内科理论与实践 ›› 2025, Vol. 20 ›› Issue (04): 276-281.doi: 10.16138/j.1673-6087.2025.04.03
孙杰1, 谢洁1, 马宏昆2, 刘宝莲1, 陈学英1, 黄文洁1, 何水林1, 陈孜瑾2, 张文2( )
)
收稿日期:2024-07-31
出版日期:2025-07-31
发布日期:2025-10-27
通讯作者:
张 文 E-mail: 基金资助:
SUN Jie1, XIE Jie1, MA Hongkun2, LIU Baolian1, CHEN Xueying1, HUANG Wenjie1, HE Shuilin1, CHEN Zijin2, ZHANG Wen2()
Received:2024-07-31
Online:2025-07-31
Published:2025-10-27
摘要:
目的:对比肾动脉超声血流动力学参数与非增强磁共振在评估肾动脉狭窄及解剖异常中的临床价值。方法:选取149例慢性肾脏病(chronic kidney disease, CKD)患者,通过肾动脉非增强磁共振血管成像(non-contrast enhanced magnetic resonance angiography, NCE-MRA)评估肾动脉狭窄及解剖变异,彩色多普勒超声检测肾动脉各段血流动力学参数,肾功能评估采用核素肾动态显像和CKD流行病学合作研究(Chronic Kidney Disease Epidemiology Collaboration, CKD-EPI)方程式计算估算的肾小球滤过率(estimated glomerular filtration rate, eGFR)2种方式。结果:149例患者CKD分期1期17例(11.4%)、2期39例(26.2%)、3期44例(29.5%)、4期17例(11.4%)、5期32例(21.5%)。起始段肾动脉狭窄患者阻力指数(resistance index, RI)明显高于无狭窄患者(P=0.000),收缩期峰值速度(peak systolic velocity,PSV)无统计学差异(P=0.443);有无中段狭窄患者2组间PSV及RI差异均无统计学意义(P=0.190、P=0.088)。解剖变异组起始段及中段的PSV和RI与无变异组差异均无统计学意义(P>0.05)。肾动脉起始段无狭窄侧eGFR明显高于狭窄侧(Z=2.980,P=0.029),中段无狭窄侧eGFR明显高于狭窄侧(Z=4.025,P=0.001),解剖变异侧与非变异侧eGFR差异无统计学意义(Z=0.579,P=0.550)。结论:彩色多普勒超声PSV和RI对肾动脉起始部狭窄诊断价值高于肾动脉中段狭窄,对肾动脉解剖学变异无诊断价值。无论是肾动脉起始段还是中段狭窄,均导致同侧eGFR下降,肾动脉解剖变异则不影响同侧肾脏eGFR。
孙杰, 谢洁, 马宏昆, 刘宝莲, 陈学英, 黄文洁, 何水林, 陈孜瑾, 张文. 肾动脉超声血流动力学参数与非增强磁共振评估肾动脉狭窄及解剖异常的临床应用[J]. 内科理论与实践, 2025, 20(04): 276-281.
SUN Jie, XIE Jie, MA Hongkun, LIU Baolian, CHEN Xueying, HUANG Wenjie, HE Shuilin, CHEN Zijin, ZHANG Wen. Clinical application of renal artery ultrasound monitoring hemodynamic parameters and non-contrast-enhanced magnetic resonance angiography in evaluation of renal artery stenosis and anatomic abnormalities[J]. Journal of Internal Medicine Concepts & Practice, 2025, 20(04): 276-281.
