外科理论与实践 ›› 2024, Vol. 29 ›› Issue (05): 409-413.doi: 10.16139/j.1007-9610.2024.05.08
张丰哲, 童一苇, 陈小松( ), 沈坤炜()
), 沈坤炜()
收稿日期:2024-09-04
出版日期:2024-09-25
发布日期:2025-01-23
通讯作者:
陈小松,E-mail: chenxiaosong0156@hotmail.com;
ZHANG Fengzhe, TONG Yiwei, CHEN Xiaosong(), SHEN Kunwei()
Received:2024-09-04
Online:2024-09-25
Published:2025-01-23
Supported by:摘要:
目的:分析前哨淋巴结(SLN)阴性乳腺癌病人非前哨淋巴结(non-SLN, NSLN)转移的危险因素。方法:回顾性纳入2009年1月至2024年8月于我中心行全乳切除和前哨淋巴结活检的乳腺癌病人,在SLN阴性且行低位组淋巴结清扫的病人中,行NSLN转移相关危险因素单因素和多因素分析。结果:2 387例SLN阴性病人中,无NSLN转移者2 288例(95.9%),NSLN转移者99例(4.1%)。单因素及多因素分析显示:脉管侵犯(LVI)为SLN阴性病人NSLN转移的独立危险因素(13.5%比3.5%;OR=4.14,95%CI: 2.27~7.56,P<0.001);与非多中心性乳腺癌相比,多中心性乳腺癌病人具有较高NSLN转移风险的趋势(9.5%比4.1%;OR=2.08,95% CI: 0.90~4.81,P=0.089)。结论:SLN阴性病人中,存在LVI、多中心性乳腺癌者具有较高NSLN转移风险。
中图分类号:
张丰哲, 童一苇, 陈小松, 沈坤炜. 前哨淋巴结阴性乳腺癌病人非前哨淋巴结转移相关危险因素分析[J]. 外科理论与实践, 2024, 29(05): 409-413.
ZHANG Fengzhe, TONG Yiwei, CHEN Xiaosong, SHEN Kunwei. Analysis of risk factors for non-sentinel lymph node metastasis in patients with sentinel lymph node-negative breast cancer[J]. Journal of Surgery Concepts & Practice, 2024, 29(05): 409-413.
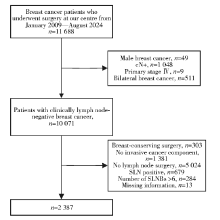
图1
筛选流程图
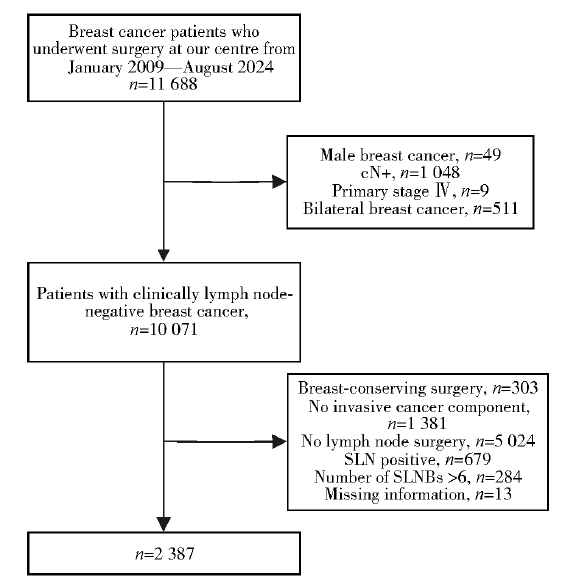
表1
SLN阴性病人NSLN转移相关危险因素单因素分析[n(%)]/M(范围)
| Characteristic | NSLN(-) (n=2 288) | NSLN(+) (n=99) | P value |
|---|---|---|---|
| Median Age(Range)(year) | 58(27-91) | 57(30-85) | 0.702 |
| Age(year) | |||
| ≤58 | 1 180(95.7) | 53(4.3) | |
| >58 | 1 108(96.0) | 46(4.0) | |
| Menopausal status | 0.650 | ||
| Premenopausal/ Perimenopause | 736(95.6) | 34(4.4) | |
| Postmenopausal | 1 552(96.0) | 65(4.0) | |
| BMI(kg/m2) | 0.626 | ||
| <25 | 1 668(96.0) | 70(4.0) | |
| ≥25 | 619(95.5) | 29(4.5) | |
| NA | 1(100.0) | 0 | |
| Tumor location | 0.025 | ||
| Non-multicentric | 1 752(95.9) | 74(4.1) | |
| Multicentric | 76(90.5) | 8(9.5) | |
| NA | 460(96.4) | 17(3.6) | |
| Tumor pathology | 0.010 | ||
| IDC | 1 890(95.4) | 91(4.6) | |
| ILC | 90(94.7) | 5(5.3) | |
| Others | 308(99.0) | 3(1.0) | |
| Tumor grade | 0.988 | ||
| Ⅰ-Ⅱ | 1 387(95.7) | 63(4.3) | |
| Ⅲ | 751(95.7) | 34(4.3) | |
| NA | 150(98.7) | 2(1.3) | |
| T stage | 0.064 | ||
| T1 | 1 406(96.4) | 52(3.6) | |
