外科理论与实践 ›› 2023, Vol. 28 ›› Issue (05): 454-462.doi: 10.16139/j.1007-9610.2023.05.11
刘萌a, 徐文a, 戴赟麒a, 谭若铭a, 刘嘉琳b, 顾飞飞c, 陈尔真d, 王晓丽a, 瞿洪平a, 邱毓祯a( )
)
收稿日期:2023-08-16
出版日期:2023-09-25
发布日期:2024-01-04
通讯作者:
邱毓祯
E-mail:qyz11849@rjh.com.cn
LIU Menga, XU Wena, DAI Yunqia, TAN Ruominga, LIU Jialinb, GU Feifeic, CHEN Erzhend, WANG Xiaolia, QU Hongpinga, QIU Yuzhena()
Received:2023-08-16
Online:2023-09-25
Published:2024-01-04
摘要:
目的:分析真实世界中重症病人耐碳青霉烯类肺炎克雷伯菌血流感染(carbapenem-resistant Klebsiella pneumonia bloodstream infection, CRKP-BSI)的死亡危险因素以及治疗效果,为病人个体化治疗提供参考。方法:回顾性分析2016年7月至2020年6月我院重症监护病房内81例CRKP-BSI病人的临床特征,评估死亡危险因素及不同抗菌药物方案的治疗效果。结果:CRKP-BSI以腹腔来源和呼吸道来源的占比较多,分别为56.79%(46例)、22.22%(18例)。CRKP-BSI病人28 d死亡率及住院死亡率分别为54.32%(44例)、65.43%(53例)。多因素回归分析结果提示入院前患胆道疾病(P=0.026)、病人BSI发生时SOFA评分升高(P=0.006)为28 d死亡率独立危险因素。接受以替加环素为基础(44例)或以多黏菌素B(26例)为基础的抗生素治疗,两组28 d死亡率差异无统计学意义[56.82%(25/44)比57.69%(15/26), P=0.943]。根据病人的年龄(≤65岁比>65岁)、性别、体质量指数(≤25 kg/m2比 >25 kg/m2)、APACHE Ⅱ评分(≤20分比>20分)、肾脏替代治疗及机械通气的使用分为不同亚组,各亚组间死亡率差异无统计学意义。结论:SOFA评分及入院前胆道疾病病史是CRKP-BSI 28 d死亡率的危险因素。以替加环素为基础与以多黏菌素B为基础的抗菌药物治疗效果无差异。
中图分类号:
刘萌, 徐文, 戴赟麒, 谭若铭, 刘嘉琳, 顾飞飞, 陈尔真, 王晓丽, 瞿洪平, 邱毓祯. ICU病人耐碳青霉烯类肺炎克雷伯菌血流感染的危险因素与预后分析(附81例报告)[J]. 外科理论与实践, 2023, 28(05): 454-462.
LIU Meng, XU Wen, DAI Yunqi, TAN Ruoming, LIU Jialin, GU Feifei, CHEN Erzhen, WANG Xiaoli, QU Hongping, QIU Yuzhen. Risk factors and prognosis of carbapenem-resistant Klebsiella pneumoniae bloodstream infection in ICU patients: a report of 81 cases[J]. Journal of Surgery Concepts & Practice, 2023, 28(05): 454-462.