表1
患者的基线特征与肾动脉病变分布[n(%)/$\bar{x} \pm s$]
| 项目 | 整体人群 | RAS | 肾动脉变异 | ||
|---|---|---|---|---|---|
| 单侧 | 双侧 | 单侧 | 双侧 | ||
| 总例数[n(%)] | 149(100.0) | 32(21.5) | 11(7.4) | 52(34.9) | 11(7.4) |
| 男性[n(%)] | 108(72.5) | 29(19.5) | 5(3.4) | 42(28.1) | 9(6.0) |
| 年龄(岁) | 57.4±15.6 | 61.6±13.8 | 76.2±8.6 | 53.5±15.4 | 54.2±18.1 |
| 原发病[n(%)] | |||||
| 慢性肾炎 | 51(34.2) | 10(6.7) | 2(1.3) | 12(8.1) | 2(1.3) |
| 糖尿病肾病 | 31(20.8) | 7(4.7) | 3(2.0) | 17(11.4) | 3(2.0) |
| 高血压肾病 | 34(22.8) | 12(8.1) | 4(2.7) | 11(7.4) | 3(2.0) |
| 其他原发病 | 33(22.2) | 2(1.3) | 2(1.3) | 12(8.1) | 3(2.0) |
| 合并症[n(%)] | |||||
| 高血压 | 125(83.9) | 28(18.8) | 10(6.7) | 43(28.9) | 6(4.0) |
| 糖尿病 | 52(34.9) | 14(9.4) | 4(2.7) | 20(13.4) | 5(3.4) |
| eGFR [mL/(min·1.73 m2)] | 47.98±31.22 | 41.68±26.10 | 39.73±23.53 | 43.90±31.47 | 62.35±32.82 |
| GFR *(mL/min)(n=99) | 48.09±23.94 | 39.29±15.93 | 34.42±13.83 | 49.28±26.17 | 46.17±27.61 |

图1
NCE-MRA评估肾动脉 A:双侧肾动脉主干及远端未见异常;B:右侧肾动脉近段管腔重度狭窄;C:左侧副肾动脉;D:右侧肾动脉提前分支。
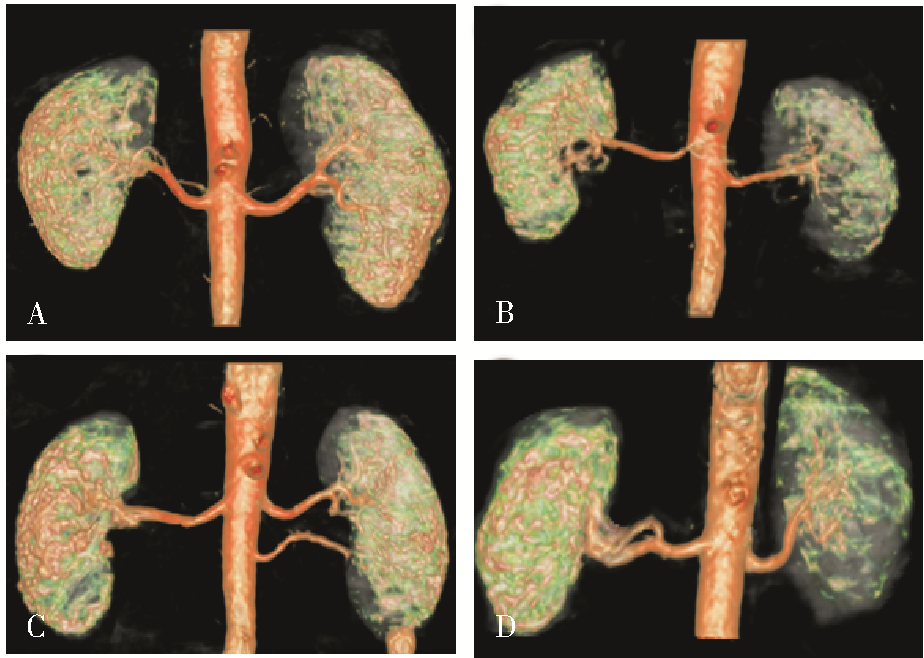
表2
不同部位狭窄RAS患者超声参数比较[M(Q1,Q3)/$\bar{x} \pm s$]
| 参数 | 肾动脉起始段无狭窄 (n=263) | 肾动脉起始段狭窄 (n=35) | t/Z | P | 肾动脉中段无狭窄 (n=277) | 肾动脉中段狭窄 (n=21) | t/Z | P |
|---|---|---|---|---|---|---|---|---|
| PSV(cm/s) | 74(54,90) | 53.5(42,78) | 0.767 | 0.443 | 41(33,50) | 40(33,44) | 1.310 | 0.190 |
| RI | 0.689±0.05 | 0.758±0.016 | -4.252 | 0.000 | 0.644±0.006 | 0.678±0.018 | -1.715 | 0.088 |
表3
肾动脉解剖变异与非变异患者超声参数比较[M(Q1,Q3)/$\bar{x} \pm s$]
| 参数 | 无副肾动脉+提前分支 (n=224) | 有副肾动脉+提前分支 (n=74) | t/Z | P |
|---|---|---|---|---|
| 肾动脉起始段PSV(cm/s) | 71.5(53,90) | 71(48,90) | 0.585 | 0.559 |
| 肾动脉起始段RI | 0.701±0.006 | 0.687±0.009 | 1.232 | 0.219 |
| 肾动脉中段PSV(cm/s) | 40.5(33,50) | 41(31.5,49) | -0.616 | 0.538 |
| 肾动脉中段RI | 0.648±0.006 | 0.644±0.010 | 0.366 | 0.715 |
表4
肾动脉起始段及中段(RI和PSV) 与GFR 的相关性
| 肾动脉 | r | P |
|---|---|---|
| 起始段RI | -0.446 | 0.000 |
| 起始段PSV | 0.302 | 0.000 |
| 中段RI | -0.294 | 0.000 |
| 中段PSV | 0.344 | 0.000 |
| [1] |
Chai JW, Lee W, Yin YH, et al. CT angiography for living kidney donors: accuracy, cause of misinterpretation and prevalence of variation[J]. Korean J Radiol, 2008, 9(4):333-339.
