外科理论与实践 ›› 2023, Vol. 28 ›› Issue (06): 540-550.doi: 10.16139/j.1007-9610.2023.06.010
祁洋, 姚文飞, 李谦益, 姚伟, 孔雷, 徐瑞云, 吴宇权, 李能平( )
)
收稿日期:2022-10-31
出版日期:2023-11-25
发布日期:2024-03-04
通讯作者:
李能平,E-mail:linengp@163.com
基金资助:
QI Yang, YAO Wenfei, LI Qianyi, YAO Wei, KONG Lei, XU Ruiyun, WU Yuquan, LI Nengping()
Received:2022-10-31
Online:2023-11-25
Published:2024-03-04
摘要:
目的: 应用网状荟萃分析,比较不同插管方法在内镜逆行胰胆管造影术(endoscopic retrograde cholangio-pancreatography, ERCP)困难胆管插管时的效果。方法: 选取英文发表的随机对照研究文献,对ERCP困难胆管插管时所采用的不同插管方法(早期或晚期针刀切开法、胰腺导丝辅助法、胰腺支架辅助法、经胰腺括约肌切开法、持续常规插管法)的效果,进行比较分析。主要观察指标为胆管插管成功率以及ERCP术后胰腺炎(post-ERCP pancreatitis,PEP)发生率。对不同插管方法的效果进行成对和网状荟萃分析,并根据累积排名曲线下面积(surface under the cumulative ranking curve, SUCRA)进行排名。结果: 18项研究符合要求,共2 033例病人。经胰腺括约肌切开法的胆管插管成功率显著高于持续常规插管法(RR=1.34, 95% CI:1.02~1.77)、胰腺导丝辅助法(RR=1.26, 95% CI:1.00~1.60)。根据SUCRA评分排名,经胰腺括约肌切开法胆道插管成功率最高,其次为早期针刀切开法。与持续常规插管法相比,只有早期针刀切开法可显著降低PEP发生率(RR=0.53, 95%CI:0.30~0.94)。与胰腺导丝辅助法相比,早期针刀切开法(RR=0.41, 95%CI:0.17~0.99)、经胰腺括约肌切开法(RR=0.49, 95%CI:0.25~0.96)的PEP发生率均显著降低。根据SUCRA评分排名,早期针刀切开法对降低PEP发生率效果最显著,其次为经胰腺括约肌切开法。结论: 经胰腺括约肌切开法可提高ERCP困难胆管插管时的胆管插管成功率;早期针刀切开法、经胰腺括约肌切开法可降低PEP发生率,可作为ERCP困难胆道插管时的选择方法。
中图分类号:
祁洋, 姚文飞, 李谦益, 姚伟, 孔雷, 徐瑞云, 吴宇权, 李能平. 不同插管方法在ERCP困难胆管插管的效果:系统评价和网状荟萃分析[J]. 外科理论与实践, 2023, 28(06): 540-550.
QI Yang, YAO Wenfei, LI Qianyi, YAO Wei, KONG Lei, XU Ruiyun, WU Yuquan, LI Nengping. Efficacy of different methods for difficult biliary cannulation in ERCP: systematic review and network meta-analysis[J]. Journal of Surgery Concepts & Practice, 2023, 28(06): 540-550.
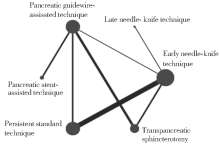
图1
6种插管方法的网状关系图
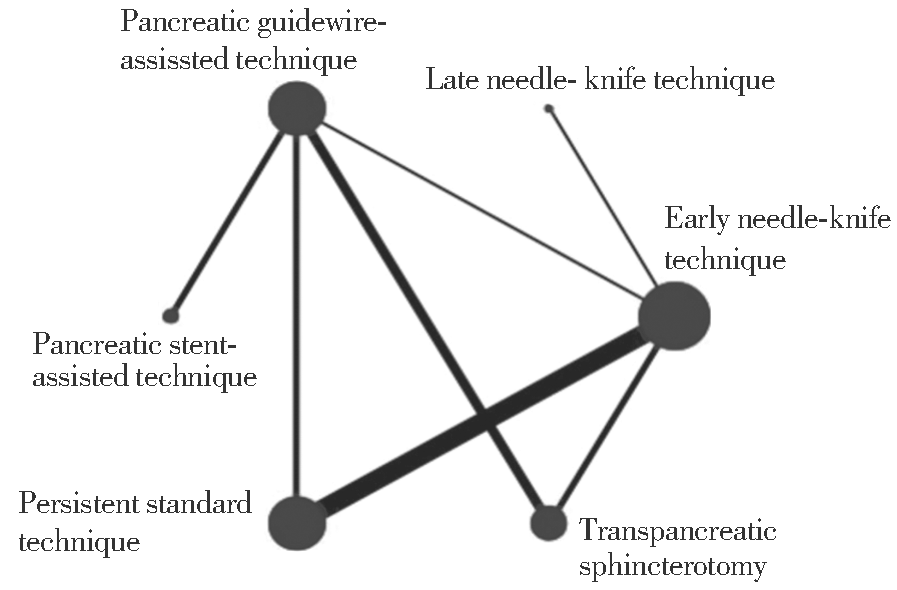
表1
纳入文献基本信息
| Serial number | Author (date of publication) | Experimental group | Control subject | Number of cases | Nation | Devise | Definition of difficult bile duct cannulation | Gender (M/F) | Age (y) | Etiology | Difficult cannulation rate (%) | Pancreatic duct stent application |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Maeda[ (2003) | Pancreatic guidewire assisted technique | Persistent standard technique | 27/26 | Japan | Single-center | 10 min | 23/30 | 64 vs. 64 | Unreported | 49.50 | Not use |