表1
病人临床特征及CRKP-BSI危重病人28 d全因死亡率相关因素分析[$\bar{x} \pm s$/M(P25,P75)/n(%)]
| Item | Total(n=81) | Non-surviver(n=44) | Surviver(n=37) | t/Z/χ2 value | P value |
|---|---|---|---|---|---|
| Demographic variable | |||||
| Age (years) | 58.12±17.52 | 62.73±14.66 | 52.65±19.20 | 2.68 | 0.009a) |
| Male sex [n(%)] | 63 (77.78) | 32(72.72) | 31(83.78) | 1.42 | 0.233b) |
| BMI (kg/m2) | 23.88(21.83, 27.63) | 24.79(18.62, 30.96) | 23.67(22.07, 27.32) | 791 | 0.827b) |
| NRS-2002 | 6(4, 6) | 6(4, 6) | 5(4, 6) | 675 | 0.170b) |
| Comorbidity | |||||
| Charlson comorbidity score | 2(1,4) | 3(1, 4) | 2(0, 6) | 674 | 0.178b) |
| Diabetes mellitus [n(%)] | 24(19.63) | 12(27.27) | 12(32.43) | 0.26 | 0.612c) |
| Chronic renal failure [n(%)] | 8(9.88) | 3(6.82) | 5(13.51) | 0.40 | 0.527c) |
| Chronic liver diseases [n(%)] | 1(1.23) | 1(2.27) | 0(0) | - | 1c) |
| Biliary tract disease [n(%)] | 10(12.35) | 9(20.45) | 1(2.7) | 4.33 | 0.038c) |
| Congestive heart failure [n(%)] | 2(2.47) | 2(4.55) | 0(0) | - | 0.498c) |
| COPD [n(%)] | 5(6.17) | 3(6.82) | 2(4.88) | 0 | 1c) |
| Malignancy [n(%)] | 13(16.05) | 7(15.91) | 6(16.22) | 0.00 | 0.97c) |
| Immunosupressiono [n(%)] | 8(9.88) | 3(6.82) | 5(13.51) | 0.4. | 0.527c) |
| Health-care exposure before hospitalization | |||||
| Antibiotic exposure (< 30 d) [n(%)] | 53(65.43) | 26(59.09) | 27(70.97) | 1.71 | 0.191c) |
| ICU admission(< 30 d) [n(%)] | 31(38.27) | 13(29.55) | 18(48.65) | 3.11 | 0.078c) |
| Surgery(< 30 d) [n(%)] | 16(19.75) | 7(15.91) | 9(24.32) | 0.90 | 0.343c) |
| Immunosuppressive therapy (< 3 m) [n(%)] | 9(11.11) | 3(6.82) | 6(16.22) | 0.97 | 0.324c) |
| Previous hospitalization (< 12 m) [n(%)] | 47(58.02) | 26(59.09) | 21(56.76) | 0.05 | 0.832c) |
| Length of stay before BSI | 23.00(13.00, 36.00) | 23.50(14.25, 39.50) | 23(9.00, 33.50) | 755 | 0.576b) |
| Source of infection [n(%)] | |||||
| Central line | 8(9.88) | 4(9.09) | 4(10.81) | 0.00 | 1c) |
| Urinary tract | 2(2.47) | 1(2.27) | 1(2.70) | - | 1c) |
| Intra-abdominal | 46(56.79) | 24(54.55) | 22(59.46) | 0.20 | 0.657c) |
| Respiratory | 18(22.22) | 11(25.00) | 7(18.92) | 0.43 | 0.512c) |
| Skin and soft tissue | 3(3.70) | 2(4.55) | 1(2.70) | 0.00 | 1c) |
| Cardio-vascular system infection | 1(1.23) | 1(2.27) | 0 | - | 1c) |
| Primary | 3(3.70) | 1(2.27) | 2(5.41) | 0.02 | 0.878c) |
| Severity of illness at BSI onset | |||||
| Biomarker at BSI onset | |||||
| PCT (ng/L) | 2.99(0.77, 7.95) | 3.86 (1.70, 7.95) | 1.33(0.46, 8.59) | 501 | 0.033b) |