doi: 10.3348/kjr.2008.9.4.333 pmid: 18682671 |
| [2] | 郭震华, 那彦群. 实用泌尿外科学[M]. 2版. 北京: 人民卫生出版社,2014:112. |
| [3] |
AbuRahma AF, Yacoub M. Renal imaging: duplex ultrasound, computed tomography angiography, magnetic resonance angiography, and angiography[J]. Semin Vasc Surg, 2013, 26(4):134-143.
doi: 10.1053/j.semvascsurg.2014.06.001 pmid: 25220318 |
| [4] |
Herborn CU, Watkins DM, Runge VM, et al. Renal arteries: comparison of steady-state free precession MR angiography and contrast-enhanced MR angiography[J]. Radiology, 2006, 239(1):263-268.
doi: 10.1148/radiol.2383050058 pmid: 16493015 |
| [5] |
Holden A, Smith A, Dukes P, et al. Assessment of 100 live potential renal donors for laparoscopic nephrectomy with multi-detector row helical CT[J]. Radiology, 2005, 237(3):973-980.
pmid: 16304115 |
| [6] |
Bordei P, Sapte E, Iliescu D. Double renal arteries originating from the aorta[J]. Surg Radiol Anat, 2004, 26(6):474-479.
pmid: 15378279 |
| [7] |
Hänninen EL, Denecke T, Stelter L, et al. Preoperative evaluation of living kidney donors using multirow detector computed tomography: comparison with digital subtraction angiography and intraoperative findings[J]. Transpl Int, 2005, 18(10):1134-1141.
pmid: 16162099 |
| [8] | Gupta A, Tello R. Accessory renal arteries are not related to hypertension risk: a review of MR angiography data[J]. AJR Am J Roentgenol, 2004, 182(6):1521-1524. |
| [9] | Shen J, Lyu L, Wu X, et al. Correlation between renal artery anatomy and hypertension: a retrospective analysis of 3000 patients[J]. Evid Based Complement Alternat Med, 2021,2021:9957361. |
| [10] | Kang K, Ma Y, Jia C, et al. Relationship between accessory renal artery and clinical characteristics of middle-aged patients with primary hypertension[J]. Int J Hypertens, 2020,2020:7109502. |
| [11] |
刘方韬, 齐晓凤, 徐学勤, 等. 非增强磁共振血管成像在肾动脉狭窄评估方面的价值研究[J]. 诊断学理论与实践, 2019, 18(1):72-76.
doi: 10.16150/j.1671-2870.2019.01.014 |
| [12] |
Zhang LJ, Peng J, Wen J, et al. Non-contrast-enhanced magnetic resonance angiography: a reliable clinical tool for evaluating transplant renal artery stenosis[J]. Eur Radiol, 2018, 28(10):4195-4204.
doi: 10.1007/s00330-018-5413-3 pmid: 29666993 |
| [13] |
Bley TA, François CJ, Schiebler ML, et al. Non-contrast-enhanced MRA of renal artery stenosis: validation against DSA in a porcine model[J]. Eur Radiol, 2016, 26(2):547-555.
doi: 10.1007/s00330-015-3833-x pmid: 26017736 |
| [14] | Fananapazir G, McGahan JP, Corwin MT, et al. Screening for transplant renal artery stenosis: ultrasound-based stenosis probability stratification[J]. AJR Am J Roentgenol, 2017, 209(5):1064-1073. |
| [15] |
Granata A, Fiorini F, Andrulli S, et al. Doppler ultrasound and renal artery stenosis: an overview[J]. J Ultrasound, 2009, 12(4):133-143.
doi: 10.1016/j.jus.2009.09.006 pmid: 23397022 |
| [16] |
van Twist DJ, Houben AJ, de Haan MW, et al. Pathophysiological differences between multifocal fibromuscular dysplasia and atherosclerotic renal artery stenosis[J]. J Hypertens, 2017, 35(4):845-852.