| 2 | Catalano[ (2004) | Transpancreatic sphincterotomy | Early needle- knife technique | 31/32 | United States of America | Single-center | 30 min; multiple intra-pancreatic ductal injections of contrast media | 38/25 | 68 | 11 cases of bile duct stones, 32 cases of obstructive jaundice, 15 cases of abdominal pain with abnormal liver function, 4 cases of SOD, 1 case of tumor | 1.40 | Selected cases |
| 3 | Tang[ (2005) | Early needle-knife technique | Persistent standard technique | 32/30 | Canada | Single-center | 12 min | 29/31 | 64.6 vs. 67.2 | There were 23 cases of choledochal dilatation, 11 cases of choledochal stone, 21 cases of tumor, 12 cases of biliary pancreatitis, 34 cases of abdominal pain, 34 cases of jaundice, 40 cases of liver function abnormality, 5 cases of cholangitis. | 9.70 | Not use |
| 4 | Zhou[ (2006) | Early needle-knife technique | Persistent standard technique | 43/48 | China | Single-center | 10 min; 3 accidental guidewire entries into pancreatic ducts | 55/36 | 62.7 vs. 64.3 | 28 cases of choledochal dilatation, 20 cases of choledochal stones, 15 cases of acute cholangitis, 25 cases of tumor, 3 cases of gastrectomy type B-Ⅱ | 9.60 | Not use |
| 5 | Manes[ | Early needle-knife technique | Persistent standard technique | 77/74 | Italy | Multicenter | 10 min; 5 accidental guidewire entries into pancreatic ducts | 98/53 | 66 vs. 65 | 72 cases of choledocholithiasis, 56 cases of tumors, 4 cases of benign bile duct stenosis, 5 cases of bile leakage, 2 cases of SOD cholecystitis, 5 cases of choledocholithiasis, 2 cases of choledochal cyst, 5 cases of recurrent pancreatitis | 9.50 | Not use |