| T2 | 849(94.9) | 46(5.1) | |
| NA | 33(97.1) | 1(2.9) | |
| ER status | 0.045 | ||
| Negative | 675(97.1) | 20(2.9) | |
| Positive | 1 610(95.3) | 79(4.7) | |
| NA | 3(100.0) | 0 | |
| PR status | 0.096 | ||
| Negative | 906(96.7) | 31(3.3) | |
| Positive | 1 378(95.3) | 68(4.7) | |
| NA | 4(100.0) | 0 | |
| HER2 status | 0.088 | ||
| Negative | 1 575(96.3) | 60(3.7) | |
| Positive | 594(94.7) | 33(5.3) | |
| NA | 119(95.2) | 6(4.8) | |
| Ki-67(%) | 0.266 | ||
| <14 | 936(96.4) | 35(3.6) | |
| ≥14 | 1 349(95.5) | 64(4.5) | |
| NA | 3(100.0) | 0 | |
| Molecular classification | 0.167 | ||
| Luminal | 1 529(95.4) | 73(4.6) | |
| Basal-like | 273(97.8) | 6(2.2) | |
| HER2-enriched | 353(96.2) | 14(3.8) | |
| NA | 133(95.7) | 6(4.3) | |
| LVI | <0.001 | ||
| Negative | 2 153(96.5) | 78(3.5) | |
| Positive | 135(86.5) | 21(13.5) | |
| Number of dissected sentinel nodes | 0.065 | ||
| Median number(range) | 3(1-6) | 3(1-6) | |
| 1-2 | 595(94.6) | 34(5.4) | |
| ≥3 | 1 693(96.3) | 65(3.7) |
表2
SLN阴性NSLN转移的临床病理影响因素的多因素分析
| Characteristic | Odds ratio | P value | 95% CI | |
|---|---|---|---|---|
| Lower imit | Upper imit | |||
| Tumor location | 0.089 | |||
| Non-multicentric | 1 | |||
| Multicentric | 2.08 | 0.089 | 0.90 | 4.81 |
| Tumor pathology | 0.064 | |||
| IDC | 1 | |||
| ILC | 1.60 | 0.345 | 0.61 | 4.21 |
| Others | 0.29 | 0.038 | 0.09 | 0.94 |
| T stage | 0.495 | |||
| T1 | 1 | |||
| T2 | 1.18 | 0.495 | 0.73 | 1.90 |
| ER status | 0.243 | |||
| Negative | 1 | |||
| Positive | 1.64 | 0.243 | 0.72 | 3.76 |
| PR status | 0.669 | |||
| Negative | 1 | |||
| Positive | 1.18 | 0.669 | 0.55 | 2.51 |
| HER2 status | 0.174 | |||
| Negative | 1 | |||
| Positive | 1.49 | 0.174 | 0.84 | 2.64 |
| LVI | <0.001 | |||
| Negative | 1 | |||
| Positive | 4.14 | <0.001 | 2.27 | 7.56 |
| Number of dissected sentinel nodes | 0.387 | |||
| 1-2 | 1 | |||
| ≥3 | 0.80 | 0.387 | 0.48 | 1.34 |
| [1] | BRAY F, LAVERSANNE M, SUNG H, et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries[J]. CA Cancer J Clin, 2024, 74(3):229-263. |
| [2] |
CHANG J M, LEUNG J W T, MOY L, et al. Axillary nodal evaluation in breast cancer: state of the art[J]. Radiology, 2020, 295(3):500-515.