| CRP (mg/L) | 124.54±83.45 | 137.65±82.03 | 112.91±83.10 | 1.28 | 0.239a) |
| Organ dysfunction at BSI onset | |||||
| AKI [n(%)] | 42(51.85) | 29(65.91) | 13(35.14) | 7.62 | 0.006c) |
| RRT [n(%)] | 29(35.80) | 20(45.45) | 9(24.32) | 3.90 | 0.048c) |
| Septic shock [n(%)] | 61(75.31) | 41(93.18) | 20(54.05) | 16.55 | <0.001c) |
| mechancal ventilation [n(%)] | 65(80.25) | 38(86.36) | 27(72.97) | 2.27 | 0.132c) |
| APACHE Ⅱ score at BSI onset | 24(18, 28) | 27(22, 29) | 19(14, 26) | 426.50 | <0.001b) |
| SOFA score at BSI onset | 8(6, 11) | 9(8, 13) | 6(3, 8) | 360.60 | <0.001b) |
| PBS | 4(2, 5) | 4(3, 6) | 3(1, 4) | 512.50 | 0.004b) |
| Outcomes | |||||
| Length of hospital stay(d) | 55.00(31.00, 86.50) | 36.00(25.25, 60.50) | 80.00(11.51, 48.50) | 299 | <0.001b) |
| Length of stay in ICU(d) | 42.00(24.00, 79.00) | 28.50(18.25, 51.25) | 65.00(44.00, 102.50) | 378.50 | <0.001b) |
表2
CRKP-BSI危重病人28 d全因死亡率的多因素Lo-gistic回归分析
| Item | OR (95 CI%) | P value |
|---|---|---|
| Biliary tract disease before admiccion | 62.86(1.66, 2 387.96) | 0.026 |
| SOFA score at BSI onset | 1.36(1.09, 1.71) | 0.006 |
| Length of hospital stay | 0.952(0.93,0.98) | <0.001 |
表3
CRKP-BSI病人抗菌药物方案
| Antimicrobial regimen | Total (n=81) | Death in 28-day | P value |
|---|---|---|---|
| Tigecycline-based regimens | 44 | 25(56.82) | 0.715 |
| Polymyxin B-based regimens | 26 | 15(57.69) | |
| Other regimens | 11 | 4 (36.36) | |
| Tigecycline-based regimens | 44 | 25(56.82) | |
| Tigecycline monotherapy | 4 | 4(100) | |
| Tigecycline + Carbapenem | 27 | 15(55.55) | |
| Tigecycline + Amikacin | 2 | 0 | |
| Tigecycline + Fosfomycin | 1 | 1(100) | |
| Tigecycline + Sulfamethoxazole | 2 | 1(50) | |
| Tigecycline + Carbapenem + Amikacin | 2 | 1(50) | |
| Tigecycline + Carbapenem + Fosfomycin | 3 | 2(66.67) | |
| Tigecycline + Carbapenem + Sulfamethoxazole | 2 | 0 | |
| Tigecycline + Carbapenem + Amikacin + Fosfomycin | 1 | 1(100) | |
| Polymyxin B-based regimens | 26 | 14(53.85) | |
| Polymyxin B monotherapy | 1 | 0 | |
| Polymyxin B + Carbapenem | 13 | 8(61.54) | |
| Polymyxin B + Fosfomycin | 2 | 0 | |
| Polymyxin B + Tigecycline | 4 | 2(50) | |
| Polymyxin B + Tigecycline + Carbapenem | 3 | 2(66.67) | |
| Polymyxin B + Carbapenem + Fosfomycin | 1 | 1(100) | |
| Polymyxin B + Ceftazidime-Avibactam | 2 | 1(50) | |
| Other regimens | 11 | 4(36.36) | |
| Ceftazidime-Avibactam monotherapy | 1 | 0 | |