| 6 | Cennamo[ | Early needle-knife technique | Late needle-knife technique | 36/32 | Italy | Single-center | 5 min; 3 accidental guidewire entries into pancreatic ducts | 31/37 | 68 vs. 69 | 47 cases of bile duct stones, 21 cases of tumor | 17.3 | Not use |
| 7 | Herreros de Tejada[ | Pancreatic guidewire-assisted technique | Persistent standard technique | 97/91 | Spain | Multicenter | 5 unsuccessful cannulations | 76/112 | 69.5 vs. 65.8 | 100 cases of bile duct stones, 38 cases of tumor, 9 cases of acute cholangitis, 5 cases of benign bile duct stenosis, 12 cases of others, 27 cases of abnormal liver function, 7 cases of SOD | 22.2 | Selected cases |
| 8 | Cote[ | Pancreatic guidewire-assisted technique | Pancreatic stent-assisted technique | 42/45 | United States of America | Multicenter | 6 min; 3 accidental guidewire entries into pancreatic ducts | Unreported | 58.1 vs. 57.4 | Unreported | 19.7 | Selected cases |
| 9 | Angsuwatcharakon[ | Pancreatic guidewire-assisted technique | Early needle- knife technique | 23/21 | Thailand | Single-center | 10 min | 23/21 | 66.1 vs. 64.1 | 23 cases of choledochal stones, 4 cases of gallbladder stones, 2 cases of Mirrizi's syndrome, 1 case of benign stenosis, 1 case of bile leakage, 13 cases of tumor | 8.2 | Not use |
| 10 | Swan[ | Early needle-knife technique | Persistent standard technique | 39/34 | Australia | Single-center | 5 min; 5 cannulations; 2 accidental guidewire entries into pancreatic ducts | 23/50 | 59 vs. 57 | 46 cases of choledocholithiasis, 8 cases of SOD, 6 cases of obstructive jaundice, 9 cases of benign bile duct stenosis, 4 cases of bile leaks | 15.7 | Selected cases |
| 11 | Yoo[ | Pancreatic guidewire-assisted technique | Transpancreatic sphincterotomy | 34/37 | South Korea (Republic of Korea) | Single-center | 10 min; 10 unsuccessful cannulation | 41/30 | 67 vs. 63.7 | 30 cases of choledochal stones, 13 cases of gallbladder stones, 18 cases of tumors, 10 cases of other | 7.4 | Not use |