doi: 10.1097/HJH.0000000000001243 pmid: 28060190 |
| [17] |
Lo R, Donaldson C. Vessel tortuosity causing false positives in detecting renal artery stenosis on doppler ultrasound[J]. Ultrasound Q, 2013, 29(1):47-50.
doi: 10.1097/RUQ.0b013e3182817b57 pmid: 23370780 |
| [18] | Kendrick J, Chonchol M. Renal artery stenosis and chronic ischemic nephropathy: epidemiology and diagnosis[J]. Adv Chronic Kidney Dis, 2008, 15(4):355-362. |
| [1] | 沈连军, 吴蔚, 吉薇, 王红, 孙幸, 施青青, 孙梅, 顾健, 倪军. 急性粒-单核细胞白血病患者造血干细胞移植后微血栓形成凝血指标监测及治疗1例报告[J]. 诊断学理论与实践, 2024, 23(02): 180-183. |
| [2] | 王珏 刘海峰 王旭东 杜博帆 王海宁 黄伟 章一新. 彩色多普勒超声和 CT 血管造影技术在下肢穿支皮瓣临床应用中的对比研究[J]. 组织工程与重建外科杂志, 2021, 17(5): 400-. |
| [3] | 孙甜甜, 叶宝英, 杨钰, 牛建梅. 彩色多普勒超声与磁共振成像在凶险型前置胎盘及合并胎盘植入产前诊断中的应用及漏诊分析[J]. 诊断学理论与实践, 2021, 20(02): 173-177. |
| [4] | 刘方韬, 齐晓凤, 徐学勤, 黄娟, 董海鹏, 倪根雄, 周雯, 孔德艳. 非增强磁共振血管成像在肾动脉狭窄评估方面的价值研究[J]. 诊断学理论与实践, 2019, 18(1): 72-76. |
| [5] | 黄海峡1,吴志远2,徐国厚1. 多排螺旋CT及彩色多普勒超声在布加综合征分型诊断中的应用价值[J]. 上海交通大学学报, 2017, 51(5): 636-. |
| [6] | 袁宇雯,昝涛,李青峰. 穿支皮瓣术前血管定位技术的研究进展[J]. 组织工程与重建外科杂志, 2014, 10(5): 285-288. |
| [7] | 王慧, 孙立群, 牛建梅, 陈炯, 周雷平, 陈瑞玉, 李丽蟾,. 彩色多普勒超声多切面联合显示法在高危人群产前胎儿心脏筛查中的诊断价值[J]. 诊断学理论与实践, 2014, 13(05): 515-518. |
| [8] | 周春, 周建桥, 詹维伟, 陈林, 戴军, 刘振华, 周伟, 柳俊, 董屹婕,. 彩色多普勒超声和超声造影在青春后期及成人睾丸扭转诊断中的价值[J]. 诊断学理论与实践, 2013, 12(03): 343-346. |
| [9] | 冯睿, 魏小龙, 赵志青, 包俊敏, 冯翔, 曲乐丰, 陆清声, 陆华, 景在平,. 采用单条大隐静脉行腹主动脉-双侧肾动脉旁路术治疗大动脉炎性肾动脉狭窄[J]. 外科理论与实践, 2011, 16(02): 151-154. |
| [10] | 何清, 何奔,. 肾动脉狭窄的诊断和治疗进展[J]. 内科理论与实践, 2009, 4(06): 511-513. |
| [11] | 窦艳娜, 刘章锁,. 动脉粥样硬化性肾动脉狭窄的诊断方法及精确性[J]. 诊断学理论与实践, 2007, 6(06): 558-560. |
| [12] | 王琴, 倪兆慧, 牟姗, 周文彦, 俞赞喆, 朱彩霞, 李萍,. 慢性肾脏病透析前患者的甲状旁腺功能异常及其意义[J]. 诊断学理论与实践, 2006, 5(06): 503-506. |
| [13] | 沈卫峰,. 重视心脏病学与肾脏病学的相互联系[J]. 诊断学理论与实践, 2006, 5(03): 197-198. |
| [14] | 姜志荣,吕慧霞,安秀丽. 彩色多普勒超声对主动脉窦瘤破裂的诊断价值[J]. 诊断学理论与实践, 2004, 3(03): 79-80. |
| [15] | 田路. 无创伤影像学检查诊断肾动脉狭窄评价[J]. 外科理论与实践, 2003, 8(04): 356-357+360. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||