| Cefoperazone + Fosfomycin | 2 | 0 | |
| Carbapenem + Fosfomycin | 2 | 1(50) | |
| Carbapenem + Amikacin | 3 | 2(66.67) | |
| Carbapenem + Sulfamethoxazole | 1 | 0 | |
| Ceftazidime-Avibactam + Amikacin | 1 | 1(100) | |
| Cefoperazone-sulbactam + Fosfomycin | 1 | 0 |
表4
替加环素组与多黏菌素B组的一般资料和临床特征比较[$\bar{x} \pm s$/M(P25,P75)/n(%)]
| Item | Tigecycline-based regimens (n=44) | Polymyxin B-based regimens (n=26) | t/Z/χ2 value | P value |
|---|---|---|---|---|
| Demographic variables | ||||
| Age (years) | 55.73 | 64.15 | -2.08 | 0.041a) |
| Male sex [n(%)] | 39(88.64) | 16(61.54) | 7.13 | 0.008c) |
| Body mass index (kg/m2) | 25.51 | 23.60 | 1.61 | 0.112a) |
| NRS-2002 | 5(4, 6) | 6(4, 6) | 0.25 | 0.303b) |
| Comorbidities | ||||
| Charlson comorbidity index | 2(0, 4) | 3(1.75, 4.25) | 0.25 | 0.125b) |
| Diabetes mellitus [n(%)] | 12(27.27) | 8(30.77) | 0.1. | 0.754c) |
| Chronic renal failure [n(%)] | 4(9.09) | 3(11.54) | 0.00 | 1.0c) |
| Chronic liver diseases [n(%)] | 0 | 1(3.85) | - | 0.371c) |
| Biliary tract disease [n(%)] | 4(9.09) | 6(23.08) | 1.59 | 0.207c) |
| Congestive heart failure [n(%)] | 0 | 2(7.69) | - | 0.135c) |
| COPD [n(%)] | 3(6.82) | 1(3.85) | 0.00 | 1.0c) |
| Malignancy [n(%)] | 6(13.64) | 6(23.08) | 0.47 | 0.494c) |
| Immunosuppression [n(%)] | 1(2.27) | 3(11.54) | 1.17 | 0.280c) |
| Health-care exposure before hospitalization [n(%)] | ||||
| Antibiotic exposure (< 30 d) | 28(63.64) | 18(69.23) | 0.23 | 0.634c) |
| ICU admission (< 30 d) | 17(38.64) | 10(38.46) | 0.00 | 0.988c) |
| Surgery (< 30 d) | 8(18.18) | 6(23.08) | 0.25 | 0.621c) |
| Immunosuppressive therapy (< 3 months) | 2(4.55) | 3(11.54) | 0.38 | 0.537c) |
| Previous hospitalization (< 12 months) | 29(65.12) | 12(46.15) | 2.63 | 0.105c) |
| Source of infection [n(%)] | ||||
| Central line | 5(11.36) | 2(7.69) | 0.01 | 0.934c) |
| Urinary tract | 0 | 1(3.85) | - | 0.371c) |
| Intra-abdominal | 28(63.63) | 12(46.15) | 2.04 | 0.153c) |
| Respiratory | 7(15.91) | 9(34.62) | 3.24 | 0.072c) |
| Skin and soft tissue | 2(4.55) | 1(3.85) | 0.00 | 1c) |
| Cardio-vascular system infection | 1(2.27) | 0 | - | 1c) |
| Primary | 1(2.27) | 1(3.85) | - | 1c) |
| Severity of illness at BSI onset | ||||
| Biomarker at BSI onset | ||||
| PCT (ng/L) | 2.55(0.89, 7.95) | 3.96(0.81, 14.59) | 1.64 | 0.635b) |
| CRP (mg/L) | 133.39 | 137.78 | -0.20 | 0.842a) |
| Organ dysfunction at BSI onset | ||||
| AKI [n(%)] | 24(54.55) | 15(57.69) | 0.07 | 0.798c) |