| 12 | Zang[ | Transpancreatic sphincterotomy | Early needle-knife technique | 73/76 | China | Single-center | 10 min; 5 accidental guidewire entries into pancreatic ducts | 71/78 | 53.7 vs. 54.6 | 127 cases of choledocholithiasis, 17 cases of benign bile duct obstruction, 5 cases of bile leakage | 13.9 | Not use |
| 13 | Mariani[ | Early needle-knife technique | Persistent standard technique | 185/190 | Italy | Multicenter | 5 min; 3 accidental guidewire entries into pancreatic ducts | 165/210 | 70.4 vs. 68.2 | 223 cases of bile duct stones, 139 cases of tumors, 33 cases of cholangitis, 18 cases of SOD, 18 cases of benign bile duct stenosis, 12 cases of bile leaks, 11 cases of other | 9.5 | Not use |
| 14 | Zagalsky[ | Early needle-knife technique | Persistent standard technique | 50/51 | Argentina | Multicenter | 8 min; 3 accidental guidewire entries into pancreatic ducts | 31/70 | 52 vs. 49 | Choledocholithiasis 78% vs. 82.3%, tumor 22% vs. 17.7%, acute pancreatitis 6% vs. 13.7%, recurrent pancreatitis 2% vs. 2%, others 14% vs. 15.7 | 8.7 | Selected cases |
| 15 | Sugiyama[ | Transpancreatic sphincterotomy | Pancreatic guidewire-assisted technique | 34/34 | Japan | Single-center | 15 min; 3 accidental guidewire entries into pancreatic ducts | 37/31 | 69.8 vs. 67.3 | 18 cases of choledocholithiasis, 34 cases of tumor, 9 cases of benign bile duct stenosis, 3 cases of hepatocellular carcinoma, 1 case of SOD, 3 cases of other | 25.8 | All cases |
| 16 | Eminler[ | Pancreatic guidewire-assisted technique | Pancreatic stent-assisted technique | 50/50 | Istanbul | Single-center | 5 min; 5 accidental guidewire entries into pancreatic ducts | 40/60 | 56 vs. 52.9 | 76 cases of choledochal stones, 13 cases of tumors, 5 cases of benign strictures, and 6 cases of bile leaks | 11 | All cases |
| 17 | Tabak[ | Early needle knife technique | Transpancreatic sphincterotomy | 43/43 | China | Single-center | 5 min; 5 unsuccessful cannulations; 2 guidewire entries into pancreatic ducts | 51/35 | 61 vs. 59.4 | 57 cases of biliary stones, 16 cases of tumors, 18 cases of benign strictures, 3 cases of cholangitis, 5 cases of biliary pancreatitis | 12.8 | Selected cases |
