 2017, 16(04): 432-433. |
| [8] | 徐星萍, 孙以隽, 阎骅,. 套细胞淋巴瘤长期生存1例[J]. 内科理论与实践, 2013, 8(03): 215-216. |
| [9] | 蔡铭慈, 赵维莅,. 利妥昔单抗在血液疾病中的临床应用[J]. 内科理论与实践, 2012, 7(02): 137-142. |
| [10] | 王文方, 徐子真, 王爱华, 诸江, 李军民,. 利妥昔单抗和RAD001对弥漫大B细胞株SUDHL-4和DB细胞增殖和凋亡的影响[J]. 诊断学理论与实践, 2012, 11(02): 130-135. |
| [11] | 黄洪晖,. 晚期滤泡性淋巴瘤的个体化治疗策略[J]. 内科理论与实践, 2011, 6(01): 22-29. |
| [12] | 阎骅, 沈志祥,. 非霍奇金淋巴瘤靶点治疗及其临床应用前景[J]. 内科理论与实践, 2009, 4(01): 18-21. |
| [13] | 樊贞瑜, 叶霜, 陆瑜,. 利妥昔单抗治疗系统性红斑狼疮的研究进展[J]. 内科理论与实践, 2008, 3(05): 354-357. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||