| RRT [n(%)] | 17(38.63) | 10(38.46) | 0.00 | 0.998c) |
| Septic shock [n(%)] | 36(81.82) | 20(76.92) | 0.25 | 0.621c) |
| Mechanical ventilation [n(%)] | 39(88.64) | 20(76.92) | 0.92 | 0.336c) |
| APACHE Ⅱ score | 24.07 | 23.15 | 0.44 | 0.663a) |
| SOFA score | 8.00(6.00, 11.00) | 8.00(5.75, 11.25) | 0.02 | 0.864b) |
| Pitt bacteremia score | 4.00(3.00, 5.00) | 4.00(2.75, 6.00) | 0.136 | 0.712b) |
| Outcomes | ||||
| 28-day mortality [n(%)] | 25(56.82) | 15(57.69) | 0.01 | 0.943c) |
| In-hospital mortality [n(%)] | 29(65.91) | 18(69.23) | 0.08 | 0.775c) |
| Length of stay(d) | 63 | 69.88 | -0.63 | 0.529a) |
| Length of stay before BSI(d) | 23.00(12.00, 34.00) | 24.50(14.50, 54.50) | 0.46 | 0.429b) |
| Length of stay in ICU(d) | 41(26, 79) | 51(21, 81) | 0.25 | 0.822b) |
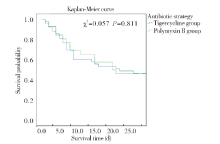
图1
替加环素组与多黏菌素B组28 d生存率的Kaplan-Meier分析

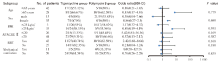
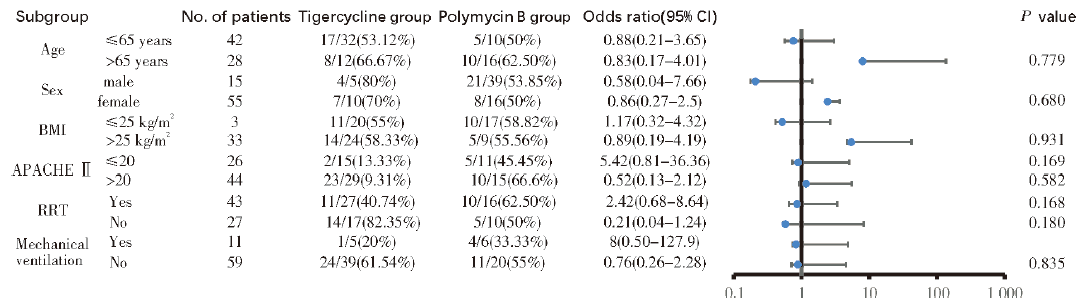
图2
不同亚组分析评估替加环素组与多黏菌素B组的疗效
| [1] |
BRINK A J. Epidemiology of carbapenem-resistant Gram-negative infections globally[J]. Curr Opin Infect Dis, 2019, 32(6):609-616.
doi: 10.1097/QCO.0000000000000608 pmid: 31567571 |
| [2] |
HU F, YUAN L, YANG Y, et al. A multicenter investigation of 2,773 cases of bloodstream infections based on China antimicrobial surveillance network (CHINET)[J]. Front Cell Infect Microbiol, 2022, 12:1075185.
doi: 10.3389/fcimb.2022.1075185 URL |
| [3] |
TIAN L, TAN R, CHEN Y, et al. Epidemiology of Klebsiella pneumoniae bloodstream infections in a teaching hospital: factors related to the carbapenem resistance and patient mortality[J]. Antimicrob Resist Infect Control, 2016, 5:48.
doi: 10.1186/s13756-016-0145-0 URL |
| [4] |
ZHEN X, LUNDBORG C S, SUN X, et al. Economic burden of antibiotic resistance in ESKAPE organisms: a systematic review[J]. Antimicrob Resist Infect Control, 2019, 8:137.
doi: 10.1186/s13756-019-0590-7 |
| [5] |
XIAO T, ZHU Y, ZHANG S, et al. A retrospective analysis of risk factors and outcomes of carbapenem-resistant Klebsiella pneumoniae bacteremia in nontransplant patients[J]. J Infect Dis, 2020, 221(Suppl 2):S174-S183.
doi: 10.1093/infdis/jiz559 URL |
| [6] |
LI Y, LI J, HU T, et al. Five-year change of prevalence and risk factors for infection and mortality of carbapenem-resistant Klebsiella pneumoniae bloodstream infection in a tertiary hospital in North China[J]. Antimicrob Resist Infect Control, 2020, 9(1):79.