| 18 | Kylanpaa[ | Transpancreatic sphincterotomy | Pancreatic guidewire-assisted technique | 104/99 | Finland, Denmark, Norway, Sweden | Multicenter | 5 min; 5 unsuccessful cannulations | 98/105 | 66 vs. 68 | 87 cases of choledocholithiasis, 91 cases of stricture, 12 cases of primary sclerosing cholangitis, and 17 cases of bile leakage, 20 cases of other | 17.1 | Selected cases |
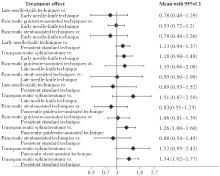
图2
不同方法插管成功率比较森林图
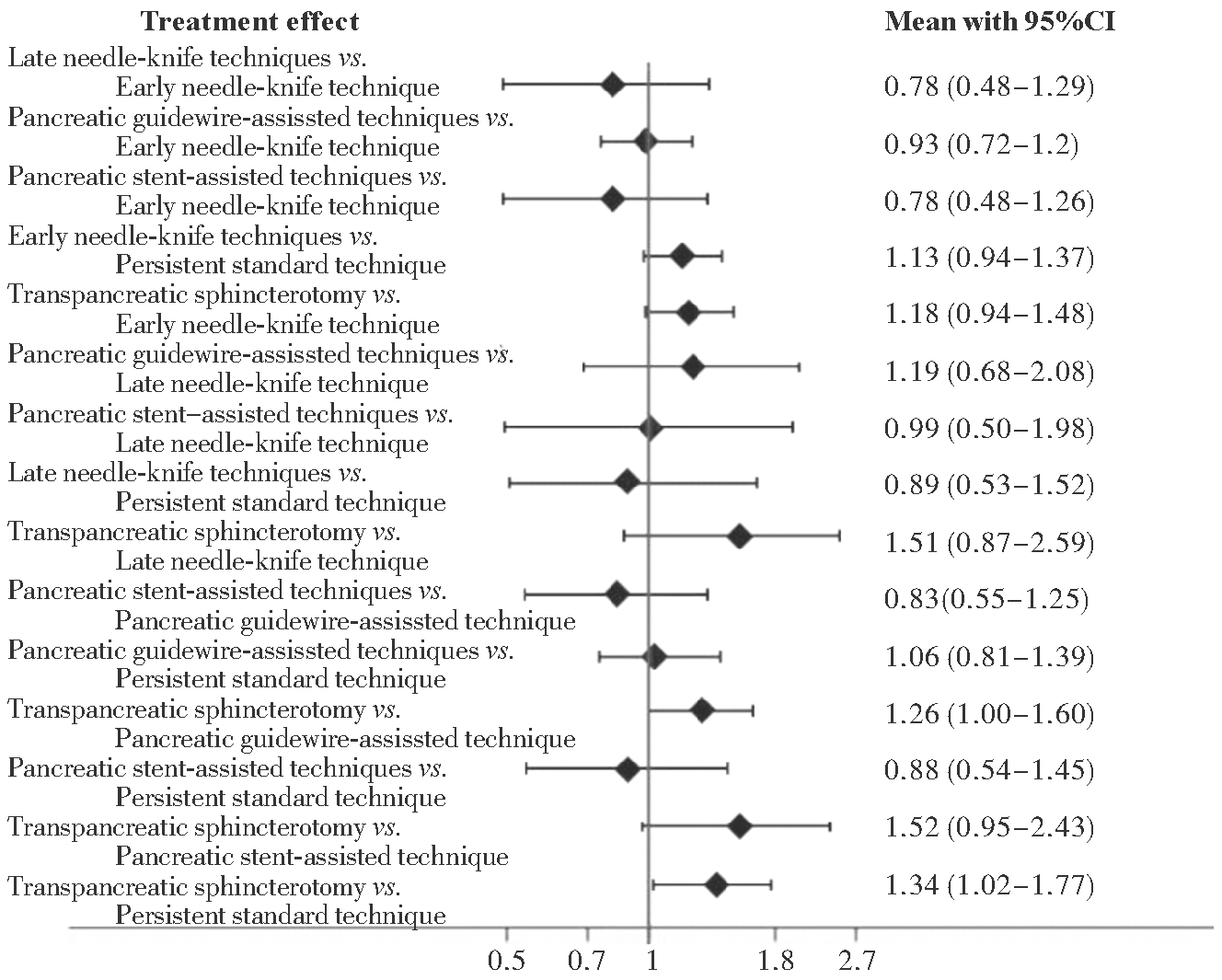
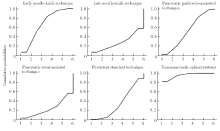
图3
不同方法插管成功率SUCRA
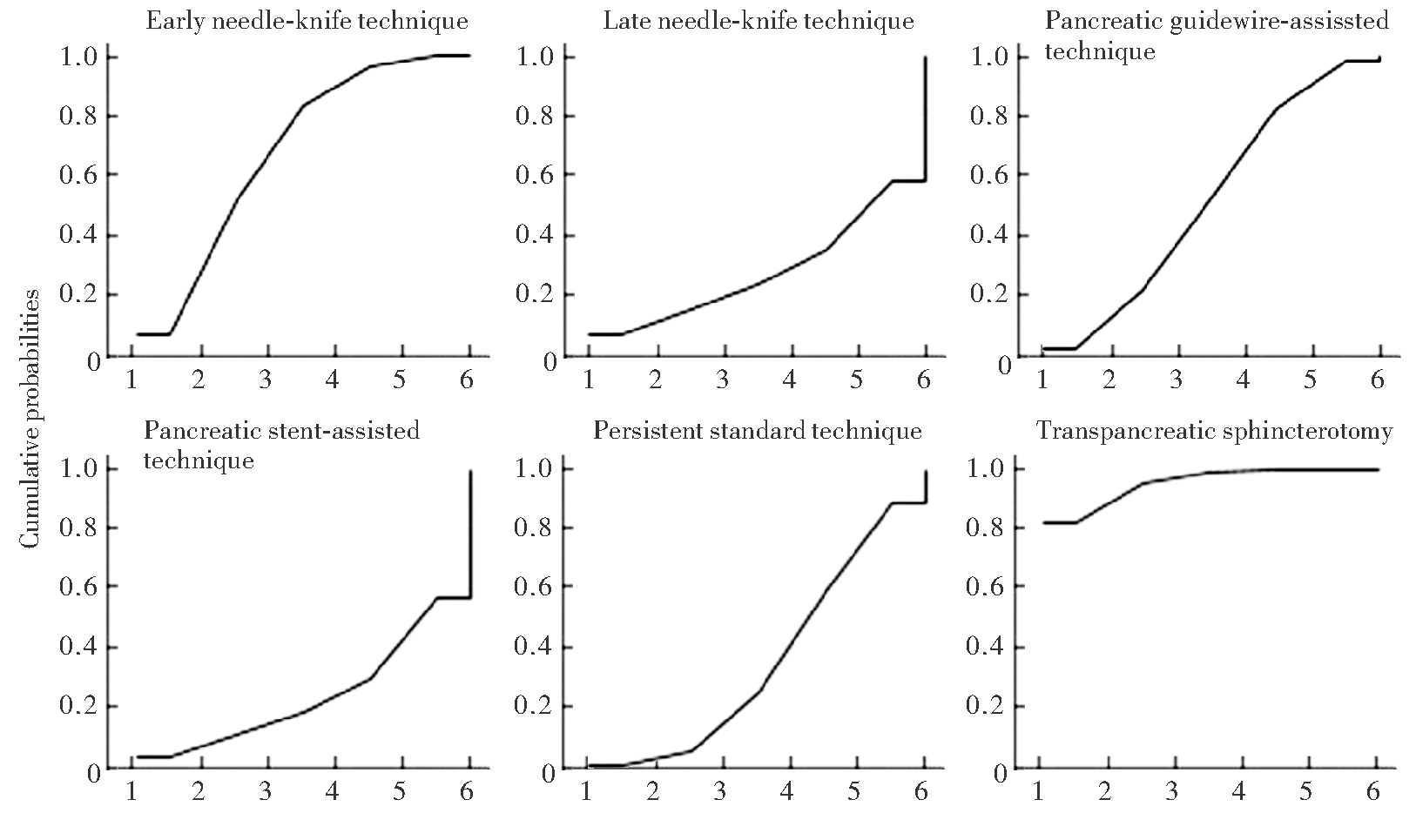
表2
不同方法插管成功率SUCRA评分及排名
| Cannulation techniques | SUCRA (%) | PrBest (%) | MeanRank |
|---|---|---|---|
| Transpancreatic sphincterotomy | 95.3 | 82.2 | 1.2 |
| Early needle-knife technique | 67.2 | 5.8 | 2.6 |
| Pancreatic guidewire-assissted technique | 50.7 | 1.7 | 3.5 |
| Standard technique | 35.8 | 0.7 | 4.2 |
| Late needle-knife technique | 27.2 | 6.3 | 4.6 |
| Pancreatic stent-assisted technique | 23.7 | 3.2 | 4.8 |
图4
不同方法PEP发生率比较森林图
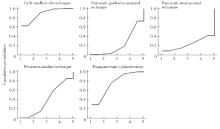
图5
不同方法PEP发生率SUCRA
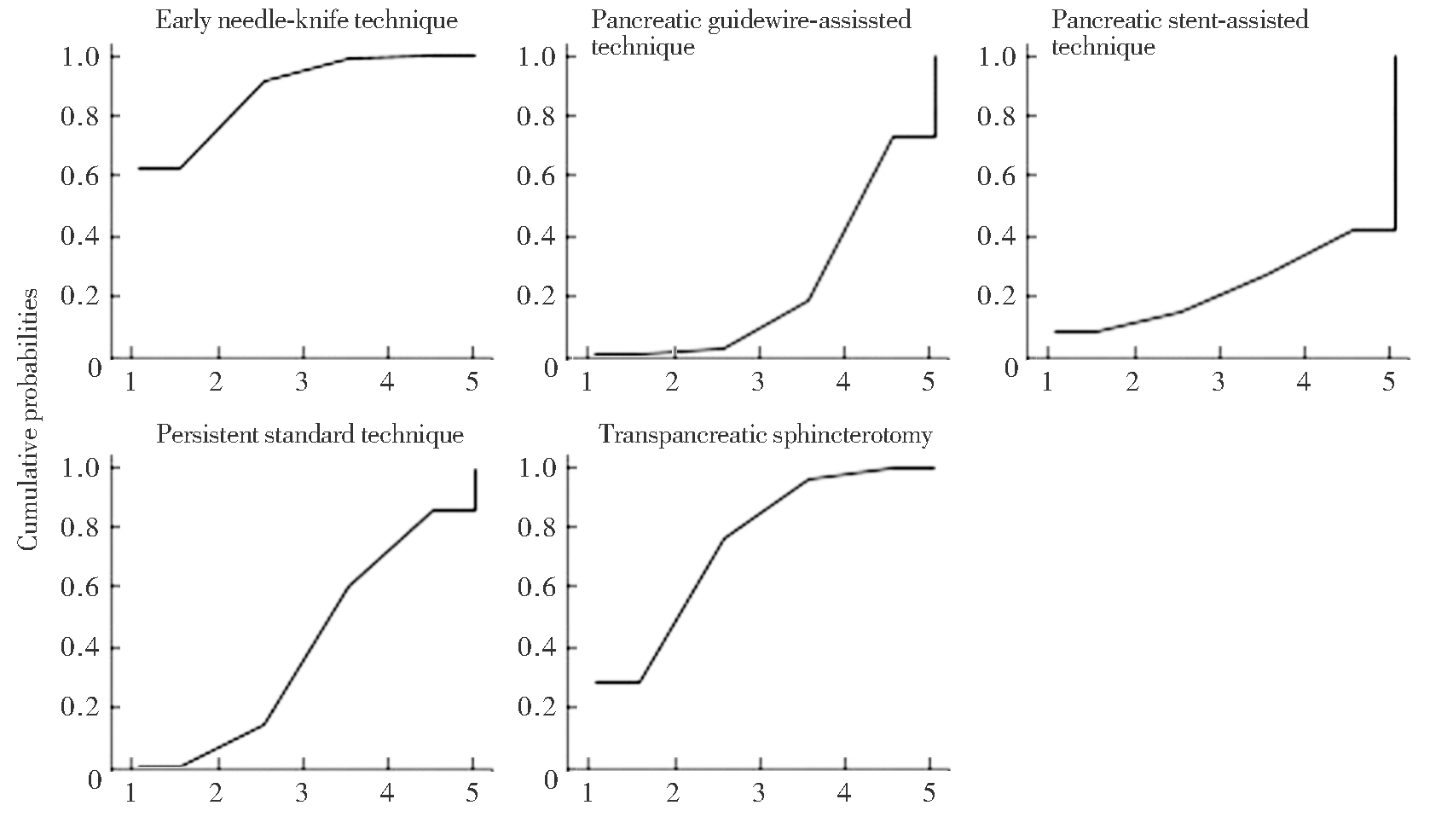
表3
不同方法PEP发生率SUCRA评分及排名
| Cannulation techniques | SUCRA (%) | PrBest (%) | MeanRank |
|---|---|---|---|
| Early needle-knife technique | 88 | 62.3 | 1.5 |
| Transpancreatic sphincterotomy | 75.2 | 28.5 | 2 |
| Persistent standard technique | 40.8 | 0.7 | 3.4 |
| Pancreatic guidewire-assissted technique | 23.2 | 0.2 | 4.1 |
| Pancreatic stent-assisted technique | 22.8 | 8.3 | 4.1 |
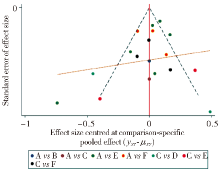
图6
插管成功率漏斗图
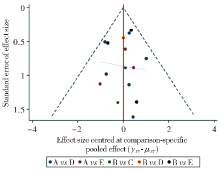
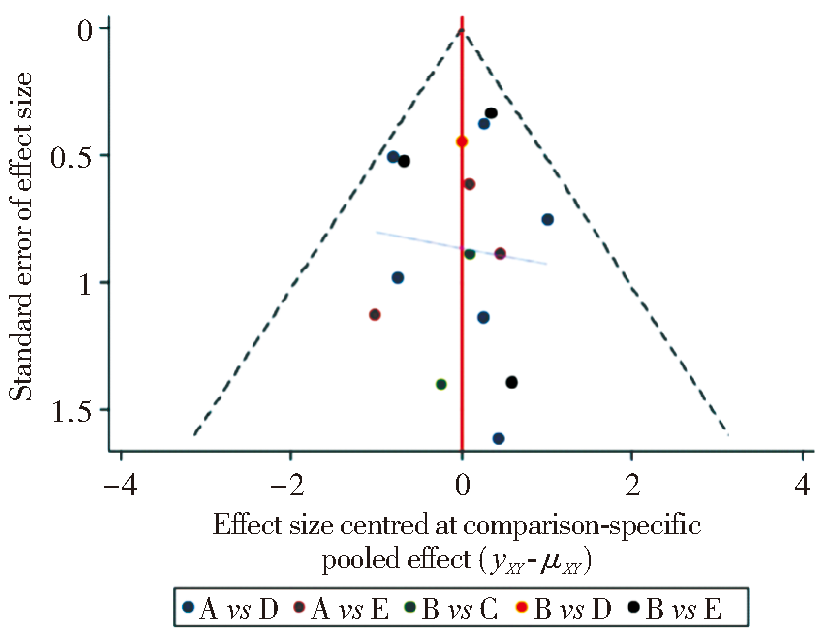
图7
PEP发生率漏斗图
| [1] | TSE F, YUAN Y, MOAYYEDI P, et al. Guidewire-assisted cannulation of the common bile duct for the prevention of post-endoscopic retrograde cholangiopancreatography (ERCP) pancreatitis[J]. Cochrane Database Syst Rev, 2012, 12(12):CD009662. |