doi: 10.1148/radiol.2020192534 pmid: 32315268 |
| [3] | VERONESI U, PAGANELLI G, VIALE G, et al. A randomized comparison of sentinel-node biopsy with routine axillary dissection in breast cancer[J]. N Engl J Med, 2003, 349(6):546-553. |
| [4] | MANSEL R E, FALLOWFIELD L, KISSIN M, et al. Randomized multicenter trial of sentinel node biopsy versus standard axillary treatment in operable breast cancer: the ALMANAC Trial[J]. J Natl Cancer Inst, 2006, 98(9):599-609. |
| [5] |
HUNT K K, BALLMAN K V, MCCALL L M, et al. Factors associated with local-regional recurrence after a negative sentinel node dissection: results of the ACOSOG Z0010 trial[J]. Ann Surg, 2012, 256(3):428-436.
pmid: 22868365 |
| [6] | GALIMBERTI V, COLE B F, ZURRIDA S, et al. Axillary dissection versus no axillary dissection in patients with sentinel-node micrometastases (IBCSG 23-01): a phase 3 randomised controlled trial[J]. Lancet Oncol, 2013, 14(4):297-305. |
| [7] | HARLOW S P, KRAG D N, JULIAN T B, et al. Prerandomization Surgical Training for the National Surgical Adjuvant Breast and Bowel Project (NSABP) B-32 trial: a randomized phase Ⅲ clinical trial to compare sentinel node resection to conventional axillary dissection in clinically node-negative breast cancer[J]. Ann Surg, 2005, 241(1):48-54. |
| [8] |
VERONESI U, PAGANELLI G, VIALE G, et al. Sentinel-lymph-node biopsy as a staging procedure in breast cancer: update of a randomised controlled study[J]. Lancet Oncol, 2006, 7(12):983-990.
doi: 10.1016/S1470-2045(06)70947-0 pmid: 17138219 |
| [9] |
CANAVESE G, CATTURICH A, VECCHIO C, et al. Sentinel node biopsy compared with complete axillary dissection for staging early breast cancer with clinically negative lymph nodes: results of randomized trial[J]. Ann Oncol, 2009, 20(6):1001-1007.
doi: 10.1093/annonc/mdn746 pmid: 19174453 |
| [10] | ZAVAGNO G, DE SALVO G L, SCALCO G, et al. A randomized clinical trial on sentinel lymph node biopsy versus axillary lymph node dissection in breast cancer: results of the sentinella/GIVOM trial[J]. Ann Surg, 2008, 247(2):207-213. |
| [11] | BRIERLEY J D, GOSPODAROWICZ M K, WITTEKIND C. TNM classification of malignant tumours[M]. 8th ed. New Jersey: Wiley Blackwell, 2017. |
| [12] |
ELSTON C W, ELLIS I O. Pathological prognostic factors in breast cancer. i. the value of histological grade in breast cancer: experience from a large study with long-term follow-up[J]. Histopathology, 1991, 19(5):403-410.
doi: 10.1111/j.1365-2559.1991.tb00229.x pmid: 1757079 |
| [13] | KRAG D N, ANDERSON S J, JULIAN T B, et al. Technical outcomes of sentinel-lymph-node resection and conventional axillary-lymph-node dissection in patients with clinically node-negative breast cancer: results from the NSABP B-32 randomised phase Ⅲ trial[J]. Lancet Oncol, 2007, 8(10):881-888. |
| [14] | GOYAL A, NEWCOMBE R G, CHHABRA A, et al. Factors affecting failed localisation and false-negative rates of sentinel node biopsy in breast cancer-results of the ALMANAC validation phase[J]. Breast Cancer Res Treat, 2006, 99(2):203-208. |
| [15] |
LEE S A, LEE H M, LEE H W, et al. Risk factors for a false-negative result of sentinel node biopsy in patients with clinically node-negative breast cancer[J]. Cancer Res Treat, 2018, 50(3):625-633.