doi: 10.1186/s13756-020-00728-3 |
| [7] |
KARAKONSTANTIS S, KRITSOTAKIS E I, GIKAS A. Treatment options for K. pneumoniae, P. aeruginosa and A. baumannii co-resistant to carbapenems, aminoglycosides, polymyxins and tigecycline: an approach based on the mechanisms of resistance to carbapenems[J]. Infection, 2020, 48(6):835-851.
doi: 10.1007/s15010-020-01520-6 |
| [8] |
TRECARICHI E M, TUMBARELLO M. Therapeutic options for carbapenem-resistant Enterobacteriaceae infections[J]. Virulence, 2017, 8(4):470-484.
doi: 10.1080/21505594.2017.1292196 URL |
| [9] |
GUAN X, HE L, HU B, et al. Laboratory diagnosis,clinical management and infection control of the infections caused by extensively drug-resistant Gram-negative bacilli: a Chinese consensus statement[J]. Clin Microbiol Infect, 2016, 22(Suppl 1):S15-S25.
doi: 10.1016/j.cmi.2015.11.004 URL |
| [10] |
GU F, HE W, XIAO S, et al. Antimicrobial resistance and molecular epidemiology of staphylococcus aureus causing bloodstream infections at Ruijin Hospital in Shanghai from 2013 to 2018[J]. Sci Rep, 2020, 10(1):6019.
doi: 10.1038/s41598-020-63248-5 pmid: 32265473 |
| [11] | Clinical and Laboratory Standards Institute (CLSI). Performance standards for antimicrobial susceptibility testing: twenty-four informational supplement[S]. CLSI document,2014,M100-S24. |
| [12] |
TIMSIT J F, RUPPÉ E, BARBIER F, et al. Bloodstream infections in critically ill patients: an expert statement[J]. Intensive Care Med, 2020, 46(2):266-284.
doi: 10.1007/s00134-020-05950-6 |
| [13] |
KELLUM J A, LAMEIRE N, KDIGO AKI Guideline Work Group. Diagnosis,evaluation,and management of acute kidney injury: a KDIGO summary (Part 1)[J]. Crit Care, 2013, 17(1):204.
doi: 10.1186/cc11454 URL |
| [14] |
SHEN L, LIAN C, ZHU B, et al. Bloodstream infections due to carbapenem-resistant Klebsiella pneumoniae: a single-center retrospective study on risk factors and therapy option[J]. Microb Drug Resist, 2021, 27(2):227-233.
doi: 10.1089/mdr.2019.0455 URL |
| [15] |
NIU T, LUO Q, LI Y, et al. Comparison of tigecycline or cefoperazone/sulbactam therapy for bloodstream infection due to carbapenem-resistant Acinetobacter baumannii[J]. Antimicrob Resist Infect Control, 2019, 8:52.
doi: 10.1186/s13756-019-0502-x |
| [16] | WANG X, WANG Q, CAO B, et al. Retrospective observational study from a chinese network of the impact of combination therapy versus monotherapy on mortality from carbapenem-resistant Enterobacteriaceae bacteremia[J]. Antimicrob Agents Chemother, 2018,21, 63(1):e01511-e015118. |
| [17] |
GUTIÉRREZ-GUTIÉRREZ B, SALAMANCA E, DE CUETO M, et al. Effect of appropriate combination therapy on mortality of patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae (INCREMENT): a retrospective cohort study[J]. Lancet Infect Dis, 2017, 17(7):726-734.
doi: 10.1016/S1473-3099(17)30228-1 URL |
| [18] |
SEO H, LEE S C, CHUNG H, et al. Clinical and microbiological analysis of risk factors for mortality in patients with carbapenem-resistant Enterobacteriaceae bacteremia[J]. Int J Antimicrob Agents, 2020, 56(4):106126.
doi: 10.1016/j.ijantimicag.2020.106126 URL |
| [19] |
STEWARDSON A J, MARIMUTHU K, SENGUPTA S, et al. Effect of carbapenem resistance on outcomes of bloodstream infection caused by Enterobacteriaceae in low-income and middle-income countries (PANORAMA): a multinational prospective cohort study[J]. Lancet Infect Dis, 2019, 19(6):601-610.