| [2] |
WILLIAMS E J, TAYLOR S, FAIRCLOUGH P, et al. Are we meeting the standards set for endoscopy?Results of a large-scale prospective survey of endoscopic retrograde cholangiopancreatograph practice[J]. Gut, 2007, 56(6):821-829.
doi: 10.1136/gut.2006.097543 URL |
| [3] |
TESTONI P A, MARIANI A, AABAKKEN L, et al. Papillary cannulation and sphincterotomy techniques at ERCP:European Society of Gastrointestinal Endoscopy (ESGE) clinical guideline[J]. Endoscopy, 2016, 48(7):657-683.
doi: 10.1055/s-00000012 URL |
| [4] |
HALTTUNEN J, MEISNER S, AABAKKEN L, et al. Difficult cannulation as defined by a prospective study of the scandinavian association for digestive endoscopy (SADE) in 907 ERCPs[J]. Scand J Gastroenterol, 2014, 49(6):752-758.
doi: 10.3109/00365521.2014.894120 URL |
| [5] |
LIAO W C, ANGSUWATCHARAKON P, ISAYAMA H, et al. International consensus recommendations for difficult biliary access[J]. Gastrointest Endosc, 2017, 85(2):295-304.
doi: 10.1016/j.gie.2016.09.037 URL |
| [6] |
FREEMAN M L, DISARIO J A, NELSON D B, et al. Risk factors for post-ERCP pancreatitis: a prospective, multicenter study[J]. Gastrointest Endosc, 2001, 54(4):425-434.
doi: 10.1067/mge.2001.117550 pmid: 11577302 |
| [7] |
WANG P, LI Z S, LIU F, et al. Risk factors for ERCP-related complications: a prospective multicenter study[J]. Am J Gastroenterol, 2009, 104(1):31-40.
doi: 10.1038/ajg.2008.5 pmid: 19098846 |
| [8] |
PÉCSI D, FARKAS N, HEGYI P, et al. Transpancreatic sphincterotomy has a higher cannulation success rate than needle-knife precut papillotomy da meta-analysis[J]. Endoscopy, 2017, 49(9):874-887.
doi: 10.1055/s-0043-111717 URL |
| [9] |
PUHAN M A, SCHÜNEMANN H J, MURAD M H, et al. A GRADE Working Group approach for rating the qua-lity of treatment effect estimates from network meta-analysis[J]. BMJ, 2014, 349:g5630.