doi: 10.4143/crt.2017.089 pmid: 28759990 |
| [16] |
CHOK K S, SUEN D T, LIM F M, et al. Factors affecting false-negative breast sentinel node biopsy in Chinese patients[J]. ANZ J Surg, 2007, 77(10):866-869.
pmid: 17803550 |
| [1] | 徐旺旺1,2,许良凤1,2,刘宁徽3,律娜3. 基于多注意力卷积神经网络的乳腺癌组织学图像诊断[J]. J Shanghai Jiaotong Univ Sci, 2025, 30(1): 91-106. |
| [2] | 宋达疆, 张天怡, 王志远, 等. 分叶游离下腹部皮瓣移植乳房再造的血管吻合方式选择 [J]. 组织工程与重建外科杂志, 2024, 20(4): 428-. |
| [3] | 郝昆, 孙宇光, 王仁贵, 等. 抽吸减容术治疗乳腺癌术后上肢淋巴水肿[J]. 组织工程与重建外科杂志, 2024, 20(1): 69-. |
| [4] | 陆裕杰, 朱思吉. 《双磷酸盐和其他骨调节剂在乳腺癌辅助治疗中的应用:ASCO-OH(CCO)指南更新》解读[J]. 外科理论与实践, 2024, 29(05): 405-408. |
| [5] | 韩梦圆, 陈小松. 遗传性乳腺癌风险基因检测与咨询:NCCN指南解读与瑞金医院临床实践[J]. 外科理论与实践, 2024, 29(05): 401-404. |
| [6] | 笪倩, 阮淼, 费晓春, 王朝夫. 人工智能在乳腺癌病理诊断中的应用及研究展望[J]. 外科理论与实践, 2024, 29(05): 389-395. |
| [7] | 曹希, 骆勇超, 沈松杰. 适合中国女性的乳腺癌筛查策略[J]. 外科理论与实践, 2024, 29(05): 382-388. |
| [8] | 赵鑫, 高鹏, 陈洁. 机器人辅助手术系统在乳腺癌治疗中的应用及前景[J]. 外科理论与实践, 2024, 29(05): 376-381. |
| [9] | 唐筱璐, 华鑫, 曹璐, 陈佳艺. 21基因检测在早期乳腺癌辅助放疗中的应用[J]. 外科理论与实践, 2024, 29(03): 270-276. |
| [10] | 刘娟, 殷丽娟, 范德生. AR、SKP2、SOX10、PD-L1及TIL表达在三阴性乳腺癌中的意义[J]. 诊断学理论与实践, 2024, 23(02): 162-172. |
| [11] | 欧丹, 蔡钢, 陈佳艺. RAD51AP1基因表达在三阴性乳腺癌脑转移中的生物信息分析[J]. 诊断学理论与实践, 2024, 23(02): 146-154. |
| [12] | 任延鑫, 于岩, 徐可欣, 等.
放疗对乳腺癌术后假体和自体组织乳房再造影响的研究进展
[J]. 组织工程与重建外科杂志, 2023, 19(5): 511-. |
| [13] | 李慧, 尹昱, 李春晓, 等. 呼吸训练对乳腺癌相关淋巴水肿康复疗效的研究进展#br#[J]. 组织工程与重建外科杂志, 2023, 19(4): 430-. |
| [14] | 张莹莹, 李华, 管佳琴, 等.
乳腺癌患者术后早期上肢淋巴水肿的发生率及影响因素分析
[J]. 组织工程与重建外科杂志, 2023, 19(3): 242-. |
| [15] | 朱丹丽 鲍婉婷 魏昊 郭善禹.
乳腺癌术后乳房缺损修复的研究进展
[J]. 组织工程与重建外科杂志, 2023, 19(2): 201-. |
| 阅读次数 | ||||||
|
全文 |
|
|||||
|
摘要 |
|
|||||