doi: 10.1016/S1473-3099(18)30792-8 URL |
| [20] |
TABAH A, KOULENTI D, LAUPLAND K, et al. Characteristics and determinants of outcome of hospital-acquired bloodstream infections in intensive care units: the EUROBACT international cohort study[J]. Intensive Care Med, 2012, 38(12):1930-1945.
doi: 10.1007/s00134-012-2695-9 pmid: 23011531 |
| [21] |
SOLOMKIN J S, RISTAGNO R L, DAS A F, et al. Source control review in clinical trials of anti-infective agents in complicated intra-abdominal infections[J]. Clin Infect Dis, 2013, 56(12):1765-1773.
doi: 10.1093/cid/cit128 pmid: 23463643 |
| [22] | LIANG C A, LIN Y C, LU P L, et al. Antibiotic strategies and clinical outcomes in critically ill patients with pneumonia caused by carbapenem-resistant Acinetobacter baumannii[J]. Clin Microbiol Infect, 2018, 24(8):908.e1-908.e7. |
| [23] |
GUTIÉRREZ-GUTIÉRREZ B, SALAMANCA E, DE CUETO M, et al. A predictive model of mortality in patients with bloodstream infections due to carbapenemase-producing Enterobacteriaceae[J]. Mayo Clin Proc, 2016, 91(10):1362-1371.
doi: 10.1016/j.mayocp.2016.06.024 URL |
| [24] |
FALCONE M, BASSETTI M, TISEO G, et al. Time to appropriate antibiotic therapy is a predictor of outcome in patients with bloodstream infection caused by KPC-producing Klebsiella pneumoniae[J]. Crit Care, 2020, 24(1):29.
doi: 10.1186/s13054-020-2742-9 |
| [25] |
MARTÍNEZ M L, FERRER R, TORRENTS E, et al. Impact of source control in patients with severe sepsis and septic shock[J]. Crit Care Med, 2017, 45(1):11-19.
pmid: 27611975 |
| [26] |
CHANG D, SHARMA L, DELA CRUZ C S, et al. Clinical epidemiology, risk factors, and control strategies of Klebsiella pneumoniae infection[J]. Front Microbiol, 12:750662.
doi: 10.3389/fmicb.2021.750662 URL |
| [27] |
TSUJI B T, POGUE J M, ZAVASCKI A P, et al. International consensus guidelines for the optimal use of the polymyxins: endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP)[J]. Pharmacotherapy, 2019, 39(1):10-39.
doi: 10.1002/phar.2019.39.issue-1 URL |
| [28] |
MEDEIROS G S, RIGATTO M H, FALCI D R, et al. Combination therapy with polymyxin B for carbapenemase-producing Klebsiella pneumoniae bloodstream infection[J]. Int J Antimicrob Agents, 2019, 53(2):152-157.
doi: 10.1016/j.ijantimicag.2018.10.010 URL |
| [29] |
DICKSTEIN Y, LELLOUCHE J, SCHWARTZ D, et al. Colistin resistance development following colistin-meropenem combination therapy versus colistin monotherapy in patients with infections caused by carbapenem-resistant organisms[J]. Clin Infect Dis, 2020, 71(10):2599-2607.
doi: 10.1093/cid/ciz1146 URL |
| [30] |
GIAMARELLOU H, POULAKOU G. Pharmacokinetic and pharmacodynamic evaluation of tigecycline[J]. Expert Opin Drug Metab Toxicol, 2011, 7(11):1459-1470.
doi: 10.1517/17425255.2011.623126 URL |
| [31] |
WANG J, PAN Y, SHEN J, et al. The efficacy and safety of tigecycline for the treatment of bloodstream infections: a systematic review and meta-analysis[J]. Ann Clin Microbiol Antimicrob, 2017, 16(1):24.