doi: 10.1136/bmj.g5630 URL |
| [10] |
HIGGINS J P, ALTMAN D G, GØTZSCHE PC, et al. The cochrane collaboration’s tool for assessing risk of bias in randomised trials[J]. BMJ, 2011, 343:d5928.
doi: 10.1136/bmj.d5928 URL |
| [11] |
MAEDA S, HAYASHI H, HOSOKAWA O, et al. Prospective randomized pilot trial of selective biliary cannulation using pancreatic guide-wire placement[J]. Endoscopy, 2003, 35(9):721-724.
pmid: 12929017 |
| [12] |
CATALANO M F, LINDER J D, GEENEN J E. Endoscopic transpancreatic papillary septotomy for inaccessible obstructed bile ducts:comparison with standard pre-cut papillotomy[J]. Gastrointest Endosc, 2004, 60(4):557-561.
doi: 10.1016/S0016-5107(04)01877-2 URL |
| [13] |
TANG S J, HABER G B, KORTAN P, et al. Precut papillotomy versus persistence in difficult biliary cannulation:a prospective randomized trial[J]. Endoscopy, 2005, 37(1):58-65.
doi: 10.1055/s-2004-826077 URL |
| [14] | ZHOU P H, YAO L Q, XU M D, et al. Application of needle-knife in difficult biliary cannulation for endoscopic retrograde cholangiopancreatography[J]. Hepatobiliary Pancreat Dis Int, 2006, 5(4):590-594. |
| [15] |
MANES G, DI GIORGIO P, REPICI A, et al. An analysis of the factors associated with the development of complications in patients undergoing precut sphincterotomy: a prospective, controlled, randomized, multicenter study[J]. Am J Gastroenterol, 2009, 104(10):2412-2417.
doi: 10.1038/ajg.2009.345 pmid: 19550413 |
| [16] |
CENNAMO V, FUCCIO L, REPICI A, et al. Timing of precut procedure does not influence success rate and complications of ERCP procedure: a prospective rando-mized comparative study[J]. Gastrointest Endosc, 2009, 69(3):473-479.
doi: 10.1016/j.gie.2008.09.037 URL |
| [17] |
HERREROS DE TEJADA A, CALLEJA J L, DÍAZ G, et al. Double-guidewire technique for difficult bile duct cannulation: a multicenter randomized,controlled trial[J]. Gastrointest Endosc, 2009, 70(4):700-709.
doi: 10.1016/j.gie.2009.03.031 URL |
| [18] |
COTÉ G A, MULLADY D K, JONNALAGADDA S S, et al. Use of a pancreatic duct stent or guidewire facilitates bile duct access with low rates of precut sphinctero-tomy: a randomized clinical trial[J]. Dig Dis Sci, 2012, 57(12):3271-3278.
doi: 10.1007/s10620-012-2269-2 URL |
| [19] |
ANGSUWATCHARAKON P, RERKNIMITR R, RIDTITID W, et al. Success rate and cannulation time between precut sphincterotomy and double-guidewire technique in truly difficult biliary cannulation[J]. J Gastroenterol Hepatol, 2012, 27(2):356-361.
doi: 10.1111/jgh.2012.27.issue-2 URL |
| [20] |
SWAN M P, ALEXANDER S, MOSS A, et al. Needle knife sphincterotomy does not increase the risk of pancrea-titis in patients with difficult biliary cannulation[J]. Clin Gastroenterol Hepatol, 2013, 11(4):430-436.
doi: 10.1016/j.cgh.2012.12.017 URL |
| [21] |
YOO Y W, CHA S W, LEE W C, et al. Double guidewire technique vs. transpancreatic precut sphincterotomy in difficult biliary cannulation[J]. World J Gastroenterol, 2013, 19(1):108-114.
doi: 10.3748/wjg.v19.i1.108 URL |
| [22] |
ZANG J, ZHANG C, GAO J. Guidewire-assisted transpancreatic sphincterotomy for difficult biliary cannulation: a prospective randomized controlled trial[J]. Surg Laparosc Endosc Percutan Tech, 2014, 24(5):429-433.
doi: 10.1097/SLE.0000000000000062 pmid: 24910935 |
| [23] |
MARIANI A, DI LEO M, GIARDULLO N, et al. Early precut sphincterotomy for difficult biliary access to reduce post-ERCP pancreatitis: a randomized trial[J]. Endoscopy, 2016, 48(6):530-535.
doi: 10.1055/s-0042-102250 pmid: 26990509 |
| [24] | ZAGALSKY D, GUIDI M A, CURVALE C, et al. Early precut is as efficient as pancreatic stent in preventing post-ERCP pancreatitis in high-risk subjectsda rando-mized study[J]. Rev Esp Enferm Dig, 2016, 108(9):558-562. |
| [25] | SUGIYAMA H, TSUYUGUCHI T, SAKAI Y, et al. Transpancreatic precut papillotomy versus double-guidewire technique in difficult biliary cannulation:prospective randomized study[J]. Endoscopy, 2018, 50(1):33-39. |
| [26] |
EMINLER A T, PARLAK E, KOKSAL A S, et al. Wire-guided cannulation over a pancreatic stent method increases the need for needle-knife precutting in patients with difficult biliary cannulations[J]. Gastrointest Endosc, 2019, 89(2):301-308.