doi: 10.1186/s12941-017-0199-8 URL |
| [32] |
NI W, HAN Y, LIU J, et al. Tigecycline treatment for carbapenem-resistant Enterobacteriaceae infections: a systematic review and meta-analysis[J]. Medicine (Baltimore), 2016, 95(11):e3126.
doi: 10.1097/MD.0000000000003126 URL |
| [33] |
TUMBARELLO M, VIALE P, VISCOLI C, et al. Predictors of mortality in bloodstream infections caused by Klebsiella pneumoniae carbapenemase-producing K. pneumoniae: importance of combination therapy[J]. Clin Infect Dis, 2012, 55(7):943-950.
doi: 10.1093/cid/cis588 URL |
| [34] |
LIN Y T, SU C F, CHUANG C, et al. Appropriate treatment for bloodstream infections due to carbapenem-resistant Klebsiella pneumoniae and Escherichia coli: a nationwide multicenter study in Taiwan[J]. Open Forum Infect Dis, 2019, 6(2):ofy336.
doi: 10.1093/ofid/ofy336 URL |
| [35] |
ALRADDADI B M, SAEEDI M, QUTUB M, et al. Efficacy of ceftazidime-avibactam in the treatment of infections due to carbapenem-resistant Enterobacteriaceae[J]. BMC Infect Dis, 2019, 19(1):772.
doi: 10.1186/s12879-019-4409-1 |
| [36] |
TAMMA P D, AITKEN S L, BONOMO R A, et al. Infectious Diseases Society of America guidance on the treatment of extended-spectrum β-lactamase producing Enterobacterales (ESBL-E), carbapenem-resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa)[J]. Clin Infect Dis, 2021, 72(7):1109-1116.
doi: 10.1093/cid/ciab295 URL |
| [1] | 林瀚, 祖拜热古丽·麦麦提阿卜拉, 苏同轩. 肝素结合蛋白辅助临床血流感染诊断的价值[J]. 诊断学理论与实践, 2023, 22(02): 147-153. |
| [2] | 高玉莲, 冯耘, 倪磊. 糖尿病人群中耐药革兰阴性菌血流感染的研究进展[J]. 内科理论与实践, 2023, 18(02): 124-127. |
| [3] | 卞秀娟, 包志瑶, 陈虹, 承璐潇, 石宝平. 血流感染耐碳青霉烯类肺炎克雷伯菌患者的死亡危险因素分析[J]. 内科理论与实践, 2022, 17(01): 73-77. |
| [4] | 王雪洁, 陈孜瑾, 杜雯, 顾飞飞, 俞海瑾, 张文, 陈晓农. 不同病原菌致血流感染相关急性肾损伤的危险因素分析[J]. 内科理论与实践, 2021, 16(01): 22-26. |
| [5] | 中华医学会肠外肠内营养学分会. 新型冠状病毒肺炎重症病人的肠外肠内营养治疗专家建议[J]. 外科理论与实践, 2020, 25(01): 35-39. |
| [6] | 刘婧娴, 陈峰, 刘瑛. 分离胶促凝管法联合基质辅助激光解吸电离飞行时间质谱鉴定1例蜡样芽胞杆菌血流感染[J]. 诊断学理论与实践, 2019, 18(1): 107-108. |
| [7] | 沈晓红, 陈慧芬, 张军, 叶剑波, 张贤华. 2014年至2017年上海地区新生儿血流感染病原菌分布及其耐药性分析[J]. 诊断学理论与实践, 2018, 17(03): 266-271. |
| [8] | 郑宇, 李啸扬, 任雨虹, 李军民,. 初发急性白血病患者化学治疗后并发血流感染特点及危险因素分析[J]. 内科理论与实践, 2015, 10(05): 359-363. |
| [9] | 李彤, 宋加友, 何伟, 张彤彦, 许媛,. 改良B超胃窦单切面法对重症病人胃排空功能判断的价值[J]. 外科理论与实践, 2009, 14(06): 619-622. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||