doi: 10.1016/j.gie.2018.08.034 URL |
| [27] |
TABAK F, WANG F, JI G Z, et al. Propensity score-matched analysis for comparing transpancreatic sphincterotomy and needle-knife precut in difficult biliary cannulation[J]. Sci Rep, 2021, 11(1):6059.
doi: 10.1038/s41598-021-84655-2 pmid: 33723297 |
| [28] |
KYLÄNPÄÄ L, KOSKENSALO V, SAARELA A, et al. Transpancreatic biliary sphincterotomy versus double guidewire in difficult biliary cannulation:a randomized controlled trial[J]. Endoscopy, 2021, 53(10):1011-1019.
doi: 10.1055/a-1327-2025 URL |
| [29] |
PÉCSI D, FARKAS N, HEGYI P, et al. Transpancreatic sphincterotomy is effective and safe in expert hands on the short term[J]. Dig Dis Sci, 2019, 64(9):2429-2444.
doi: 10.1007/s10620-019-05640-4 |
| [30] |
CHEN J, WAN J H, WU D Y, et al. Assessing quality of precut sphincterotomy in patients with difficult biliary access: an updated metaanalysis of randomized controlled trials[J]. J Clin Gastroenterol, 2018, 52(7):573-578.
doi: 10.1097/MCG.0000000000001077 URL |
| [31] |
JANG S I, KIM D U, CHO J H, et al. Primary needle-knife fistulotomy versus conventional cannulation method in a high-risk cohort of post-endoscopic retrograde cho-langiopancreatography pancreatitis[J]. Am J Gastroenterol, 2020, 115(4):616-624.
doi: 10.14309/ajg.0000000000000480 URL |
| [32] | 李谦益, 姚文飞, 祁洋, 等. 胰管支架表面括约肌预切开在ERCP困难胆管插管中的应用效果[J]. 肝胆胰外科杂志, 2022, 34(3):129-133. |
| LI Q Y, YAO W F, QI Y, et al. Efficacy of precut over a pancreatic duct stent for difficult biliary cannulation in ERCP[J]. J Hepatopancreatobiliary Surg, 2022, 34(3):129-133. |
| [1] | 叶枫, 龚笑勇, 任家俊, 蔡强, 陈胜. ERCP在原发性肝癌围术期胆道并发症诊治中的应用[J]. 外科理论与实践, 2023, 28(04): 355-360. |
| [2] | 聂海行, 王帆, 王红玲, 赵秋. ERCP术后胰腺炎的危险因素及预防方法[J]. 外科理论与实践, 2023, 28(04): 310-315. |
| [3] | 董元航, 陈洁. 胰十二指肠切除术后胆胰疾病消化内镜介入策略[J]. 外科理论与实践, 2023, 28(04): 307-309. |
| [4] | 翁明哲, 王雪峰. 小肠镜ERCP在治疗胆肠吻合术后良性狭窄中的应用体会[J]. 外科理论与实践, 2023, 28(04): 296-299. |
| [5] | 王震宇. 胰腺良性疾病的内镜诊治[J]. 外科理论与实践, 2023, 28(04): 288-295. |
| [6] | 张玲, 邹多武. ERCP在慢性胰腺炎诊治中的作用[J]. 外科理论与实践, 2023, 28(04): 283-287. |
| [7] | 李文. 中国ERCP的发展及展望[J]. 外科理论与实践, 2023, 28(04): 279-282. |
| [8] | 胡贤荣, 杨档档, 吴军, 赵毅, 陈萃, 张婷, 胡冰. 经口胆道镜SpyGlass在肝门部不明原因胆管狭窄诊断中的应用[J]. 外科理论与实践, 2023, 28(04): 361-365. |
| [9] | 龚笑勇, 陈胜, 任家俊, 叶枫, 蔡强, 蔡琳燕, 刘远滨, 隋亮. SpyGlass内镜直视系统治疗内镜和外科手术治疗失败的困难胆管结石[J]. 外科理论与实践, 2022, 27(03): 215-220. |
| [10] | 翁昊, 翁明哲, 束翌俊, 顾钧, 张文杰, 王雪峰. 乳头球囊扩张及机械碎石先后顺序对ERCP治疗胆总管结石影响的前瞻性研究[J]. 外科理论与实践, 2022, 27(03): 210-214. |
| [11] | 翁昊, 王雪峰. 侧视镜治疗毕Ⅱ式胃切除术后胆管结石的要领与策略[J]. 外科理论与实践, 2022, 27(03): 203-209. |
| [12] | 张敏敏, 邹多武. 超声内镜在可疑胆总管结石诊治中的作用[J]. 外科理论与实践, 2022, 27(03): 193-197. |
| [13] | 胡冰. 困难胆管结石的ERCP诊治[J]. 外科理论与实践, 2022, 27(03): 189-192. |
| [14] | 石加利, 程思乐, 金杭斌, 张筱凤. ERCP联合SpyGlass DS直视下液电碎石治疗困难胆总管结石[J]. 外科理论与实践, 2022, 27(02): 165-168. |
| [15] | 胡刚峰, 黄侠. LC联合ERCP一期治疗胆囊结石合并肝外胆管结石与分期ERCP+LC手术疗效比较[J]. 外科理论与实践, 2021, 26(05): 437-440. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||